Novel Radiation Protection Devices: An Update on Radiation Safety in the Cath Lab
Morton Kern, MD
Clinical Editor; Chief of Medicine,
Long Beach Veterans
Administration Health Care
System, Long Beach, California;
Associate Chief Cardiology,
Professor of Medicine, University of
California Irvine, Orange, California
mortonkern2007@gmail.com
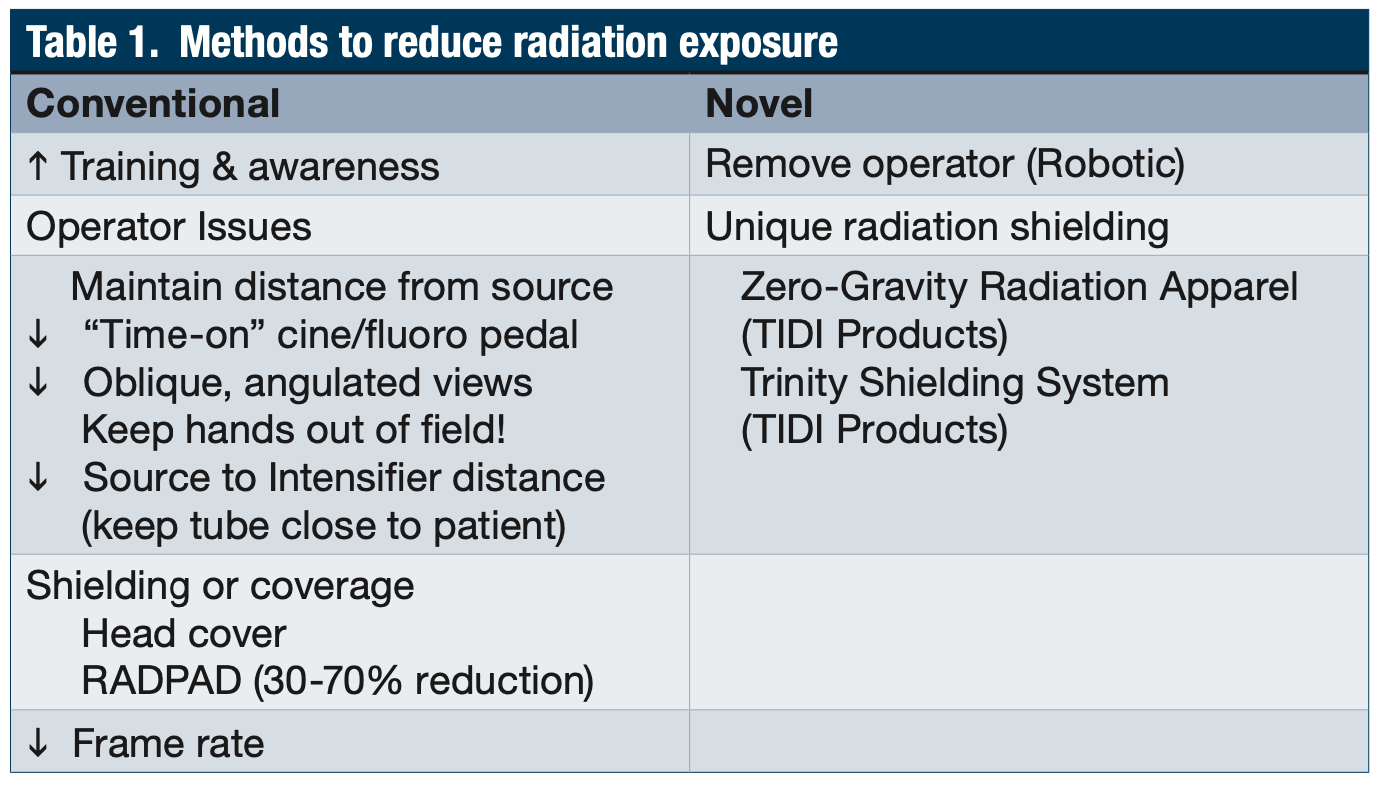
Table 1. Methods to reduce radiation exposure
Stimulated by a couple of recent articles on the efficiency of the RADPAD protection drape in reducing operator’s exposure1 and the effects of shielding on nurses and technologists in the cath lab2, I thought it would be a good idea to see what was new and what we should be thinking about to reduce radiation exposure to ourselves, our team, and our patients.
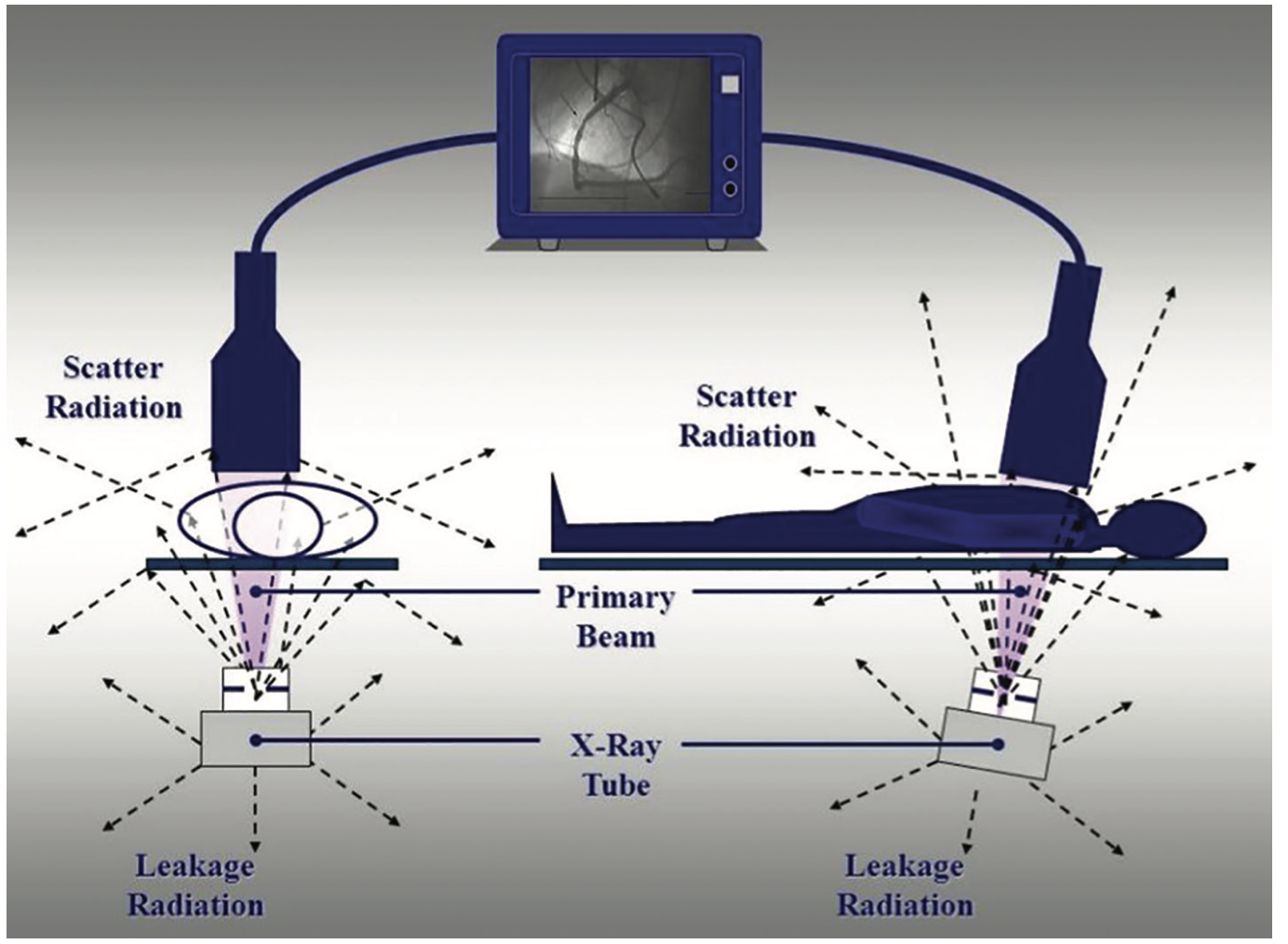
Figure 1A. Diagram of radiation scatter in the cath lab. Most radiation scatter occurs through the patient’s body and is increased with increasing angulations.
To remind all of us, radiation safety is everybody’s business in the cath lab. While standard teaching about radiation safety is part of every team member’s basic concepts and training, there have been very few major changes in our protective equipment over the years to reduce radiation exposure, other than to employ the standard tableside and mobile shielding. We know that radiation dose is directly related to exposure time, determined by the operator’s visualization needs (i.e., pedal time). We also are aware that the distance away from radiation source is also a critical determinant of dose: the further, the better. Methods to reduce exposure are summarized in Table 1. Let’s not forget that significant radiation exposure has the potential to impact the health and well-being of interventional cardiologists and their teams by causing3:
Cancer (odds ratios [OR] 3.0, 95% confidence interval [CI] 1.5-6.2);
Cataracts (OR 6.3, 95% CI 1.5-27.6);
Hypertension (OR 1.5, 95% CI 0.9-2.6); and
Skin lesions (OR 2.8, 95% CI 1.3-6.1).
Generalized adverse health effects such as cardiovascular disease and diminishment of reproductive capacity also may be linked to chronic, low-dose radiation exposure.3
Is Our Current Radiation Shielding Sufficient?
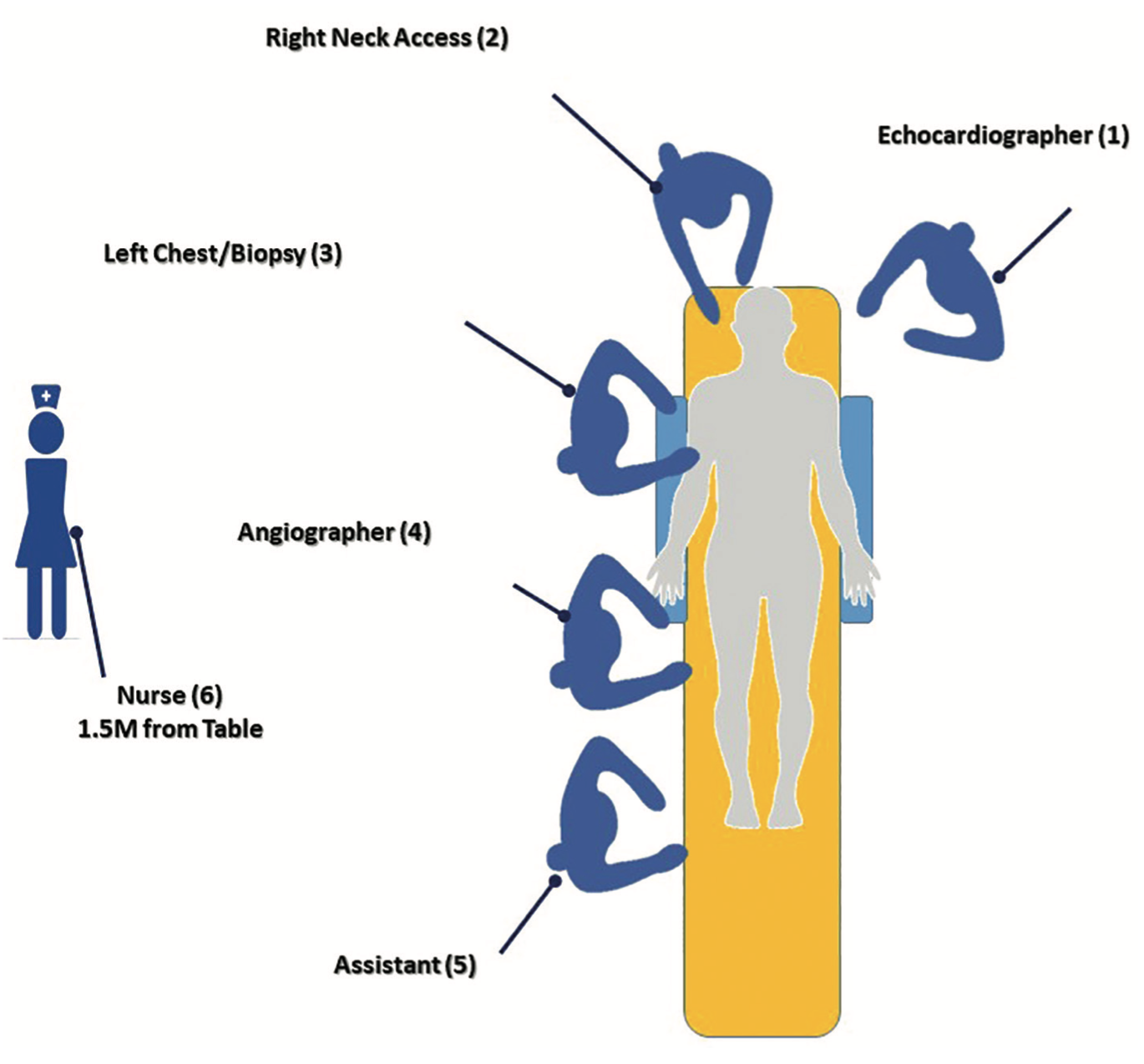
Figure 1B. Diagram of locations that are exposed to radiation in the cath lab. Compared to the pre-structural heart disease era, there are now personnel located closer to the x-ray tube for anesthesia and TEE operations.
Courtesy of Dr. Robert Wilson, Founder and CEO, Egg Medical, Inc.
Cath lab radiation shielding provides only partial protection depending on location around the table, body heights and imaging angles (Figure 1A-B). Personal protection equipment (PPE) alone has limits and is not sufficient to block all scatter radiation dose to the interventional cath lab staff. No current radiation protection strategy is designed to protect the entire health care team in the interventional cath lab room (Figure 2). We need to account for additional staff locations around the table for transcatheter aortic valve replacement (TAVR), right heart procedures, biopsies and transesophageal echocardiogram (TEE), with operators at the head of the table and very close to a radiation source. Although novel shield systems have been proposed over the last several years, none have been routinely employed in most laboratories.
Is Shielding Protecting Nurses and Techs in the Lab?
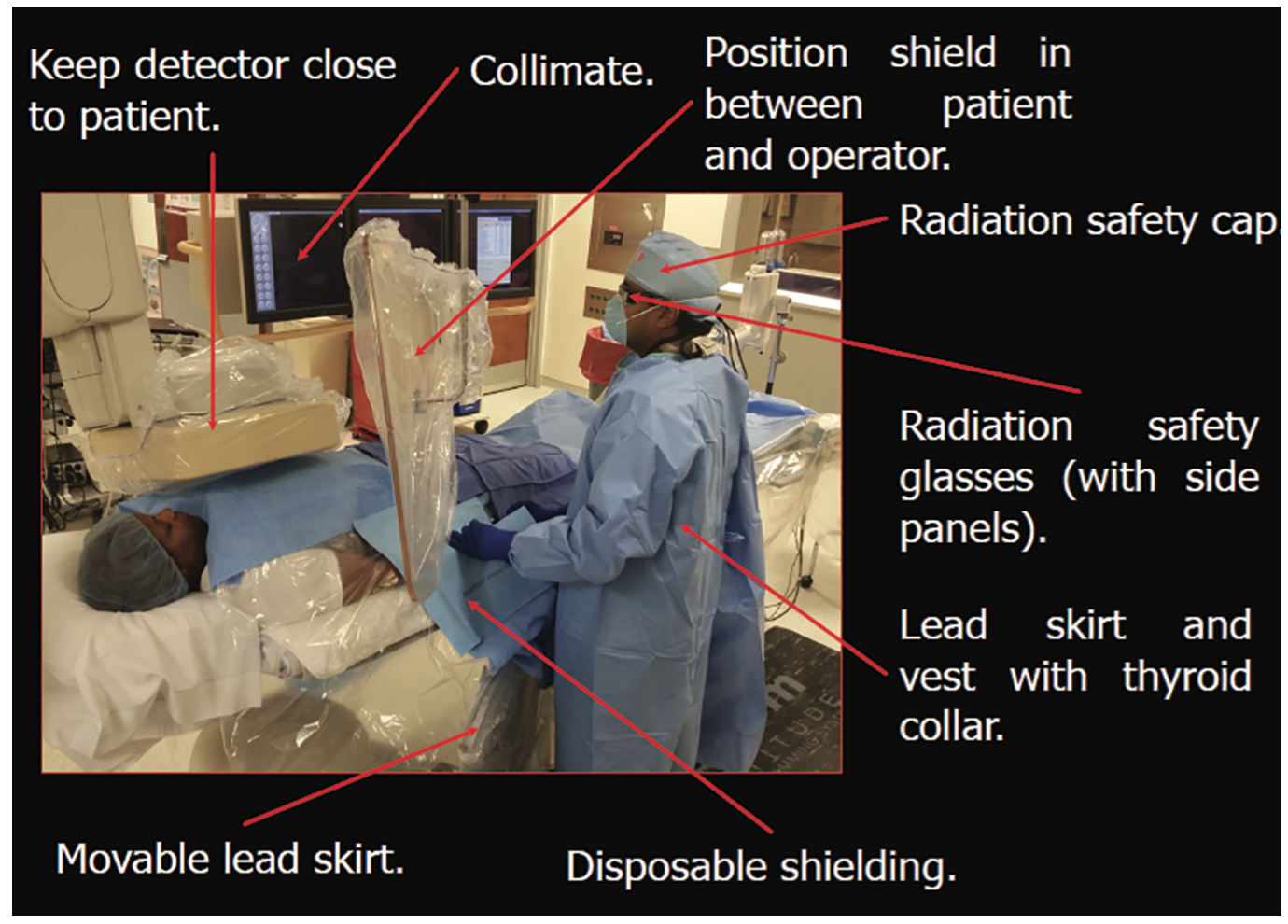
Figure 2. Ways to reduce radiation injury in the cath lab.
Reprinted with permission from Kumar G, Rab ST. Radiation Safety for the Interventional Cardiologist—A Practical Approach to Protecting Ourselves From the Dangers of Ionizing Radiation. http://www.acc.org. January 4, 2016. Accessed December 12, 2017. http://www.acc.org/latest-in-cardiology/articles/2015/12/31/10/12/radiation-safety-for- the-interventional-cardiologist.
During daily operations, we hope that the circulating cath lab personnel are far enough from the x-ray tube to keep their radiation exposure at very low levels. Unfortunately, we probably do not use these vertical shields enough or some may not believe they actually work. Madder et al2 recently looked at radiation exposure among scrub technologists and nurse circulators during cardiac catheterization, emphasizing the impact of using accessory lead shields. Real-time x-ray exposure was collected in 764 consecutive procedures in two phases. In the first phase, standard radiation protection measures were used and in the second phase, standard radiation protections were combined with an accessory lead shield placed between the staff member and the patient. Radiation exposure was then reported as a normalized dose area product. They found that accessory shield use was independently associated with lower dose area product exposure among both technologists (with a 34% reduction) and nurses (with a 36% reduction). The authors determined that the use of accessory shielding was indeed associated with a significant reduction in radiation exposure among nurses and technologists.
Selective Shielding to Reduce Exposure
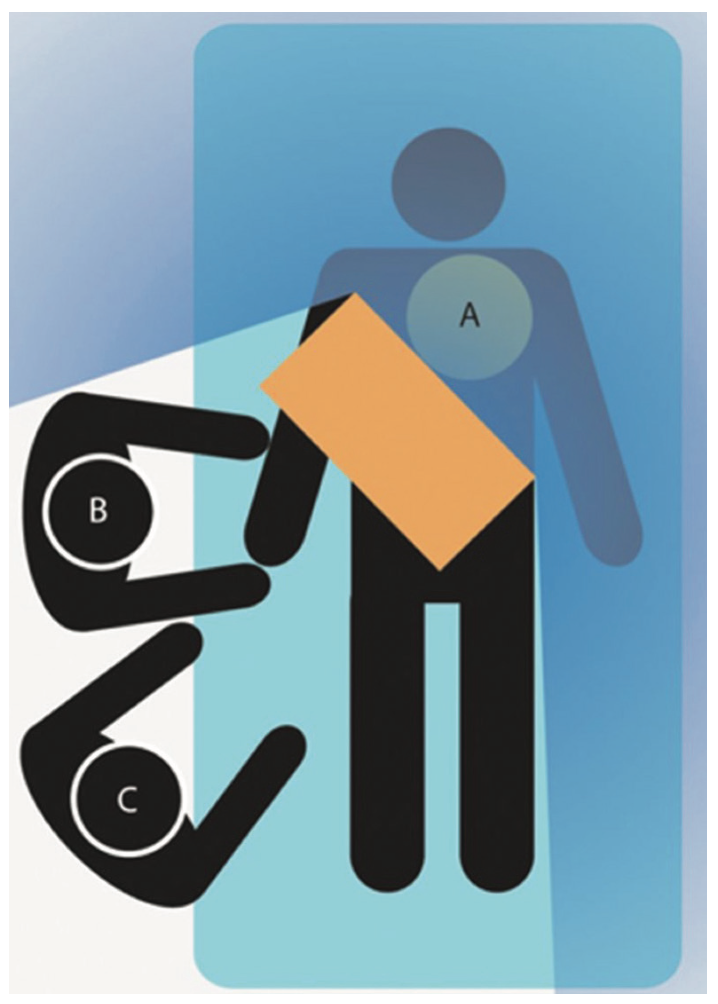
Figure 3. Position of the absorbing shield, placed on the patient, between the image intensifier (A), the primary operator (B), and occasionally the secondary operator (C). Reprinted with permission from Wieneke Vlastra et al. Circ Cardiovasc Interv. 2017;10:e006058
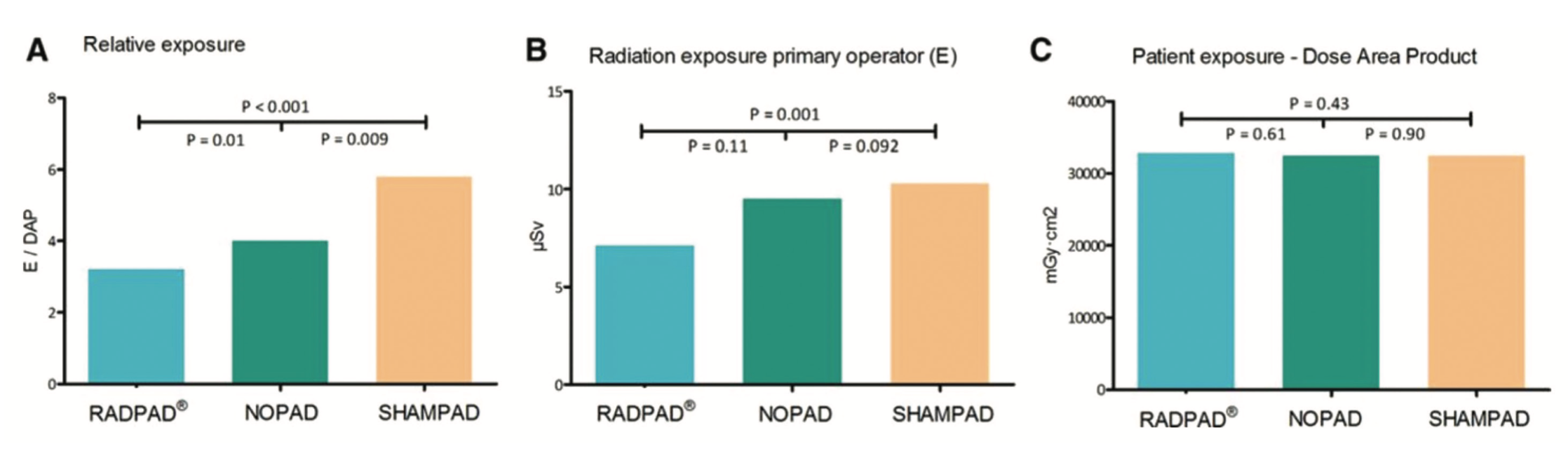
The RADPAD (Worldwide Innovations & Technologies, Inc.) is a sterile, disposable, lead-free shield placed on the patient’s side and is presumed to minimize operator-received scattered radiation. The efficacy of the RADPAD was compared to a standard treatment with no pad or sham treatment with a pad that had no shielding in it1 (Figure 3). The sham pad allowed for testing of shield-induced radiation behaviors by the operators. The exposures were compared between the RADPAD, “SHAMPAD”, and “NOPAD” as the ratio between the operator’s exposure and the patient’s exposure in dose area product in mGy/cm2. In 766 consecutive procedures, each of the three groups of 255 patients were tested. The RADPAD was associated with 20% reduction of relative operator exposure compared to NOPAD and a 44% relative exposure compared to the use of the SHAMPAD. SHAMPAD with associated with 43% higher relative radiation exposure than procedures with NOPAD (Figure 4). It appears that in daily clinical practice, use of the radiation RADPAD shield reduces the operator radiation exposure compared to with no pad or sham pad, and supports the use of such a device in the cath lab.
Increased Shielding Without the Weight
Figure 4. Relative exposure (A) (×10–4) is defined as the ratio between the exposure of the primary operator at chest level (B) and the patient exposure per procedure (C). Data are presented as mean (A) or median (B and C). DAP indicates dose area product; NOPAD, standard treatment; RADPAD, radiation absorbing shield; and SHAMPAD, sham shield. Reprinted with permission from Wieneke Vlastra et al. Circ Cardiovasc Interv. 2017;10:e006058
A ceiling-suspended gantry system is available to support a walk-in, lead-lined suit that eliminates the weight of lead aprons on the users. Stress injury due to the weight of lead has been reported by interventionalists. Using TIDI Products’ Zero-Gravity Radiation Protection System (Figure 5), this issue is eliminated. The lead apron has 1-mm lead equivalency protection from the thyroid to groin, about twice the protection compared to standard lead aprons. It also provides 0.5-mm protection where previously there was none available, with front and side protection from direct and scatter radiation. While this system has been available for several years, its adoption has been slow.
A Radiation Nest: Egg Radiation Protection
Figure 5. The Zero-Gravity Total Body Shield (TIDI Products) is a suspended personal protective system. It utilizes a 1.0 mm lead shield that protects the entire torso, upper arms and legs and engages magnetically to a vest worn by the operator under their sterile gown so it can move with them or be easily moved out of the way when not needed. In addition, it also employs a 0.5 mm lead equivalent lead-acrylic head shield that protects the head, eyes and throat of the operator.
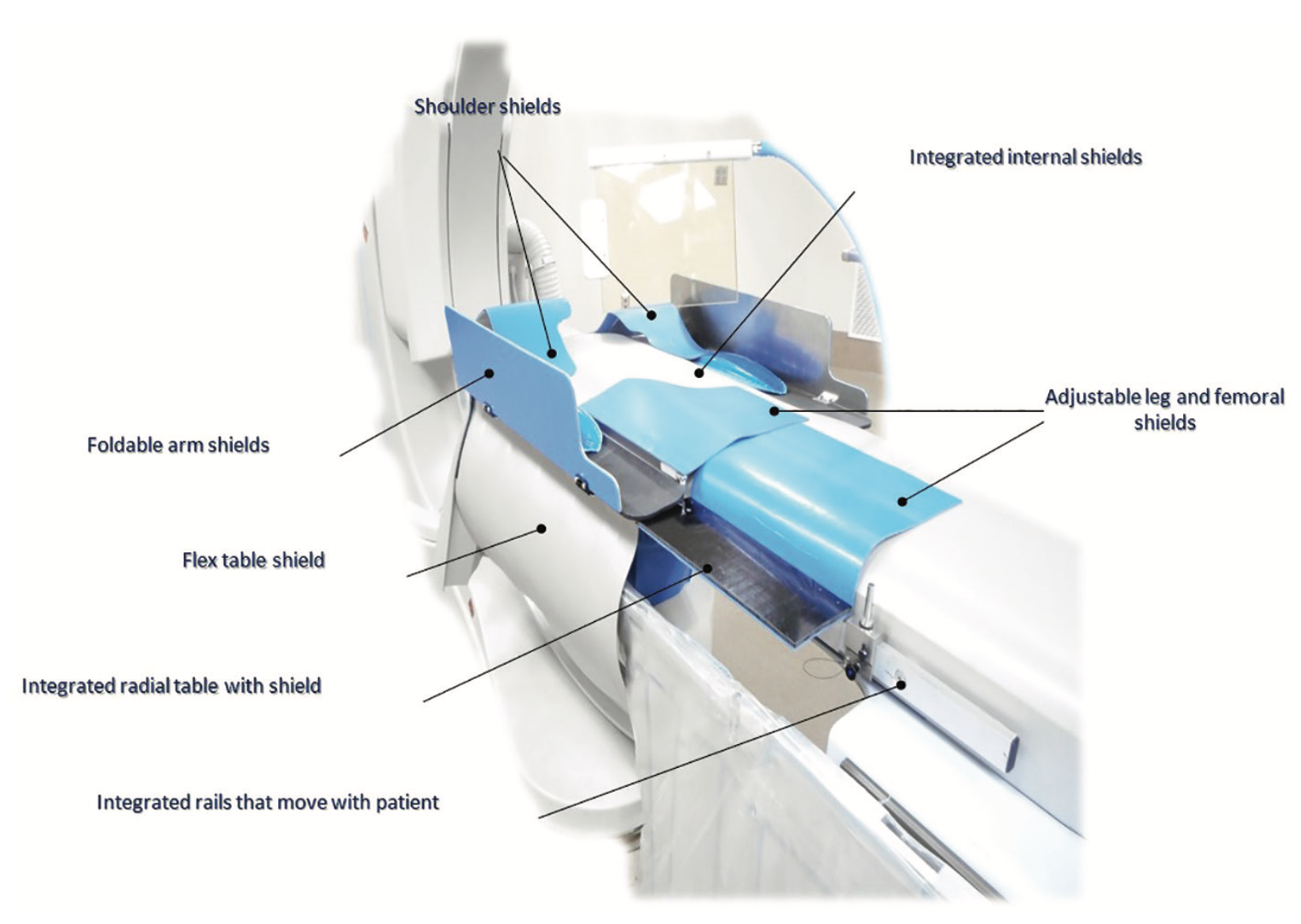
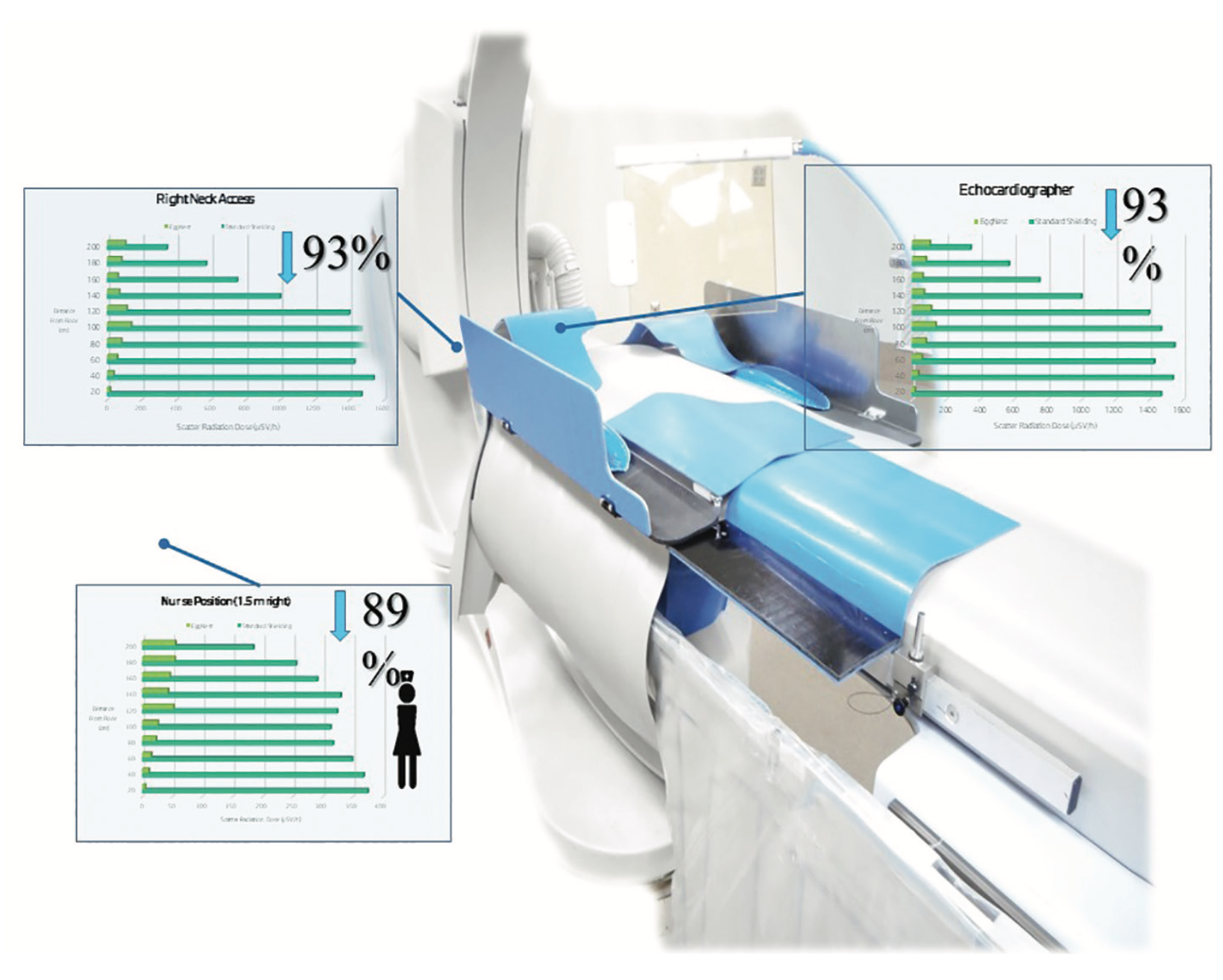
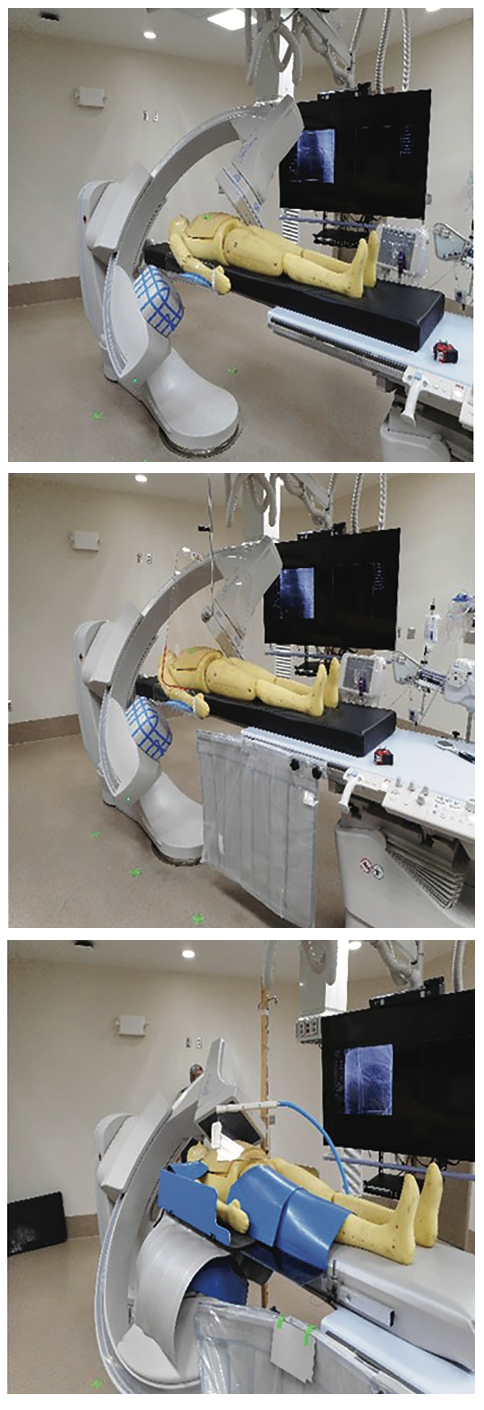
The EggNest-XR System (Egg Medical) is a carbon fiber sled platform with flexible shielding for radiation protection which conforms to the patient’s body to provide effective shielding with full x-ray gantry motion. It is particularly designed to improve shielding for radial, femoral and neck access, with specifically designed flexible shields for head and neck protection. The system lies on top of the x-ray table and includes integrated electrocardiogram (ECG) wiring (Figure 6A-B). Significant reductions in x-ray exposure were demonstrated for each position both above and below the table, as well as around the table with the EggNest-XR System compared to the standard shielding (Figure 7).
Remove the Operator from the Radiation Environment: Robotic Systems
Figure 6A. EggNest-XR System. Courtesy of Dr. Robert Wilson.
There are three robotic systems currently on the U.S. market that have indications for electrophysiology (EP) procedures, coronary artery procedures, and peripheral artery navigation and intervention. Stereotaxis was the first to introduce a robotic system, followed by the Hansen Sensei Robotic System, both designed for long EP procedures. The Corindus CorPath system gained U.S. Food and Drug Administration (FDA) approval for percutaneous coronary intervention (PCI) in 2012, followed by an indication for peripheral vessels in March 2016. Use of the robotic system permits the remote operation of devices during the cath procedure, thus eliminating exposure. However, confidence in complete independent remote operation for a complex PCI at this time remains low.
Additional Protection
Figure 6B. Effect of EggNest-XR System on scatter radiation: head and nurse positions. Percentages compared to standard shielding. Courtesy of Dr. Robert Wilson.
Beyond vertical mobile shields, radiation protection in the lab could be coupled with some novel systems of reducing x-ray system dosage.4 There are new x-ray systems which generate less x-ray rate dose. Manu et al at the Cleveland Clinic Foundation5 reported on dose reduction x-ray systems for the pediatric catheterization laboratory. They compared the Megalix tube and amorphous silicon detector to that of the Gigalix tube, a more powerful version of the Megalix tube from Siemens Healthineers. The advancement in tube design was the replacement of the amorphous silicone with crystalline silicone as the photo detector, which decreased electronic noise at the detector level and reduced radiation necessary to obtain images of the same quality. They found that a Gigalix tube and crystalline Si detector decreased radiation dose by 50 to 60% for fluoroscopy and cine acquisition in pediatric patients. This advancement will likely be extended into the adult cath lab.
Figure 7. Comparison of cath lab with no shielding (top), standard shielding with hanging shield and table skirt (middle), and EggNest- XR System (bottom). Courtesy of Dr. Robert Wilson.
Reduced frame rates also reduce x-ray dose. Radiologic software programs augment imaging systems to achieve excellent visibility at low x-ray dose levels for patients of all sizes. This unique software helps correct for motion, reduces noise, auto-enhances the image and corrects pixel shift on cine images. In addition, a new x-ray tube (Siemens Healthineers) that uses flat emitter technology enables smaller, square focal spots that may reduce exposure 70 percent, with improved visibility of small vessels and improved image quality.
Monitoring Dose in Real Time
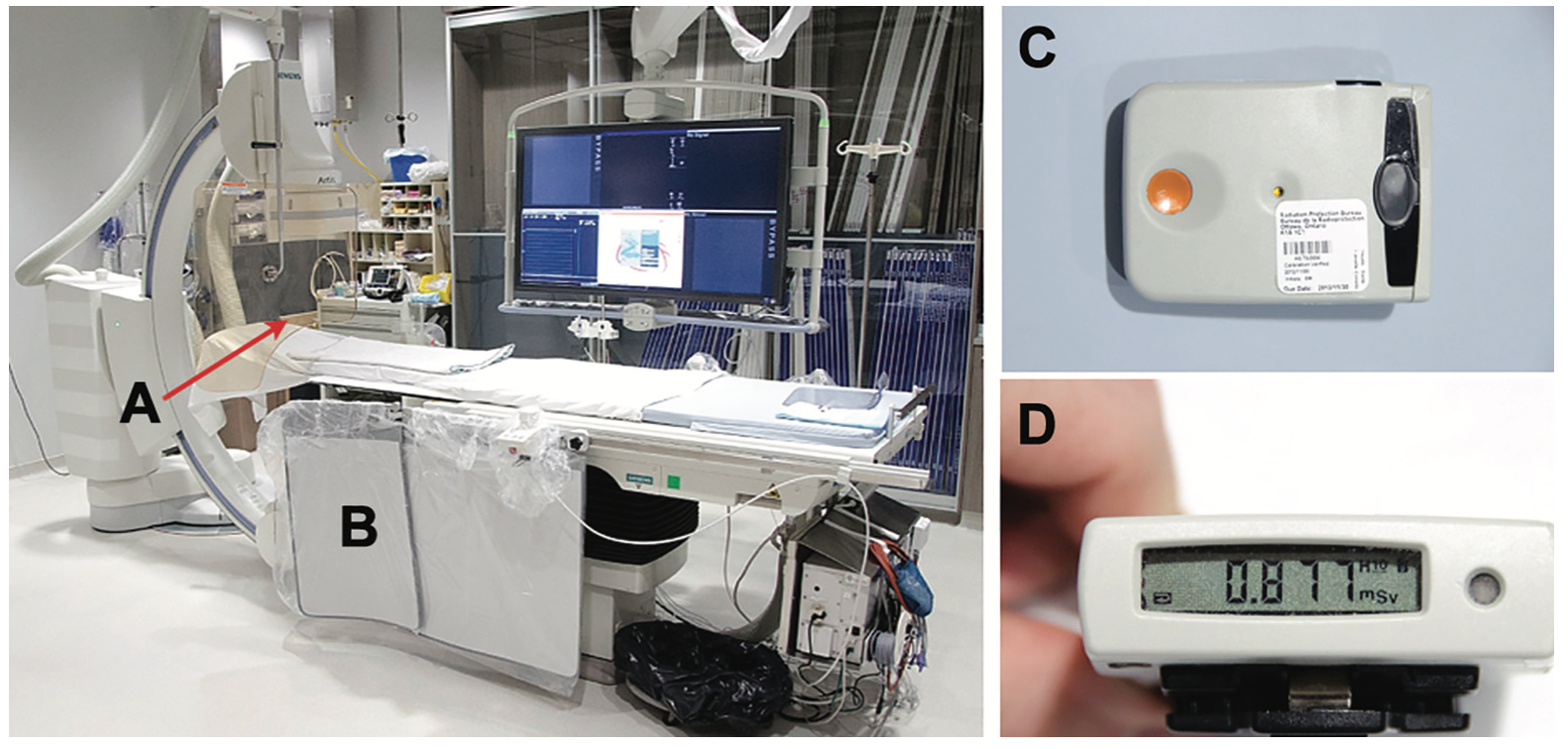
Figure 8A. Standard radiation protection equipment installed. (A) Ceiling-suspended acrylic shielding (1-mm lead equivalent), and (B) table-to-floor lead flap. (C) Electronic personal dosimeters worn by operators. An electronic personal dosimeter was worn on the left side of the thyroid lead shield and the recorded dose was absorbed by the operator during each case. (D) Electronic personal dosimeter screen display. Reprinted with permission from Abdelaal E et al; Interventional Cardiologists at Quebec Heart-Lung Institute. JACC Cardiovasc Interv. 2014 May; 7(5): 567-574. doi: 10.1016/j.jcin.2014.02.005.
The traditional radiation monitor badges are not very helpful because they only alert the badge’s wearer (a cath lab nurse, tech, or operator) to high levels of radiation well after the fact.6 Real-time exposure dosing can be obtained with one of several systems (Figure 8A-B). For example, the RaySafe i2 system (Unfors RaySafe) provides teams the ability to see their personal radiation exposure on an overhead display screen and move their location or make other changes (i.e., bring in an additional shield) to lower their exposure. The accumulated dose per individual user also is captured and displayed.
The Bottom Line
Figure 8B. Display of an electronic personal dosimeter readout. The badge owner can see the exposure and adjust their position as needed. Courtesy of Mentice.
In the cath lab, the majority of x-ray scatter radiation in any angiographic projection comes from below the mattress top. Angulated views significantly increase staff radiation exposure. Standard shielding provides modest protection for the angiographer positioned at the radial/femoral access sites, but no protection for the remainder of the staff or for procedures with head access. Mobile floor shields add protection for those circulating in the room. There are novel systems soon to be available (like the EggNest-XR System, among others) which can provide significantly better protection for both the physician and the staff in the room, and for all positions around the table. We should continue to work toward reducing radiation exposure and use the best protection operator techniques, methods, and equipment available.
References
Vlastra W, Delewi R, Sjauw KD, Beijk MA, Claessen BE, Streekstra GJ, et al. Efficacy of the RADPAD protection drape in reducing operators’ radiation exposure in the catheterization laboratory: a sham-controlled randomized trial. Circ Cardiovasc Interv. 2017 Nov; 10(11). pii: e006058. doi: 10.1161/CIRCINTERVENTIONS.117.006058.
Madder RD, LaCombe A, VanOosterhout S, Mulder A, Elmore M, Parker JL, et al. Radiation exposure among scrub technologists and nurse circulators during cardiac catheterization: the impact of accessory lead shields. JACC Cardiovasc Interv. 2017 Oct 25. pii: S1936-8798(17)31545-5. doi: 10.1016/j.jcin.2017.07.026. [Epub ahead of print]
Andreassi MG, Piccaluga E, Guagliumi G, Del Greco M, Gaita F, Picano E. Occupational health risks in cardiac catheterization laboratory workers. Circ Cardiovasc Interv. 2016 Apr; 9(4): e003273. doi: 10.1161/CIRCINTERVENTIONS.115.003273.
Fornell D. 5 technologies to reduce cath lab radiation exposure. Diagnostic and Interventional Cardiology. 2016 Aug 9. Available online at https://www.dicardiology.com/article/5-technologies-reduce-cath-lab-radiation-exposure. Accessed December 11, 2017.
Manu S, Suntharos P, Boyle GJ, Wang L, Prieto LR. Radiation reduction in the pediatric catheterization laboratory using a novel imaging system. J Invasive Cardiol. 2017 Oct 15. pii: JIC20171015-2. [Epub ahead of print]
Abdelaal E, Plourde G, MacHaalany J, Arsenault J, Rimac G, Déry JP, et al; Interventional Cardiologists at Quebec Heart-Lung Institute. Effectiveness of low rate fluoroscopy at reducing operator and patient radiation dose during transradial coronary angiography and interventions. JACC Cardiovasc Interv. 2014 May; 7(5): 567-574. doi: 10.1016/j.jcin.2014.02.005.
Disclosure: Dr. Kern is a consultant for Abiomed, Merit Medical, Abbott Vascular, Philips Volcano, ACIST Medical, Opsens Inc., and Heartflow Inc.
The Cleerly Polygenic Cardiovascular Risk Score Test, powered by Allelica’s proprietary multi-ancestry PRS technology, gives physicians a new option to identify and evaluate patients with an inherited predisposition to coronary plaque.
The Cleerly Polygenic Cardiovascular Risk Score Test, powered by Allelica’s proprietary multi-ancestry PRS technology, gives physicians a new option to identify and evaluate patients with an inherited predisposition to coronary plaque.
First and only biomarker to measure coronary inflammation and assess cardiovascular mortality risk, enabling personalized disease management. CaRi-Heart Risk score identifies cardiovascular risk 10 years in advance.
First and only biomarker to measure coronary inflammation and assess cardiovascular mortality risk, enabling personalized disease management. CaRi-Heart Risk score identifies cardiovascular risk 10 years in advance.
Implicity’s newly cleared ILR ECG algorithm can now analyze data from ICMs across all major device manufacturers, including Abbott, Biotronik, Boston Scientific, and Medtronic.
Implicity’s newly cleared ILR ECG algorithm can now analyze data from ICMs across all major device manufacturers, including Abbott, Biotronik, Boston Scientific, and Medtronic.
ESC Press Release
Sophia Antipolis, France – 23 July 2026: The results of 59 ground-breaking trials will be unveiled for the first time at ESC Congress 2026, the annual congress of the European Society of Cardiology, which takes...
ESC Press Release
Sophia Antipolis, France – 23 July 2026: The results of 59 ground-breaking trials will be unveiled for the first time at ESC Congress 2026, the annual congress of the European Society of Cardiology, which takes...
ALAMEDA, Calif. – Penumbra, Inc. announced the results of THUNDER, an Investigational Device Exemption (IDE) study, to evaluate the safety and effectiveness of THUNDERBOLT™, the company’s novel...
ALAMEDA, Calif. – Penumbra, Inc. announced the results of THUNDER, an Investigational Device Exemption (IDE) study, to evaluate the safety and effectiveness of THUNDERBOLT™, the company’s novel...
Researchers at the LKS Faculty of Medicine of the University of Hong Kong (HKUMed) have developed an artificial intelligence tool that may help predict serious cardiovascular problems many years before symptoms appear.
The system, known as...
Researchers at the LKS Faculty of Medicine of the University of Hong Kong (HKUMed) have developed an artificial intelligence tool that may help predict serious cardiovascular problems many years before symptoms appear.
The system, known as...
WASHINGTON —The American College of Cardiology (ACC) is introducing a new cardiogenic shock designation to improve outcomes for one of the most life-threatening complications of a heart attack. The new designation builds on the success of the...
WASHINGTON —The American College of Cardiology (ACC) is introducing a new cardiogenic shock designation to improve outcomes for one of the most life-threatening complications of a heart attack. The new designation builds on the success of the...
CAMPBELL, Calif., July 16, 2026 — Imperative Care, a medical technology company focused on advancing treatments for patients suffering from thromboembolic disease, today announced the launch of the Ikon™ 24 Pro Guidewire, a next-generation...
CAMPBELL, Calif., July 16, 2026 — Imperative Care, a medical technology company focused on advancing treatments for patients suffering from thromboembolic disease, today announced the launch of the Ikon™ 24 Pro Guidewire, a next-generation...
At week 24 in the CORALreef Lipids and CORALreef HeFH trials, Merck's LIPFENDRA significantly reduced LDL-C by a placebo-adjusted 56% and 59%, respectively.
At week 24 in the CORALreef Lipids and CORALreef HeFH trials, Merck's LIPFENDRA significantly reduced LDL-C by a placebo-adjusted 56% and 59%, respectively.
Serotonin is usually associated with mood, sleep, and digestion. But research published in 2023 suggests this chemical messenger may also influence a small structure that performs a vital job during every heartbeat: the mitral valve.
The...
Serotonin is usually associated with mood, sleep, and digestion. But research published in 2023 suggests this chemical messenger may also influence a small structure that performs a vital job during every heartbeat: the mitral valve.
The...