


Letter to the Clinical Editor
Hi Mort!
I read with great interest your thoughts and those of leading colleagues on left radial cath/PCI in a recent Cath Lab Digest.1
I agree with all of those who find the procedure by this approach less than optimal — in fact, downright infuriating at times!
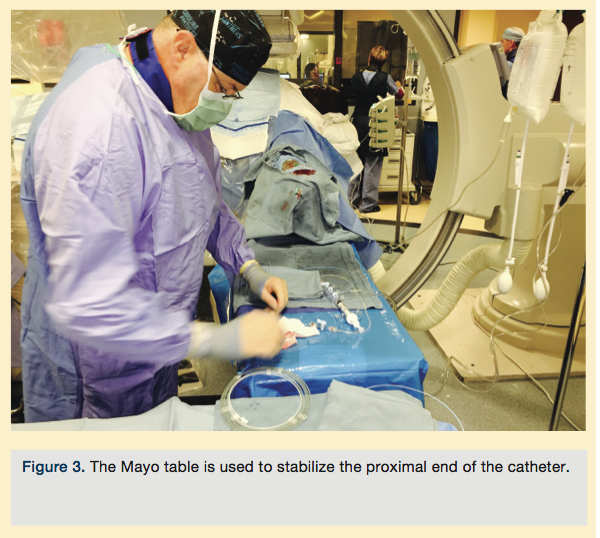
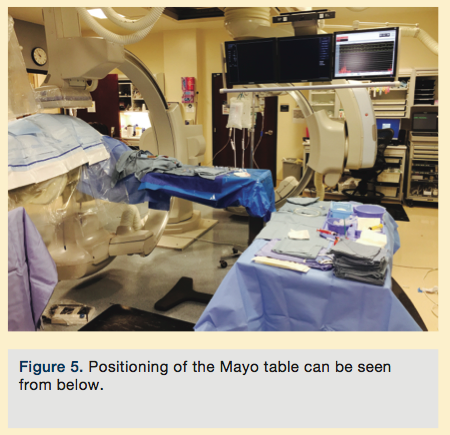
We’ve developed in our lab a set up that does mitigate at least some of the misery. It involves keeping the left arm extended, swinging the monitors around to be behind the patient’s left arm, and using a Mayo table that can be rolled and adjusted vertically to provide a platform for stabilizing the proximal end of the catheter for manipulation and device insertion. The foot pedal is below the Mayo stand.
While not ideal (it is still difficult to pan for diagnostics, but not as much of an issue for PCI, where panning tends to be more limited), for me it is preferable to trying to reach over — especially a large individual — where the hand tends to pronate and drift away.
I think, though, a better solution is a redesign of the cath lab table (Figure 1, note extension to better position the operator, image intensifier, and left wrist of the patient). Figures 2-5 are of our current set up as described above.

The cath lab should be designed to meet our needs and those of our patients, and should not require continual workarounds on a daily basis. The modified “T” table proposed allows the operator to stand where he/she usually stands with all of the monitors and equipment in its usual place. This should provide a better sense of security for the operator — and given the well <50% of adoption of radial by our U.S. colleagues — would, I think, accelerate radial acceptance and use.
Also, since the majority of patients are right-handed, they would have use of their dominant hand immediately after the procedure with no “light use” mandated in the following 24-48 hours.
While true laterals could not be done, I do not think this is a major issue; gantries should be designed to slide down over the femoral area if an emergent temp pacer is needed (although knowing how to use alligator clips on a coronary wire should mitigate this need).
I have shown this design to several cath lab vendors and all have told me they do not make the tables in-house.
It’s time for us to make the cath lab work for us. We don’t do caths the same way we did when the original rooms were designed. It’s clearly time for a redesign.
Appreciate your thoughts!
Peter L. Duffy, MD
Director/ Cardiovascular Service Line
FirstHealth Cardiology Services
Reid Heart Center
Pinehurst, North Carolina
pld@nc.rr.com
Peter,
Thanks for taking the time and interest to add to the debate. I think you may get a cath lab maker to adjust their systems. Worth a try.
Best wishes,
M.
Reference
- Kern M, et al. Conversations in cardiology: should you still prepare the femoral site for radial cases? Cath Lab Digest. 2015 May; 23(5): 4-6. Available online at https://www.cathlabdigest.com/article/Conversations-Cardiology-Should-You-Still-Prepare-Femoral-Site-Radial-Cases. Accessed July 21, 2015.


