


New Year — New Bundle! 2018 welcomes the new voluntary Bundled Payments for Care Improvement – Advanced Initiative (BPCI Advanced)
 In this month’s article, we are keying in on the very hottest topic currently facing cardiology, the advent of Centers for Medicare and Medicaid Services’ (CMS) new BPCI Advanced. Announced in early January, these voluntary cardiac bundles have the potential to achieve real, quantifiable results for those physician practices and hospitals who feel they can manage the target price that will be set by CMS. Key objectives of this initiative center on care redesign, decreasing costs due unnecessary or low-value care, and financial accountability tied to outcomes. Anne Beekman, RN, Vice President, MedAxiom Consulting, will walk us through some of the more salient aspects of the program, and when and why it’s important for interested parties to sign up by the March 12 deadline.
In this month’s article, we are keying in on the very hottest topic currently facing cardiology, the advent of Centers for Medicare and Medicaid Services’ (CMS) new BPCI Advanced. Announced in early January, these voluntary cardiac bundles have the potential to achieve real, quantifiable results for those physician practices and hospitals who feel they can manage the target price that will be set by CMS. Key objectives of this initiative center on care redesign, decreasing costs due unnecessary or low-value care, and financial accountability tied to outcomes. Anne Beekman, RN, Vice President, MedAxiom Consulting, will walk us through some of the more salient aspects of the program, and when and why it’s important for interested parties to sign up by the March 12 deadline.
— Gary Clifton, Vice President, Terumo Business Edge
On November 30, 2017, CMS announced the cancellation of the mandatory Episode Payment Model (EPM). However, with this cancellation, CMS promised a new revision of a bundles payment model was on the horizon. Fast forward to January 8, 2018 and the release of the new BPCI Advanced. So, how is this program different from the original release and specific procedural cardiology?
It might be good to start with how the two BPCI programs are the same. CMS has not changed its belief in the value of the bundle payment model or the benefit to the consumer. Here is a list of what CMS is looking to achieve with the bundled payment model: “Payment models that provide a single bundled payment to health care providers can motivate health care providers to furnish services more effectively, to better coordinate care, and to improve the quality of care.” CMS bases this statement on previous success in bundle payment initiatives such as the Medicare Participating Heart Bypass Center Demonstration. This body of work proved that a bundled payment for a specific discharge resulted in Medicare savings without any decline in quality outcomes. Both the original mandatory program and the new voluntary program intend to achieve cost savings while driving up quality with better care management, as well as eliminating unnecessary care, reducing post discharge emergency department (ED) admissions, and reducing readmissions. The concept of reducing costs and unnecessary care has been part of everyone’s job for a long time, but BPCI Advanced will require a larger team and responsibility for 90 days.
What are the key components and differences of the new BPCI Advanced initiative? The initiative is a voluntary program that consists of 29 inpatient bundles and 3 outpatient bundles. The addition of outpatient bundles is unique from the first version, which did not include outpatient procedures such as PCI and defibrillators. Payment for the clinical episode is a single, retrospective payment and one risk track with a 90-day clinical episode time frame. The new BPCI Advanced program qualifies also as an Advanced Alternative Payment Model under the Medicare Access and CHIP Reauthorization Act of 2015 (MACRA). This is an important change from the first version, allowing physicians to use this bundled payment model in lieu of participation in the Merit-based Incentive Payment System (MIPS). Another noteworthy change to the new BPCI model is that either the physician or the acute care hospital can be the episode initiator or owner of the bundle. In the previous BPCI model, the acute care hospital was the owner or episode initiator of the bundle, and the physician or provider could participate, but only at the invitation of the hospital. As in the previous model, there will be quality performance metrics that drive incentive or penalty reconciliation payments, which have been capped at +20%. Pricing for the bundle is a target price provided in advance of the first performance period of each model year. In the next section, we will talk about how to get your pricing and the advantages of an on-time BPCI application whether or not you think participation in a voluntary bundle is the right thing for your practice or hospital.
Of the 29 inpatient bundles and 3 outpatient bundles, the cardiovascular-focused episodes are as follows:
- Percutaneous coronary intervention (inpatient [IP] and outpatient [OP]);
- Coronary artery bypass graft surgery (CABG);
- Congestive heart failure;
- Stroke;
- Acute myocardial infarction (AMI);
- Cardiac pacemakers;
- Cardiac valves;
- Cardiac defibrillators;
- Cardiac arrhythmia.
The BPCI episode will begin with an inpatient admission, called the “anchor” admission, or the start of an outpatient procedure, called the “anchor” procedure. Inpatient admissions will be identified through MS-DRGs (Medicare Severity-Diagnosis Related Groups) compared to outpatient admissions that will be identified through HCPCS (Healthcare Common Procedure Coding System) codes. The duration of the Clinical Episode will end 90 days from the end of the anchor admission or the end of the anchor procedure. The costs included in the 90-day episode are both Medicare Part A and B services, and examples are physician services, hospital outpatient services, readmissions, long-term care hospitals, skilled nursing facilities, home health, clinical labs, and hospice. Inpatient bundles also include diagnostic testing and certain therapeutic services provided three days prior to admission. There are some costs that are not included in the 90-day bundle such as major trauma, cancer care, organ transplant, and ventricular shunts.
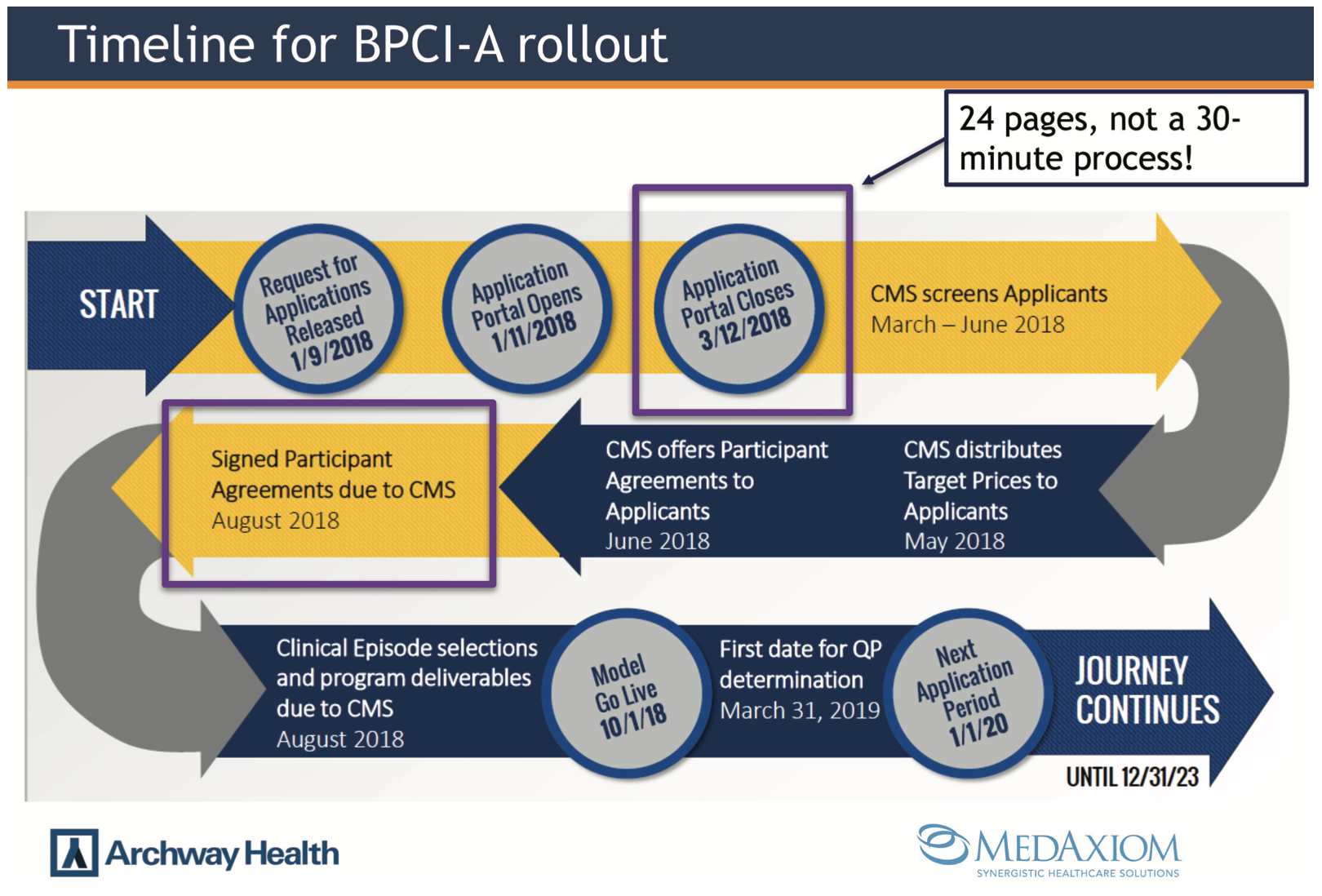
How do you know if participating in a voluntary bundle is right for your practice or program? Are there more advantageous bundles to be in? These are important questions and the good news is you can get benchmarking data from CMS without committing to participate in a voluntary bundle. Keep in mind the first set of participants will begin on October 1, 2018 and continue through December 31, 2023. Practices and programs that do not elect to participate will not be able to join until the second application opportunity, opening in January 2020. CMS has provided a timeline for submitting applications to participate in the BPCI Advanced program with a deadline of March 12, 2018. This first application step does not require you to select which bundles you want to participate in or require you to participate at all. So, if there is one takeaway from this article, it is to submit your non-binding application prior to March 12, 2018 and receive your data. Figure 1 is a diagram right from the CMS BPCI link (https://innovation.cms.gov/initiatives/bpci-advanced) that provides a visual of the timeline for the BPCI program and key pieces of information.
This visual outlines the process for an application related to bundle participation. The application is a 24-page document consisting of 12 components. The application process is more robust than seen in the past with other models, so plan accordingly. CMS states it will prioritize applications based on the following components: Model Design/Care Improvement, Cost Reduction, Quality of Care, and Patient Centeredness and Organizational Capabilities. If your practice or hospital has submitted its application, received an agreement, and elects to participate according to the timeline, you must do two things by August 2018:
- Commit to one or more clinical episodes;
- Enter into a BPCI Advanced Model Participation Agreement with CMS.
Once you select your clinical episodes, you may not add or drop clinical episodes until January 1, 2020.
Who can enroll as a practice or hospital? This entity is defined as a “Participant” and a Participant can be one of two types:
Non-Convener Entity
- Acute Care Hospital (ACH)
- Physician Group Practices (PHPs)
Convener Entity
- Eligible entities that are Medicare-enrolled providers or suppliers
- Eligible entities that are not enrolled in Medicare
- Acute Care Hospitals
- Physician Practice Groups
Unless you are a provider who really wants to get out of MIPS, what is the incentive to participate in a voluntary bundle payment plan? The answer to that will lie with your data and your ability to manage in a competitive bundle. Once you receive your data, you want to do some work before you commit to bearing the downside risk. A program that has the infrastructure and relationships to manage an episode of care with high quality and low cost for 90 days will want to be involved. Figure 2 outlines potential upside savings for a cardiology group participating in an episode of care involving inpatient and outpatient PCI.
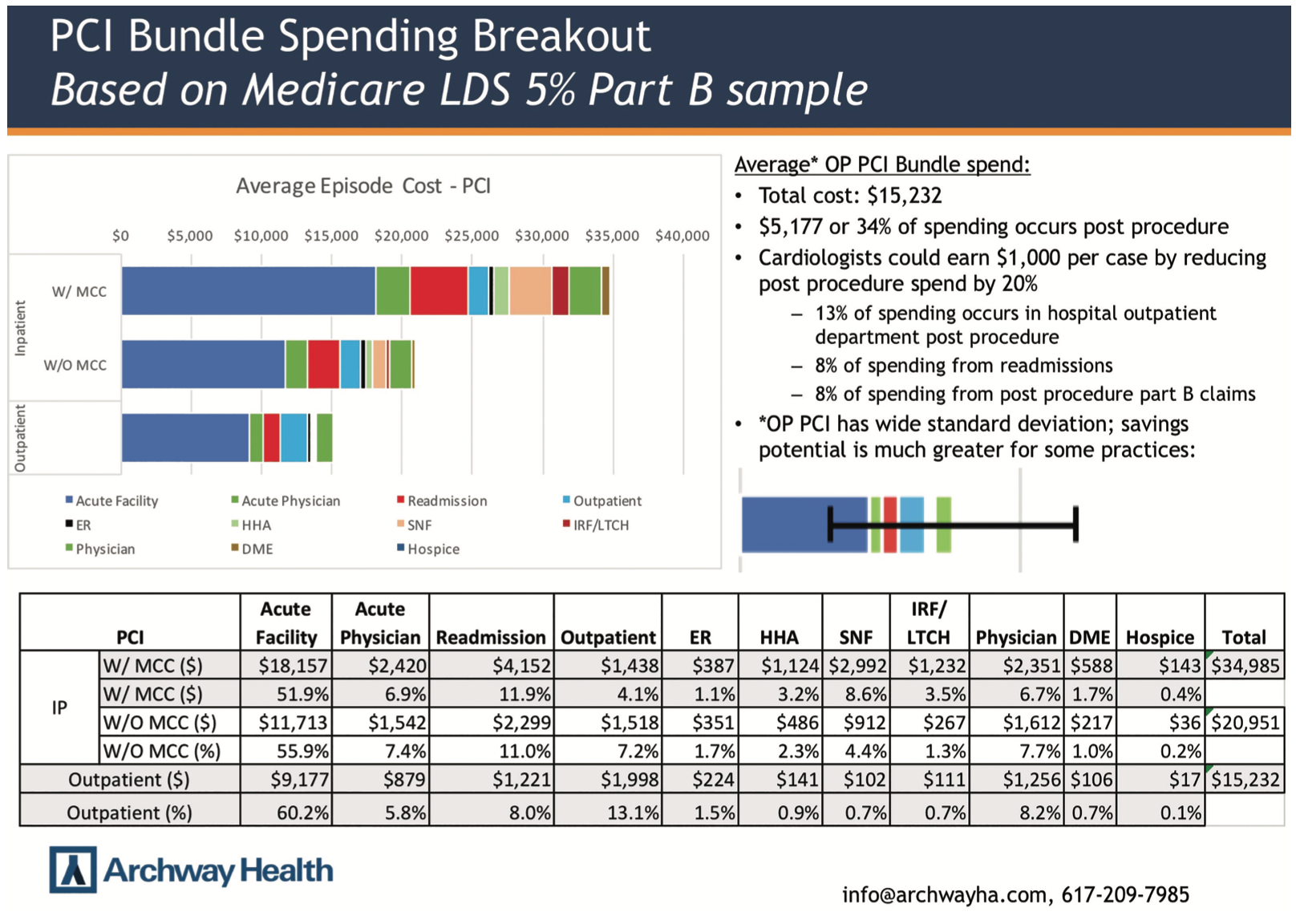
The data in Figure 2 is provided by Archway Health, a partner with MedAxiom. The potential savings identified in the Figure 2 graph highlights the variation in care for the PCI procedure over the 90-day episode. Just by reducing the post procedure spend by 20%, a provider or hospital could save $1,000.00 dollars per episode. At the end of the article, there is an offer from Archway Health for free help with submitting your data and then receiving the data, not in a data dump, but as an easy-to-read document as displayed in Figure 2.
It is easy to see why physicians and hospitals that have the ability to actively manage care and costs will be eager to participate. What are the necessary steps for understanding the new BPCI Advanced payment model? We suggest two basic steps: 1) Complete the application process by March 12, 2018, so you can review your data; and 2) Begin to review your team and resources for a 90-day episode.
Programs and providers may have different points of view on how and where to reduce unnecessary care and control the costs of healthcare; bundles have had success in reducing costs while meeting or improving quality benchmarks. Today, bundles are voluntary, but it looks like the concept is here to stay, so why not make 2018 the year to get informed and be successful in a bundle?
Follow the links below to learn more about how to receive free help with your data submission and an easy-to-read format of the results.
https://medaxiom.lpages.co/bpci-a/
https://www.archwayhealth.com/bpci-advanced/


