


Guided Oral Hygiene: A Virtual Intervention to Improve Oral Health
Abstract
In the US, the adult population aged 65 and older is projected to outnumber the youth population in 2030 and will continue to substantially increase by 2060. As the older adult population continues to increase, so does the number of older adults who require long-term care (LTC). Adults aged 65 and older requiring LTC have a high incidence of poor oral health, which is exacerbated by medical conditions and medications compounding the problem. To improve the oral health of older adults in LTC facilities, medical and dental professionals must work together. The 2022 Surgeon General Report identified a need for medical and dental professionals to develop collaborative workforce models to address the poor oral health conditions plaguing adults aged 65 and older. The primary purpose of this article is to illustrate a workforce model that was effective in improving the oral health of adults aged 69 to 100 living in an LTC facility.
Citation: Ann Longterm Care. 2023. Published online September 18, 2023.
DOI:10.25270/altc.2023.09.003
There are an estimated 54 million adults aged 65 and older in the US.1,2 This population is projected to grow to 70 million in 2030 and 98.2 million in 2060.1,2 This trajectory of growth for older adults correlates to an increasing number of people requiring long-term care (LTC). The 2016 Vital and Health Statistics report estimated that 16.9% of adults aged 65 and older required LTC, including adult day care, residential care, hospice care, nursing home residence, and home health care.3 According to this projection of growth, an estimated 16 million older adults would require LTC in 2060.
The growing population of older adults in the US have multifactorial conditions, which often lead to significant oral health concerns. First, adults 65 and older are retaining more natural teeth than past generations. The 2022 Surgeon General Report found that 49% of older adults in 1960 were edentulous compared with 13% in 2014.4,5 Older adults with natural teeth have a two to three times higher risk of root caries, and 68% have chronic periodontitis.5-7 Second, 80% of adults aged 65 and older have chronic health conditions and 70% have at least two chronic conditions.4,8 As these health conditions progress, difficulty in self-oral hygiene care and accessing dental services may ensue. Additionally, nine out of every 10 adults aged 65 and older require medications for health conditions.9 Dry mouth (xerostomia) is a major side effect of many of these medications (Table 1). Older adults with dry mouth no longer have the natural benefits of saliva to maintain a healthy oral environment.10 The third contributing factor to poor oral health is the lack of insurance. Many older adults are insured by Medicare to cover medical expenses; however, 70.8% of adults aged 65 and older do not have dental insurance.11 Uninsured older adults are less likely to seek preventive dental care and often do not receive dental treatment until the oral condition becomes an emergency.4,11
Table 1. Common Medications With Xerostomia Side Effects
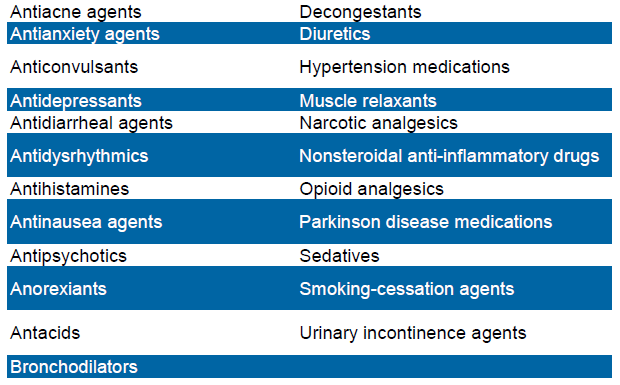
Source: Xerostomia. The American Academy of Oral Medicine. Updated October 15, 2015. Accessed July 10, 2022. https://www.aaom.com/index.php?option=com_content&view=article&id=107:xerostomia&catid=22:patient-condition-information&Itemid=120
The increasing older adult population and the multifactorial conditions leading to poor oral health is well documented in the 2020 Surgeon General Report.4 The Surgeon General also identified an oral-systemic link and correlated poor oral health in older adults with an increased risk for aspiration pneumonia, lack of glycemic control, increased cardiovascular risks, and a possible link to increased incidence of dementia.4,12 To improve overall health in adults aged 65 and older, the report identified the need for interprofessional collaboration and education to develop new workforce models.4 As the US population ages and more older adults require LTC, new interprofessional workforce models that include LTC facilities must be developed. Workforce models at a minimum should address the lack of daily oral hygiene care provided to older adults in LTC facilities. Well documented literature reports that residents in LTC facilities receive minimal to no daily oral care.13-15 Staff at these facilities identified common reasons for not providing daily oral hygiene services as lack of patient cooperation, lack of time, and having minimal education on daily oral care for dependent older adults.16-18 Based on these problems, the Guided Oral Hygiene program (GOHP) was created to focus on improving oral health for older adults in an assisted living center and to train staff to provide daily oral hygiene services.
Setting
The GOHP was implemented at a local memory care assisted living center. This facility is a three-building facility with a total of 46 beds. The staff included administration, certified nursing assistants (CNAs), and medical assistants (MAs) who provide LTC for residents aged 65 and older with mobility, memory, and medical conditions. The GOHP program was designed to address oral health concerns by virtually assisting caregivers to provide daily oral hygiene care for residents requiring assistance with daily tasks.
Prevention Efforts
Preparation for the Program
Information packets about the GOHP were sent via email to the assisted living center to gain written consent for residents to participate. Once consent forms were signed, Idaho State University (ISU) dental hygiene faculty were allowed to enter the assisted living center to expose intraoral photographs on the residents with consent to participate. Intraoral photographs were taken before starting the GOHP and again at the completion of the program. The intraoral photographs taken before the start of the program were used to determine the type of toothbrush and intraoral aids recommended for each participant. The recommended oral health care items were then placed in individualized dental hygiene kits created for residents participating in the program. The intraoral photographs were also used to score gingival inflammation using the Modified Gingival Index (MGI)19 and oral debris using the Simplified Oral Hygiene Index (SOH).20 MGI and SOH were recorded by two ISU faculty from the initial intraoral photographs and again with the final intraoral photographs. Before data collection, the two ISU faculty (principle investigator and co-investigator) were calibrated to establish intra-rater and inter-rater reliability.
Once the intraoral photographs were taken, the ISU faculty trained the staff to use the Zoom platform and how to access it on the iPad. Written instructions for Zoom and the iPad were also developed and left onsite for the staff to reference. In addition, a binder was created for staff to record information about recommended daily oral hygiene provided to each resident participant between live sessions.
Implementation of the Program
Live sessions took place once-weekly with each resident participant, the assisted living center staff, which included one administrator, one CNA or MA, and two dental hygiene faculty. Before the start of the session, the dental hygiene faculty informed the administrative staff of meeting ID and passcode for the Zoom live session to ensure the confidentiality and personal health information of participants.
The assisted living center staff logged into Zoom and rolled the iPad (mounted to a mobile stand) to the first resident participant’s room. On the other end of the live Zoom session, the dental hygiene faculty would admit the assisted living center staff into the Zoom waiting room for the live session. The staff member would then place the iPad into position to allow the dental hygiene faculty full view of the resident’s facial area. The staff member was then asked to brush the resident’s teeth while the dental hygiene faculty provided guidance on how to angle the toothbrush, the length of time to stay in each area, and the amount of pressure to use while brushing. Once brushing was completed, the staff member was asked to use the recommended interdental aid. The dental hygiene faculty watched the technique and made recommendations for modifications. After each resident completed the virtual session, the iPad was disinfected and rolled into the next resident participant’s room. This process continued until all resident participants completed their virtual session.
Between live sessions, CNA and MA staff provided daily oral hygiene to residents according to the recommendations identified during the live session. A binder was created for the assisted living center staff to record the oral hygiene care provided for each resident participant on a Daily Resident Hygiene form. The form included space to write the date for each day, indicate whether oral hygiene was successfully completed as recommended from the live session (yes or no), identify a list of problems for unsuccessful days, and record the name of the staff member. The administration staff ensured daily oral hygiene was recorded each day.
Study Limitations
The GOHP was an opt-in intervention, which required a signed consent form before participation. One barrier to gaining consent was the requirement of a legal guardian or power of attorney, who often lived out of state, to sign the resident’s consent forms. Another limitation was posed by residents with medical conditions or those who did not have enough teeth to participate (at least 8). Residents who were unable to participate and challenges with gaining consent resulted in a small sample size. However, the nonparticipating residents did benefit from the intervention indirectly; staff (identified within the GOHP survey) applied the skills learned from the GOHP to provide improved daily oral hygiene care for all residents.
Data Collection
The GOHP evaluation used a convenience sample size of residents (N=10) aged 69 to 100 with consent from their guardian, power of attorney, or durable or health power of attorney to participate in the program. Noninvasive intraoral photographs of the residents’ teeth were taken and evaluated by calibrated licensed dental hygienist at the beginning of the GOHP and again at the end of the program. Intraoral photographs were evaluated for oral debris, gingival inflammation, and dental referral needs. These parameters for oral health assessment follow the guidelines of the American Dental Hygienists Associations Standards for Clinical Dental Hygiene Practice.21
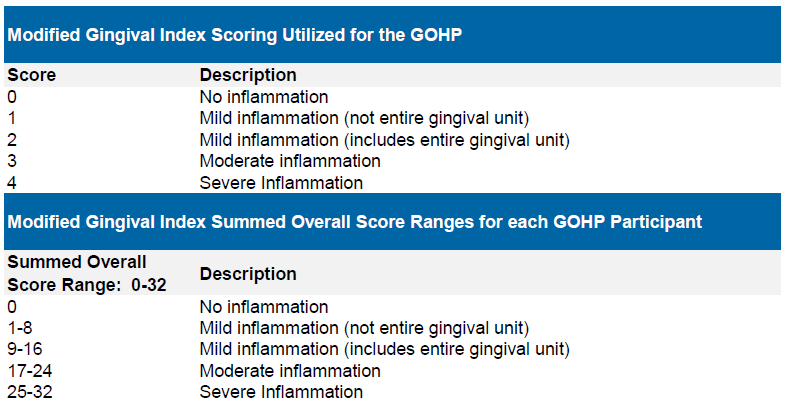
The Modified Gingival Index (MGI) was used to assess the facial (lip/cheek side) gingival inflammation of participating residents. MGI, as adapted from the Gingival Index, is used as means to measure gingival inflammation in public health and other settings when a recorded bleeding score is not possible, which was the case in GOHP.19 MGI scores were evaluated on eight selected teeth (one premolar, one canine, and two incisors) for each participant: See Table 2 for scoring.
Table 2
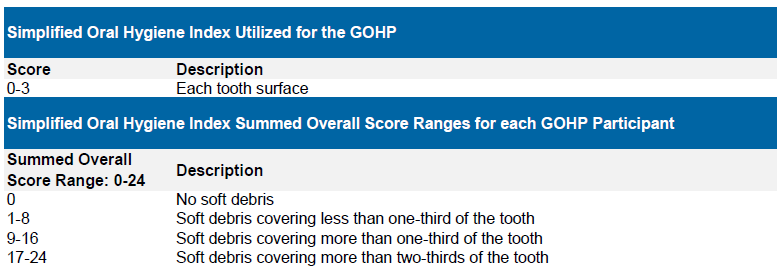
The Simplified Oral Hygiene Index20 evaluated the level of soft debris covering the facial/buccal tooth structure of eight teeth (one premolar, one canine, and two incisors on each dental arch). See Table 3 for scoring.
Table 3
Sample Description
For this program evaluation during the spring semester of 2021, the experimental group comprised a convenience sample of 10 assisted living center residents aged 69 to 100 who gave consent.
Inclusion Criteria
Residents with consent to participate in the program were required to have at least eight teeth, which include one premolar, one canine, and two incisors in each dental arch.
Exclusion Criteria
Residents could not participate in the program without consent, or if they did not have at least eight teeth, which must have included one premolar, one canine, and two incisors in each dental arch.
Clinical Outcomes
Modified Gingival Index and Simplified Oral Hygiene Index
The gingival inflammation scores of participating residents in an assisted living center were compared before the implementation of the GOHP and at the completion of the program. The mean initial MGI score was 27.60 (SD, 3.95) and the mean MGI at the completion of the program was 16.20 (SD, 5.67). The higher MGI scores represent greater gingival inflammation. The results of the correlated t test employing the bootstrap method showed a statistically significant difference in gingival inflammation from the beginning of the GOHP to the end of the program (P=.003) The mean difference was an improvement of inflammation demonstrated by a decrease of 11.4 score units. The effect size was large (Cohen’s d, 1.70).
The Wilcoxon Signed-Ranks Test for matched pairs was used to assess the oral debris of the ten residents participating in the GOHP. The mean results revealed a statistically significant decrease in oral debris after completion of the program; initial mean was 16.3 (SD, 5.7) and final mean score was 3.8 (SD, 3.45)(P=.002).
Staff and Administration Surveys
Eight staff members participating in the program were surveyed to identify their views on the success or lack of success of the program. All staff members agreed the virtual sessions with the residents and dental hygienists increased their understanding of the need for individualized day-to-day oral health care, with 6 of them stating strongly agreement. See Table 4 for survey results.
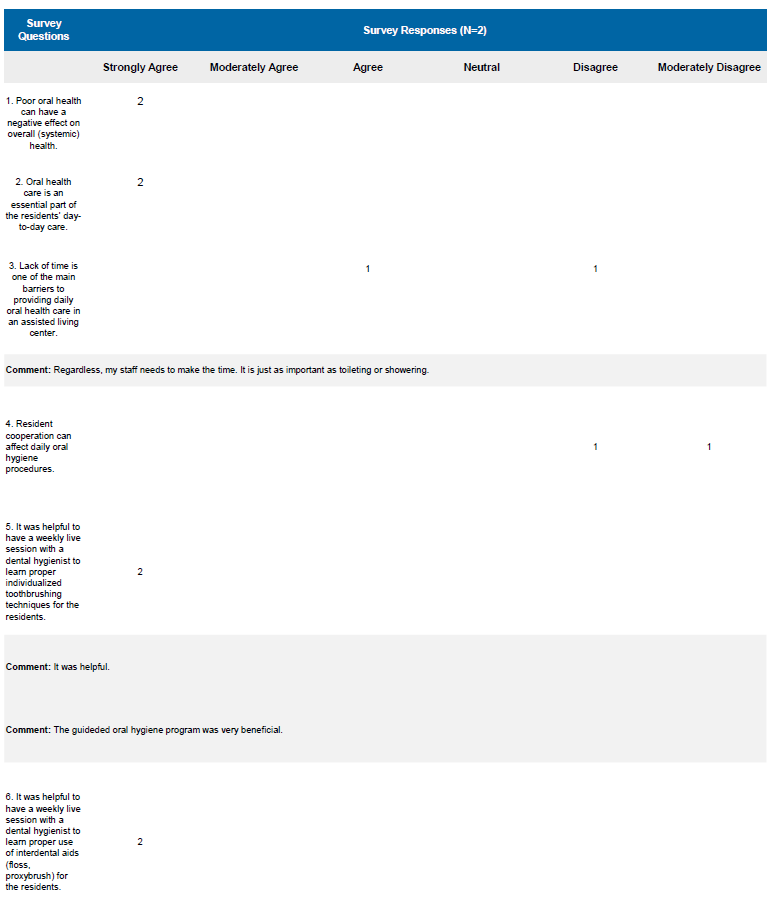
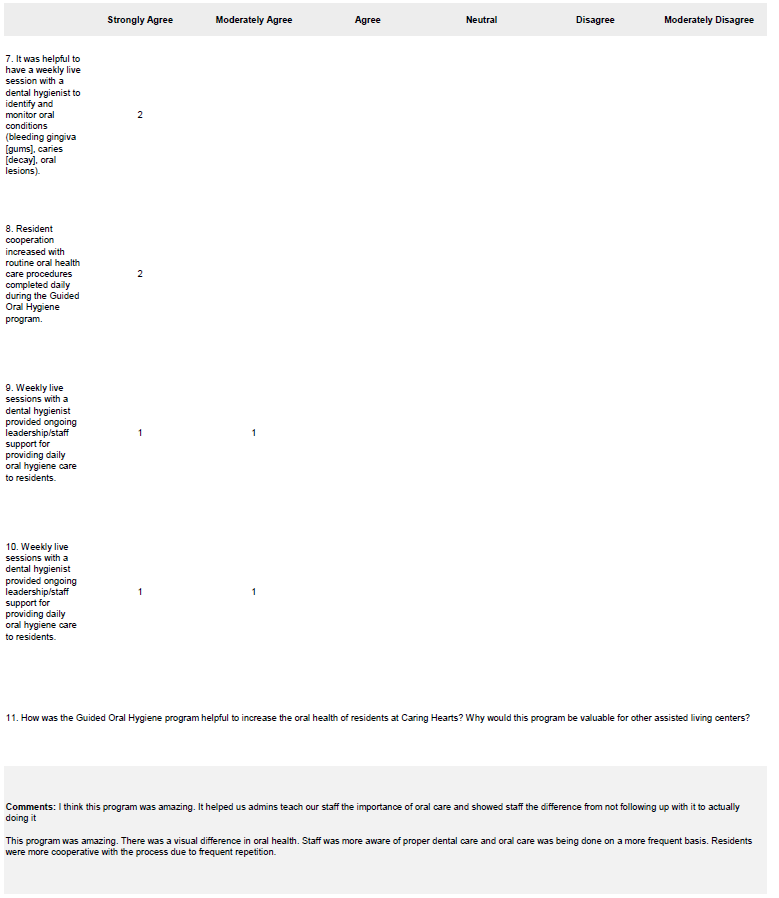
Administrative staff were also surveyed. One administrator stated, “This program was amazing. There was a visual difference in oral health. Staff members were more aware of proper dental care and oral care was being done on a more frequent basis. Residents were more cooperative with the process due to frequent repetition.” See Table 5 for survey results.
Table 4 Staff Survey Responses
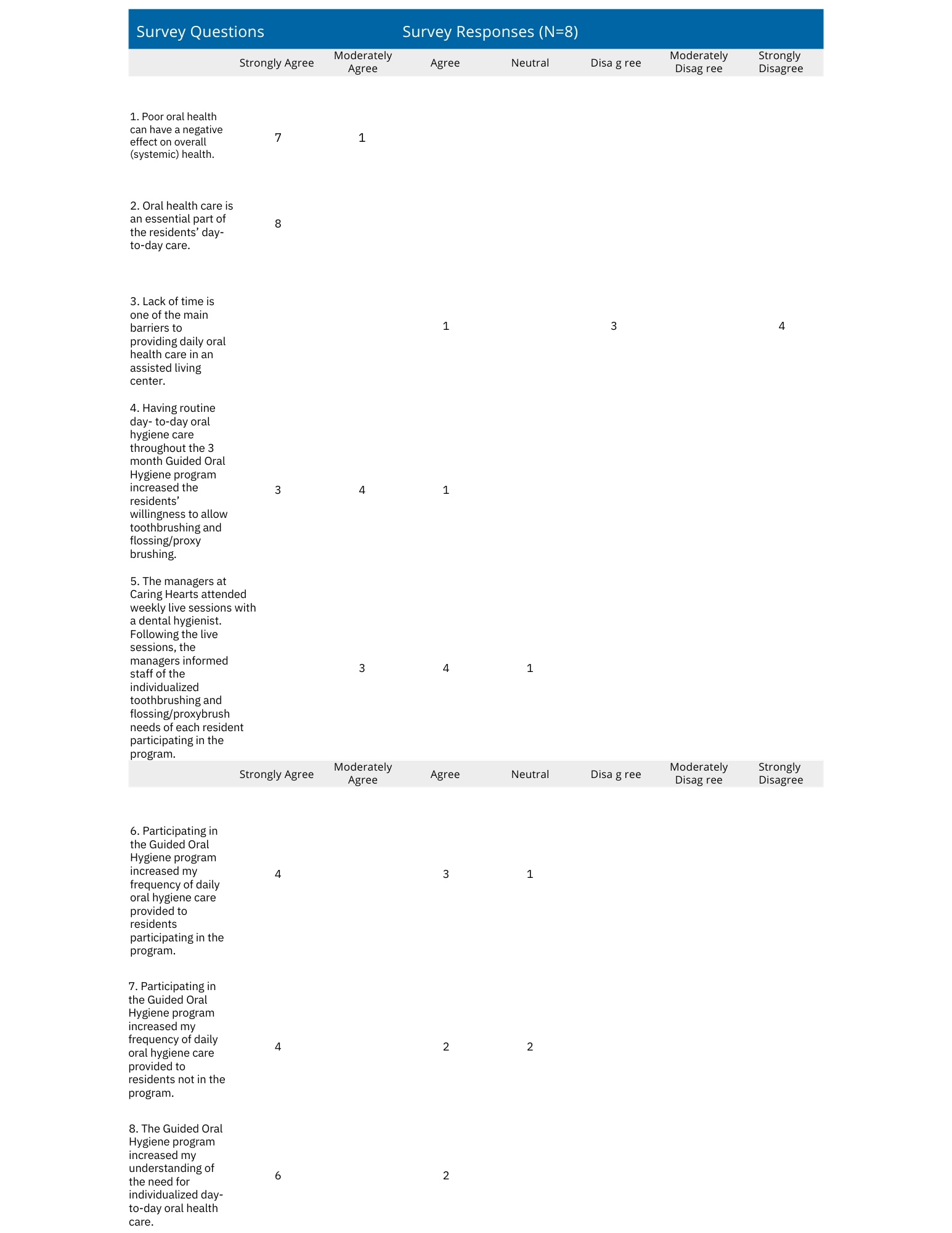
Table 5. Administrative Survey Responses
Discussion
After the first 3 weeks of the program, staff needed minimal guidance with toothbrushing techniques, and by 4 weeks they were able to use the interdental aid without causing pain to the resident. An unexpected outcome was the increase in patient cooperation. In the first 2 weeks of the program, there were many challenges with residents who did not want to open their mouth or moaned because they did not want to participate. What we found each week was an improvement in residents opening their mouths and less moaning about participating. We never forced the residents to participate, but we encouraged them kindly and completed whatever aspect of oral care they would allow us to do for the day. As the weeks progressed, the guided sessions became routine to the residents participating in the program and they became more cooperative. The staff became comfortable and efficient with providing daily oral hygiene care, which in turn increased the efficiency of the process and made providing day-to-day oral hygiene care manageable during a routine busy day.
The increased cooperation and staff’s increased skills in providing daily oral hygiene, resulted in a substantial decrease in gingival inflammation and oral debris in residents participating in the program. The innovative methods employed by the GOHP can be implemented within any LTC facility to improve the oral health of residents. Improved oral health is a result of the interprofessional collaboration between medical staff and dental professionals during the virtual live sessions. This collaboration allows for real-time discussions between staff (mental and overall health considerations) and dental professionals (oral health recommendations and techniques) for each resident. Additionally, improved oral health occurred from the continued daily oral hygiene services provided between live sessions with staff who were more confident in providing these procedures. Furthermore, residents became accustomed to the routine of daily oral hygiene care and became more cooperative, which in turn allowed for increased removal of oral biofilm. Research has shown that staff in LTC facilities often do not provide oral health care for residents due to lack of confidence in providing such services, lack of patient cooperation, and lack of time throughout a busy day.16-18 Implementing programs such as GOHP may help to address some of the issues with implementing daily oral hygiene care in LTC settings.
Challenges and Considerations
As with any use of technology, Internet connections can be a problem. Occasionally, during live sessions the screen would freeze, making it difficult to watch the staff members demonstrate oral hygiene techniques. An additional challenge presented when the facility had an emergency or site visitors; on those days, the virtual sessions were canceled and rescheduled for another day. This challenge did not happen often; however, initially scheduling backup days for the virtual sessions is recommended.
Conclusions
Oral health is essential to quality of life.5 An increasing population of adults aged 65 and older have significant oral health conditions affecting overall health and quality of life. Interprofessional workforce models are needed to address the complex health care needs of older adults. Those residing in LTC settings are not receiving basic oral hygiene care to prevent poor oral conditions, which increases the risk for and exacerbates systemic conditions. Programs similar to the GOHP represent a collaborative effort to improve overall health for older adult residents. Implementation of this program requires the commitment from LTC facility administrators, staff, and oral health practitioners to create a unique interprofessional workforce model and an innovative teledentistry delivery system to benefit older adults. The GOHP is not without limitations. The study enrolled a small sample size of participants, which limits the ability to generalize the results. Despite this limitation, the statistical outcomes had a large effect size and greatly increased the oral health of the participants.
Affiliations, Acknowledgements, Disclosures & Correspondence
Rachelle Williams, RDH, MS1 • Jennifer Dahlke, RDH, BS2
Affiliations:
1 Department of Dental Hygiene, Idaho State University, Pocatello, ID
2 Department of Dental Hygiene, Idaho State University, Pocatello, ID
Acknowledgements:
The authors thank Ellen Rogo, professor and associate dean of curriculum and assessment, for her assistance and mentorship in developing the research study and the staff at Caring Hearts assisted living center for their participation in the GOHP.
Disclosures:
The Idaho Oral Health Program (IOHP) awarded a HRSA subgrant to the Department of Dental Hygiene at Idaho State University for developing and implementing a Teledentistry Program called the Bengal Smiles for Life program. Permission was provided by IOHP to utilize $1500.00 of the subgrant funding for equipment and supplies for the Guided Oral Hygiene Program.
Correspondence:
Rachelle Williams
931 Sawtooth St
Phone: 208-282-2395
email: rachellewilliams@isu.edu
References
- Colby SL, Ortman JM. Projections of the size and composition of the U.S. population: 2014 to 2060. Current Population Reports. US Census Bureau; 2015. Updated October 8, 2021. Accessed June 30, 2022. https://www.census.gov/library/publications/2015/demo/p25-1143.html
- Nation begins to age as it becomes more diverse. News release. US Census Bureau; June 20, 2022. Accessed June 30, 2022. https://www.census.gov/newsroom/press-releases/2022/population-estimates-characteristics.html
- Harris-Kojetin L, Sengupta M, Park-Lee E, et al. Long-term care providers and services users in the United States: data from the National Study of Long-Term Care Providers, 2013–2014. Vital Health Stat 3. 2016;38:x-xii, 1-105.
- National Institutes of Health. Oral Health in America: Advances and Challenges. US Department of Health and Human Services, National Institutes of Health, National Institute of Dental and Craniofacial Research; 2021. Accessed August 22, 2023. https://www.nidcr.nih.gov/sites/default/files/2021-12/Oral-Health-in-America-Advances-and-Challenges.pdf
- Griffin SO, Griffin PM, Li CH, Bailey WD, Brunson D, Jones JA. Changes in older adults’ oral health and disparities: 1999 to 2004 and 2011 to 2016. J Am Geriatr Soc. 2019;67(6):1152-1157. doi:10.1111/jgs.15777
- Eke PI, Wei L, Borgnakke WS, et al. Periodontitis prevalence in adults ≥ 65 years of age, in the USA. Periodontol 2000. 2016;72(1):76-95. doi:10.1111/prd.12145
- Badr F, Sabbah W. Inequalities in untreated root caries and affordability of dental services among older American adults. Int J Environ Res Public Health. 2020;17(22):8523. doi:10.3390/ijerph17228523
- National Council on Aging. Get the facts on healthy aging. Updated March 13, 2023. Accessed June 30, 2022. https://www.ncoa.org/article/get-the-facts-on-healthy-aging
- Kirzinger A, Neuman T, Cubanski J, Brodie M. Data note: prescription drugs and older adults. Published August 9, 2019. Accessed August 23, 2023. https://www.kff.org/health-reform/issue-brief/data-note-prescription-drugs-and-older-adults/
- Jurasic MM, Gibson G, Wehler CJ, Orner MB, Jones JA. Caries prevalence and associations with medications and medical comorbidities. J Public Health Dent. 2019;79(1):34-43. doi:10.1111/jphd.12292
- Kramarow EA. Dental Care Among Adults Aged 65 and Over, 2017. NCHS Data Brief, No. 337. National Center for Health Statistics; 2019. Accessed August 22, 2023. https://www.cdc.gov/nchs/data/databriefs/db337-h.pdf
- Dominy SS, Lynch C, Ermini F, et al. Porphyromonas gingivalis in Alzheimer’s disease brains: Evidence for disease causation and treatment with small molecule inhibitors. Sci Adv. 2019;5(1):eaau3333. doi:10.1126/sciadv.aau3333
- Tracee SD, Ann B, Margaret L. Oral care in the long-term care of older patients: How can the dental hygienist meet the need? J Dent Hyg. 2015:89(4):229-237.
- Coker E, Ploeg J, Kaasalainen S, Fisher A. A concept analysis of oral hygiene care in dependent older adults. J Adv Nurs. 2013;69(10):2360-2371. doi:10.1111/jan.12107
- Liu C, Cao Y, Lin J, et al. Oral care measures for preventing nursing home-acquired pneumonia. Cochrane Database Syst Rev. 2018;9(9):CD012416. doi:10.1002/14651858.CD012416.pub2
- Hartshorn JE, Cowen HJ, Comnick CL. Cluster randomized control trial of nursing home residents’ oral hygiene following the Mouth Care Matters education program for certified nursing assistants. Spec Care Dentist. 2021;41:372-380. doi:10.1111/scd.12577
- Albrecht M, Kupfer R, Reissmann DR, Mühlhauser I, Köpke S. Oral health educational interventions for nursing home staff and residents. Cochrane Database Syst Rev. 2016;9(9):CD010535. doi:10.1002/14651858.CD010535.pub2
- Mohammad JJY, Franks K, Hines S. Effectiveness of professional oral health care intervention on the oral health of residents with dementia in residential aged care facilities: a systematic review protocol. JBI Database Syst Rev Implement Rep. 2015;13(10):110-122. doi:10.11124/jbisrir-2015-2330
- Löe H. The gingival index, the plaque index and the retention index systems. J Periodontol. 1967;38(6):Suppl:610-616. doi:10.1902/jop.1967.38.6.610
- Simplified oral hygiene index. Malmo University, Oral Health Country/Area Profile Project; 2013. Accessed June 30, 2022. https://capp.mau.se/methods-and-indices/
- American Dental Hygienist’ Association. Standards of Clinical Dental Hygiene Practice. Revised 2016. Accessed August 22, 2023. http://www.dhed.net/ewExternalFiles/2016-Revised-Standards-for-Clinical-Dental-Hygiene-Practice.pdf
