Clinical Editor's Corner
Time to Review Your Radial Practice for Best Results
September 2017
The increasing use of the radial artery approach in the United States over the last decade has been dramatic and yet the acceptance of the procedure among many interventionalists remains somewhat tentative. The RIVAL1 and MATRIX2 trials provided strong supporting evidence for use of transradial access (TRA) in acute coronary syndromes, since TRA was associated with a 27-32% reduction in major bleeding and a 14-27% improvement in mortality rates.3 From these results, TRA is currently the recommended access route for patients undergoing coronary angiography and intervention.3,4 On a personal note, after transitioning from the all-femoral approach to about 90% radial access in our VA and University cath labs today, we have truly appreciated the benefits of the TRA method: less bleeding, more patient comfort, more security in the post procedure course, and early discharge for both diagnostic and percutaneous coronary intervention (PCI) cases. Although my colleagues and I may struggle with a few cases involving tortuosity, short stature, or complex coronary artery bypass graft (CABG) anatomy, we have the great satisfaction of knowing that the procedure was completed safely, and that the patient and his/her family and the nurses are highly satisfied that the patient will do well after discharge. It is also gratifying that we no longer have the same fear of retroperitoneal bleeding and the other complications of the femoral approach.
While perusing the literature, I was impressed with a recent article by Obaid et al5 describing their experience with balloon-assisted tracking to improve radial artery access success, especially during primary PCI for ST-elevation myocardial infarction (STEMI), as well as an accompanying editorial by Dr. James Blankenship6. This article reminded me how far we’ve come with radial access in the last few years. I thought it would be a good idea to review opportunities in front of us in order to continue improving our TRA.
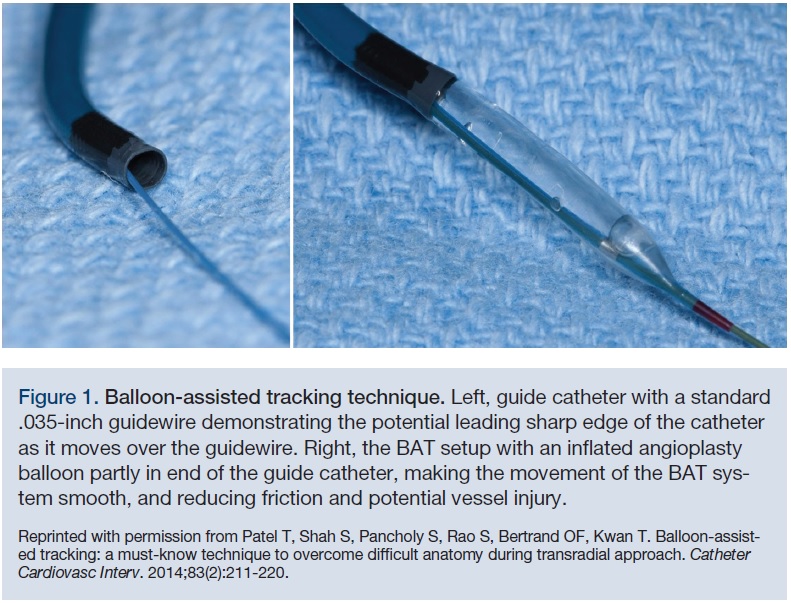 Dr. Obaid and the interventionalists from Morristown Cardiac Centre, Swansea, United Kingdom, reported on their radial artery access success before and after use of the balloon-assisted tracking technique. Balloon-assisted tracking (BAT) is a particularly useful technique to overcome both arterial loops and extreme tortuosity.7 BAT puts a smooth, tapered tip (the balloon) in front of the diagnostic or guide catheter to ease passage through a tortuous or vasospastic arm artery (Figure 1). The method is as follows:
Dr. Obaid and the interventionalists from Morristown Cardiac Centre, Swansea, United Kingdom, reported on their radial artery access success before and after use of the balloon-assisted tracking technique. Balloon-assisted tracking (BAT) is a particularly useful technique to overcome both arterial loops and extreme tortuosity.7 BAT puts a smooth, tapered tip (the balloon) in front of the diagnostic or guide catheter to ease passage through a tortuous or vasospastic arm artery (Figure 1). The method is as follows: 1) Insert a .014-inch soft-tipped guidewire through the guide as we would do for angioplasty, past the difficult arterial segment;
2) Advance a small PCI balloon (2 mm diameter) into the guide, positioning it at the end of the guide catheter, partially protruding from the distal end of the diagnostic or guiding catheter;
3) Inflate the balloon at low pressures (3–6 atmospheres [atm]);
4) Advance the catheter-balloon assembly over the guidewire, thus eliminating a sharp edge of the guide catheter, and facilitating a smooth and atraumatic advancement of the catheter through the difficult vascular anatomy.
Looking at 2223 consecutive patients undergoing PCI from the radial approach, Obaid et al5 found fewer crossovers to femoral access after using BAT compared to a similar period of time before using BAT technique. During the initial study period, 1334 radial PCIs were attempted with a crossover rate of 26 patients to femoral at an early stage and 76 patients with radial artery spasm who underwent successful BAT in 69 cases (91%) with a total crossover rate of only 2.5%. Using BAT rather than switching to the femoral puncture reduced the TRA-to-transfemoral (TF) crossover rate from 7.6 to 2.5% (P<0.01), which was lower than the crossover rate of 6.1% in the 12 months occurring before BAT. Moreover, the BAT technique did not delay reperfusion with primary PCI.
 In his editorial6, Dr. James C. Blankenship, former president of the Society for Cardiovascular Angiography and Interventions (SCAI) commented not only on BAT performance, but also highlighted additional aspects of the procedure to become a “complete radialist”. I have taken the liberty of repeating portions of these complementary and comprehensive descriptions. Dr. Blankenship notes that many of these procedures are available, but not all are necessary. He cites the following from his experience (we have added a couple of helpful hints along the way as well):
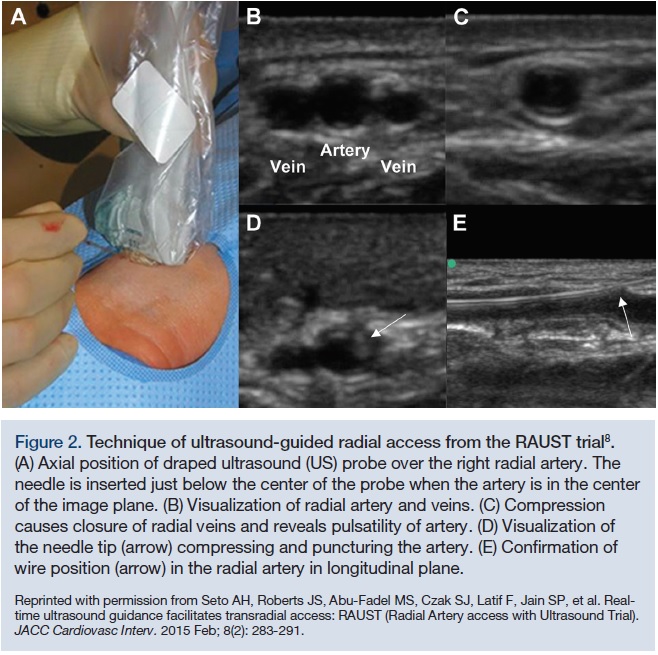
In his editorial6, Dr. James C. Blankenship, former president of the Society for Cardiovascular Angiography and Interventions (SCAI) commented not only on BAT performance, but also highlighted additional aspects of the procedure to become a “complete radialist”. I have taken the liberty of repeating portions of these complementary and comprehensive descriptions. Dr. Blankenship notes that many of these procedures are available, but not all are necessary. He cites the following from his experience (we have added a couple of helpful hints along the way as well):- Ultrasound for radial puncture increases access success (Figure 2). Dr. Arnold Seto from University of California Irvine and the RAUST investigators8 convincingly provide support for this addition to our radial toolbox.
 The ulnar artery can be used as an alternative to access root and should be considered before abandoning the TRA. Keep the ulnar artery in mind when the radial artery is too small, too tortuous, or too stubborn (spastic) (Figure 3). A recent CLD Editor’s page9 describes our experience and the utility of transulnar access (TUA) when the standard radial access fails.
The ulnar artery can be used as an alternative to access root and should be considered before abandoning the TRA. Keep the ulnar artery in mind when the radial artery is too small, too tortuous, or too stubborn (spastic) (Figure 3). A recent CLD Editor’s page9 describes our experience and the utility of transulnar access (TUA) when the standard radial access fails.- Use of the contralateral radial access makes good sense if we believe in TRA. Switching to the femoral for TRA failure should be done if both arms are impassable due to bilateral tortuosity, radial loops, or calcific arm arteries (e.g., Monkenberg’s medial sclerosis).
- Perform early angiographic imaging of the brachial bifurcation when difficulty in catheter advancement up the arm occurs. An angiogram may show that the wire passed up a recurrent radial artery branch too small to permit catheter passage. This small branch is often associated with a radial loop, which can be traversed on further appropriate wire manipulation or by BAT. It is worth using angulated views of the brachial bifurcation, since the bifurcation may be difficult to define. Angulated views of 30 degrees left or right anterior oblique may help.
- Consider sheathless 7 French guides for PCI when larger equipment or bifurcation stenting is planned.
- When tortuous or spasmodic arteries are encountered, use BAT as noted above. In addition, hydrophilic sheaths and 5 French (F) catheters inside of a 6F catheter may also reduce friction and help catheter passage. Also remember, rotating the guide as it passes proximally around vessel curvature may also facilitate passage without inducing more spasm. If possible, limit the number of catheter exchanges.
 Apply antispasm cocktails early. In some labs, the use of antispasm cocktails is reserved for those arteries that become spastic. We still start our procedure with intraarterial (IA) verapamil (250 mcg) only. Intravenous (IV) heparin is routine, but we no longer give IA heparin because of the discomfort during injection.
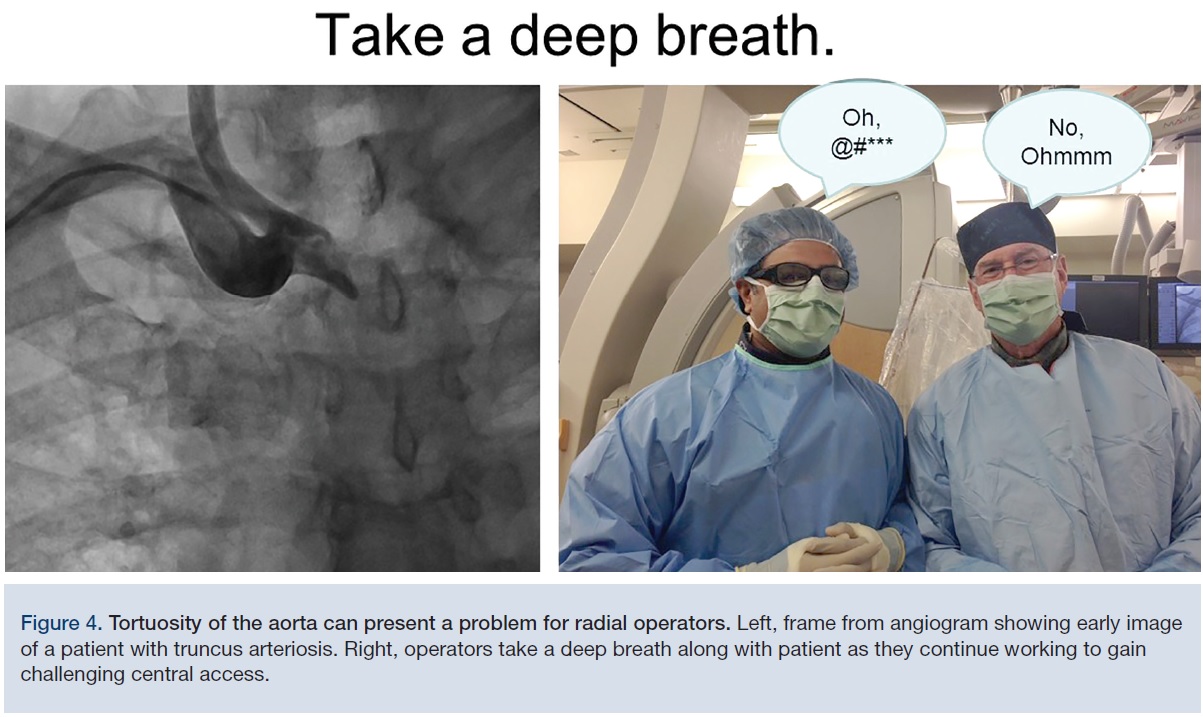
Apply antispasm cocktails early. In some labs, the use of antispasm cocktails is reserved for those arteries that become spastic. We still start our procedure with intraarterial (IA) verapamil (250 mcg) only. Intravenous (IV) heparin is routine, but we no longer give IA heparin because of the discomfort during injection.- Negotiating innominate or subclavian artery tortuosity may require particularly shaped catheters coupled with softer/harder guidewires. A deep breath by the patient pulls the vascular structures downward, straightening some of the curvature and helping pass the catheter to the ascending aorta (Figure 4).
- For patients shorter than 5’5’’, we routinely use the left radial artery to reduce the difficulty of negotiating a sharp angle into the ascending aorta from the right side.
- Beware of aberrant aortic arches, including arteria lusoria (anomalous path of right subclavian artery behind the esophagus) and a bovine aortic arch (also see Figure 4) where the innominate trunk is moved centrally and leftward, making the turn down to the ascending aorta difficult.
 Coronary catheter seating and manipulation is improved when operators have experience with several catheters. Patience and practice will determine catheter selection after the standard shapes fail. Beware of deep seating with the Jacky (Terumo), especially for the right coronary artery (RCA). The TIG (Terumo) is our first choice for training fellows in the technique.
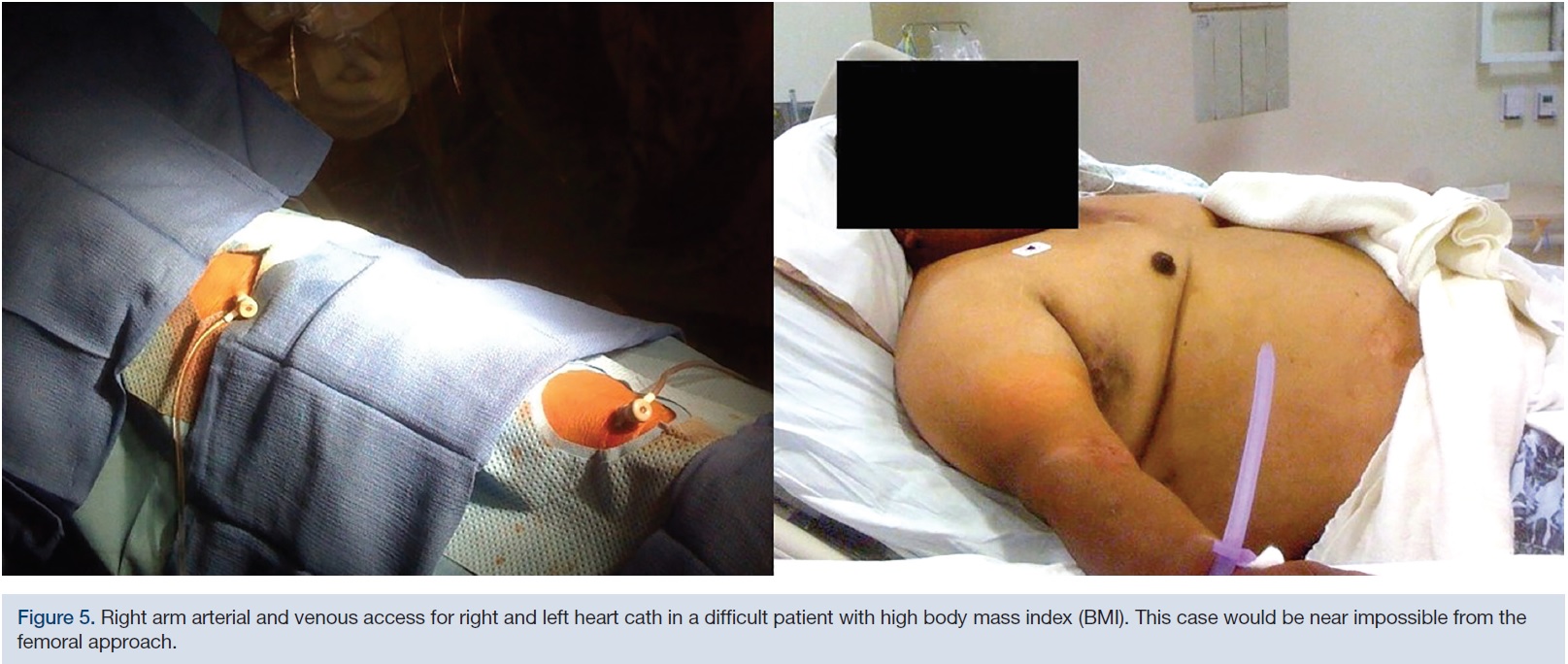
Coronary catheter seating and manipulation is improved when operators have experience with several catheters. Patience and practice will determine catheter selection after the standard shapes fail. Beware of deep seating with the Jacky (Terumo), especially for the right coronary artery (RCA). The TIG (Terumo) is our first choice for training fellows in the technique.- A right heart cath from the arm should no longer present a problem for the radial approach (Figure 5). We have successfully used a brachial vein (at times, requiring ultrasound access). The medially oriented brachial vein is better than the lateral cephalic vein, because of the acute angle (T-junction) that the cephalic vein takes entering into the subclavian vein. We start with a 16g angiocath placed in the vein before the procedure; then, using a micropuncture guidewire, we exchange the angiocath for a 5F sheath in the brachial vein. A 5F pediatric balloon-tipped pulmonary artery catheter can then be easily positioned for right heart hemodynamics and estimated cardiac output from oxygen saturation samples. A femoral vein access should not be necessary.
 I hope this review of several specific suggestions will be helpful while you examine your radial approach track record. For more details on a particular approach or anomalies, there are several excellent compendiums of radial operator techniques and recommendations.10,11 For best TRA success, keep these helpful hints in mind as “Radial First” (Figure 6) becomes the default approach to cardiac catheterization.
I hope this review of several specific suggestions will be helpful while you examine your radial approach track record. For more details on a particular approach or anomalies, there are several excellent compendiums of radial operator techniques and recommendations.10,11 For best TRA success, keep these helpful hints in mind as “Radial First” (Figure 6) becomes the default approach to cardiac catheterization. References
- Valgimigli M, Gagnor A, Calabró P, Frigoli E, Leonardi S, Zaro T, et al; MATRIX Investigators. Radial versus femoral access in patients with acute coronary syndromes undergoing invasive management: A randomised multicentre trial. Lancet. 2015; 385: 2465-2476.
- Jolly SS, Yusuf S, Cairns J, Niemelä K, Xavier D, Widimsky P, et al. Radial versus femoral access for coronary angiography and intervention in patients with acute coronary syndromes (RIVAL): A randomised, parallel group, multicentre trial. Lancet. 2011; 377: 1409-1420.
- Azzalini L, Jolicoeur EM. The wise radialist’s guide to optimal transfemoral access: Selection, performance, and troubleshooting. Catheter Cardiovasc Interv. 2017 Feb 15; 89(3): 399-407.
- Windecker S, Kolh P, Alfonso F, et al. ESC/EACTS Guidelines on myocardial revascularization: the task force on myocardial revascularization of the European Society of Cardiology (ESC) and the European Association for Cardio-Thoracic Surgery (EACTS). Eur Heart J. 2014; 35: 2541-2619.
- Obaid D, Hailan A, Chase A, Dorman S, Jenkins G, Raybould A, et al. Balloon assisted tracking use reduces radial artery access failure in an experienced radial center and is feasible during primary PCI for STEMI. J Invasive Cardiol. 2017; 29: 219-224.
- Blankenship JC. The complete radialist. J Invasive Cardiol. 2017; 29(7): 225-226.
- Patel T, Shah S, Pancholy S, Rao S, Bertrand OF, Kwan T. Balloon-assisted tracking: A must-know technique to overcome difficult anatomy during transradial approach. Catheter Cardiovasc Interv. 2014; 83: 211-220.
- Seto AH, Roberts JS, Abu-Fadel MS, Czak SJ, Latif F, Jain SP, et al. Real-time ultrasound guidance facilitates transradial access: RAUST (Radial Artery access with Ultrasound Trial). JACC Cardiovasc Interv. 2015 Feb; 8(2): 283-291.
- Kern MJ and Seto AH. Radial access failure: when should we go ulnar? Cath Lab Digest. 2016 Nov; 24(11). Available online at https://www.cathlabdigest.com/article/Radial-Access-Failure-When-Should-We-Go-Ulnar. Accessed August 14, 2017.
- Patel T, Shah S, Pancholy SB, eds. Patel’s atlas of transradial intervention: The basics and beyond. Malvern, PA: HMP Communications, LLC; 2012.
- Bertrand O, Rao S. Best practices for transradial approach in diagnostic angiography and intervention. Philadelphia, PA: Lippincott Williams & Wilkins; 2015.
Disclosure: Dr. Kern is a consultant for Abiomed, Merit Medical, Abbott Vascular, Philips Volcano, ACIST Medical, Opsens Inc., and Heartflow Inc.
Subscriber
Cath Lab Digest Newsletter