


Complications of Transradial Catheterization Series: Radial Artery Dissection
A 72-year-old female was referred for cardiac catheterization because of New York Heart Association (NYHA) class III heart failure symptoms, angina, and inferior wall ischemia on the stress Myoview imaging test. Her past medical history included hypertension, diabetes, dyslipidemia, and coronary artery disease. She was treated with coronary artery bypass surgery in 2011 with a saphenous vein graft (SVG) to the right coronary artery (RCA) and to the left anterior descending artery (LAD). The patient was pre-treated with dual antiplatelet treatment of aspirin and clopidogrel (Plavix, Bristol Myers-Squibb). Other medications included glipizide, glucophage, Lopressor (Novartis), Crestor (AstraZeneca), and lisinopril. The physical examination was remarkable only for bilateral lower extremity 1+ pitting edema and a scar from the surgery.
Right radial artery (RA) access was chosen for the procedure, as the patient did not have a left internal mammary artery (LIMA) graft. We routinely use the Seldinger technique (posterior wall puncture or through-and-through puncture) to obtain radial artery access. After the local anesthetic infiltration, a 20-gauge Teflon-coated Angiocath needle (B. Braun) was used to obtain access. Skin was entered at a 45-degree angle and after entering the anterior wall of the radial artery, a flash of blood was seen in the transparent hub of the Angiocath. At this point, the Angiocath was advanced further and the posterior wall was punctured. The stylet was removed and a 0.021-inch guide wire (supplied with the Terumo Glide Access Kit, Terumo Corporation) was placed in the hub of the Teflon cannula and the entire system was very gradually withdrawn. When the pulsatile flow was seen in the hub of the Teflon cannula, the guide wire was advanced. After advancing 2-3 inches, some resistance was felt. The wire then advanced about 6-7 inches further and at that point, there was significant resistance. To confirm the intraluminal course of the wire, the Teflon cannula was advanced over the wire into the RA. There was pulsatile flow, but not as brisk. An angiogram was performed by injecting diluted contrast through the Teflon cannula. The radial artery angiogram showed radial artery dissection (Figure 1).

A 0.014-inch Prowater wire (Abbott Corporation) was given a 35- to 45-degree shape and was tactfully advanced into the RA. As the wire entered a side branch, it was reassuring that the wire was in the true lumen and unlikely to be in the false lumen. The wire was then advanced further through a tortuous course of the RA originating from the axillary artery (Figure 2).

A 6 French hydrophilic-coated sheath (Terumo) was advanced over the 0.014-inch wire. A vasodilator cocktail of 5 mg of diltiazem and 200 mcg of nitroglycerin was administered intra-arterially via the introducer sheath. Fifty units per kilogram unfractionated heparin was administered intravenously after introducer sheath placement.
The coronary angiogram showed a 100% occluded proximal RCA and a long area of heavily calcified 90% stenosis in the mid LAD. The left main and left circumflex arteries were patent with mild disease. The SVG to the LAD was widely patent with mild degenerative changes and an excellent run-off to the LAD. The SVG to the RCA had severe proximal and body of the graft stenosis (Figure 3).
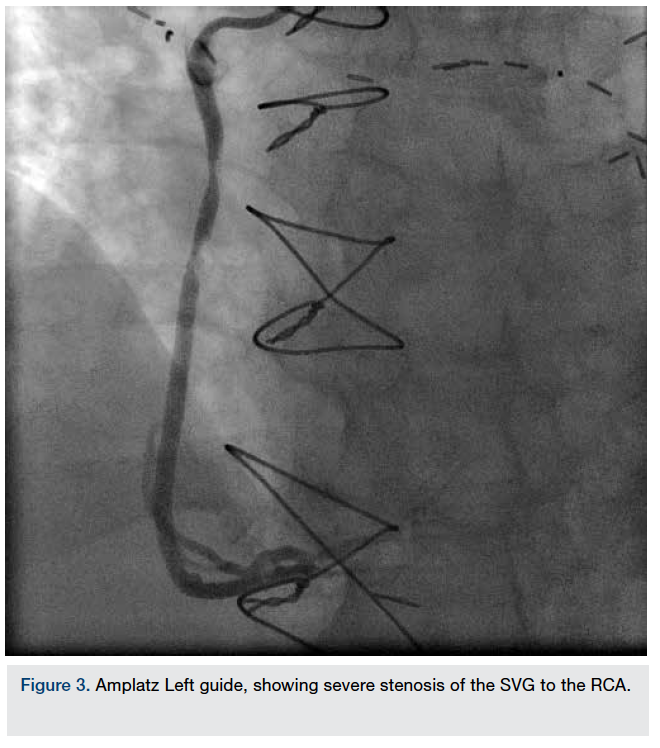
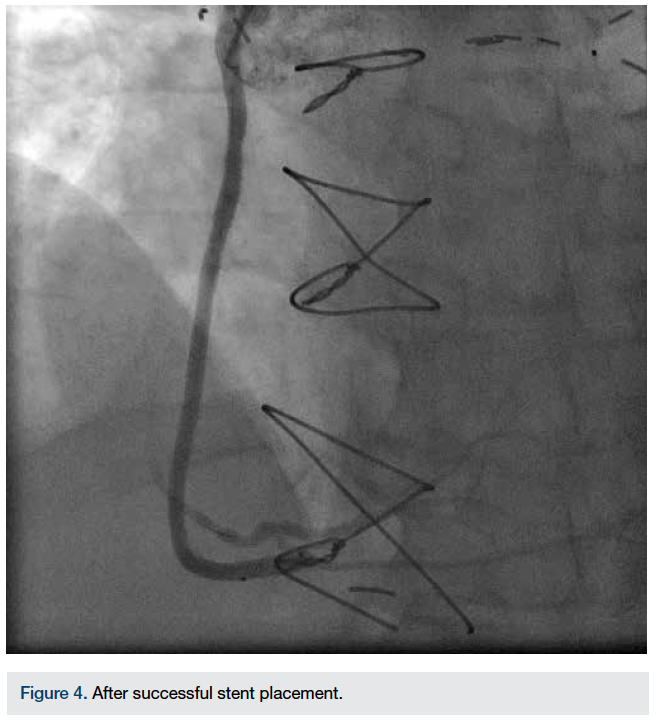
A 6 French Amplatz Left (AL) 2 guide was used to cannulate the SVG to the RCA. Additional heparin was used for weight-based anticoagulation. After deploying a 5 mm Spider filter (ev3) in the SVG to the RCA, a 4.0 x 26 mm Integrity bare-metal stent (Medtronic) was deployed by direct stenting, with a good final angiographic result (Figure 4).
The guide catheter was removed over the J wire and a final angiogram of the RA was performed through the sheath (Figure 5).
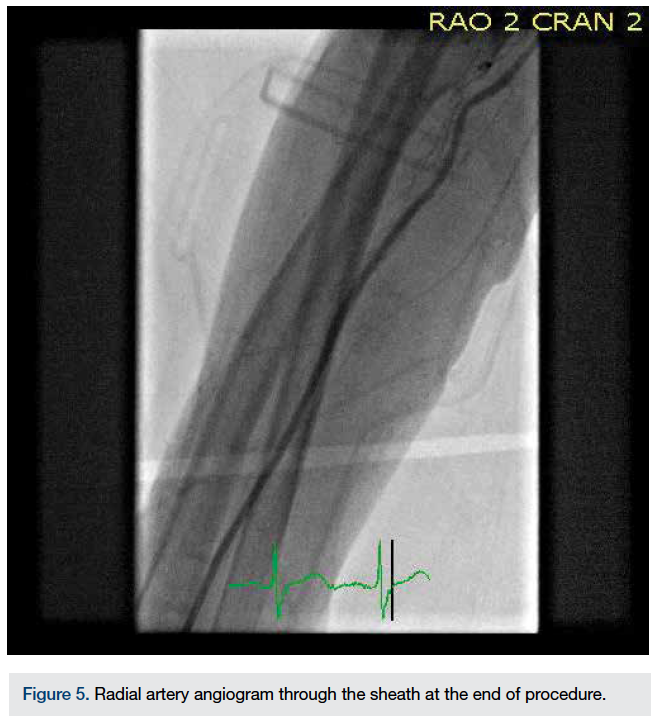
There was normal flow in the RA and no dissection was seen. The sheath was removed and a TR Band (Terumo) applied for hemostasis. Patent hemostasis protocol was followed. After 16 hours, at the time of discharge, the RA was patent on a reverse Barbeau test.
Discussion
Access-related complications are significantly lower with RA access in comparison to femoral artery access.1 Even though it is rare, RA access can be complicated by RA dissection, perforation, or radial artery occlusion. Most of these complications can be managed without any further long-term sequelae or clinical impairment. In this case, the RA dissection was dealt with by continuing the procedure through the same RA access. A retrograde dissection may have healed if the 20-gauge access was abandoned, but it would have required us to change to another access. A true lumen wire advancement was crucial; therefore, we preferred to use the 0.014-inch wire. The RA sheath or catheter works as an internal hemostatic device and helps seal the dissection or even perforation.2
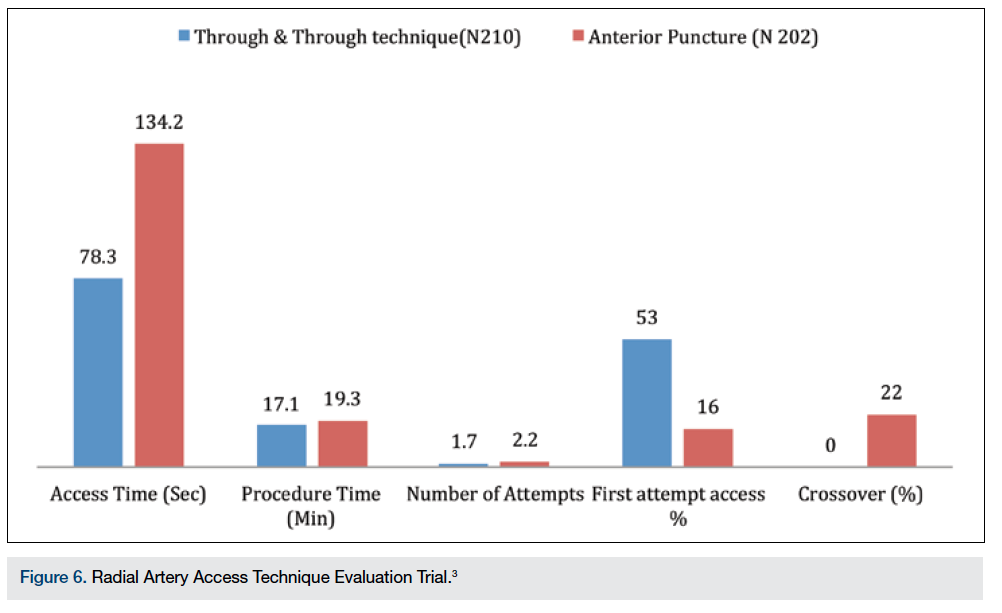
There are two ways to obtain RA access: via a modified Seldinger technique (anterior wall puncture only) or Seldinger technique (posterior wall puncture or through-and-through puncture). We reported in a randomized trial that the through-and-through puncture technique was a faster and probably a more reliable way to obtain radial artery access with shorter procedure time, shorter time to gain access, and required a fewer number of attempts to gain radial artery access, as well as no crossovers. There were no differences in procedure-related complications such as hematoma formation or RA occlusion (Figure 6).3
The following tips may increase the success of the radial artery access and reduce the chances of complications:
- It is very important to feel for any resistance as the wire is advanced in the RA. It is very easy for a wire to travel in sub-intimal space and rarely, even through the posterior wall, if a bare needle is partially in the posterior wall (applicable in the anterior puncture technique).
- If there is any resistance encountered, instead of pushing the wire further, it should be pulled back and an angled wire should be steered through.
- At times, resistance is felt after advancing few centimeters of the 0.021-inch wire because of distal RA tortuosity. In this situation, if the through-and-through technique is used, the Teflon cannula can be inserted over the wire. Remove the wire. If your cannula is intraluminal, there will be pulsatile blood flow. Diluted contrast can be injected to define the anatomy through the Teflon cannula (non-diluted contrast causes burning pain).
- A vasodilator cocktail can be injected into the RA if there is spasm.
- When tactile resistance is encountered while advancing the wire, fluoroscopy should be used. Defining any variation in the upper limb arterial anatomy with contrast allows for successful negotiation and avoids complications.
- Use a 0.014-inch workhorse wire to negotiate through radial tortuosity.
- Completing the procedure through the same RA access often treats the complication of access.
- Irrespective of the situation, patent hemostasis protocol must be followed and immediate removal of the sheath is mandatory after completion of the procedure.
Disclosure: The authors report no conflicts of interest regarding the content herein.
Dr. Cholankeril and Dr. Sanghvi may be contacted via Dr. Kintur Sanghvi at SanghviK@Deborah.org.
References
- Jolly SS, Amlani S, Hamon M, Yusuf S, Mehta SR. Radial versus femoral access for coronary angiography or intervention and the impact on major bleeding and ischemic events: a systematic review and meta-analysis of randomized trials. Am Heart J. 2009; 157: 132-140.
- Patel T, Sanghvi K, Pancholy S. Management of radial and brachial artery perforations during transradial procedures — a practical approach. J Invasive Cardiol. 2009 Oct; 21(10): 544-547.
- Pancholy S, Sanghvi K, Patel T. Radial artery access technique evaluation trial: randomized comparison of Seldinger versus modified Seldinger technique for arterial access for transradial catheterization. Catheter Cardiovasc Interv. 80(2): 288-291.



