A Paradigm Shift in the Treatment of Valvular Heart Disease: Transcatheter Aortic Valve Implantation (TAVI)
 Note: This article has undergone correction since print publication. See asterisks in the text and at the end for specified corrections.
For years, Corazon has witnessed increasing “turf battles” between cardiac surgeons and interventional cardiologists with respect to the treatment of coronary artery disease. More
aggressive reperfusion strategies, coupled with advanced technologies, have enabled the interventional cardiologist to continue to treat patients who would have once been deemed surgical candidates for coronary artery bypass grafting (CABG).
Note: This article has undergone correction since print publication. See asterisks in the text and at the end for specified corrections.
For years, Corazon has witnessed increasing “turf battles” between cardiac surgeons and interventional cardiologists with respect to the treatment of coronary artery disease. More
aggressive reperfusion strategies, coupled with advanced technologies, have enabled the interventional cardiologist to continue to treat patients who would have once been deemed surgical candidates for coronary artery bypass grafting (CABG).
In consideration of declining CABG surgeries nationwide, the Corazon team has had discussions with cardiac surgeons related to keeping their volumes stable. In these meetings, there is typically a ‘sigh of relief’ due to limitations in terms of eligible treatments for structural heart disease and the necessity for open surgery to treat conditions such as valvular disease. In fact, we often work with surgeons to bolster their volumes and outcomes specific to valve cases, so that cardiac surgery services as whole can be viewed as an ongoing, viable component to a full-service cardiac program.
However, a new strategy for maintaining adequate total cardiac procedure volumes and competency must emerge. The last decade has literally been bursting with new and often very disruptive technologies that allow cardiovascular disease to be treated with the most minimally-invasive techniques that have ever been witnessed. It now appears that all cardiovascular conditions requiring anatomical intervention are amenable to endovascular and/or transcatheter approaches to care. Valvular disease is no exception! The last year has seen a tremendous interest in valve disease treatment based on solely on transcatheter techniques. This practice has shifted the operating room-type patient of yesterday into a catheterization lab or hybrid suite today. Though, fortunately, there appears to be a collaborative approach emerging among interventional cardiologists and cardiac surgeons, especially as the industry ventures into technologically-advanced procedure techniques that capitalize on all these specialists’ skill sets.
Presently, much of the focus for a catheter-based approach to valve care has been directed at aortic stenosis. A recent outpouring in the literature has resulted, as initial results related to transcatheter aortic valve implantation (TAVI) have shown great promise in high-risk patient populations.
Catheter-based techniques for what is essentially a valve replacement procedure are not as new as one might think. In fact, the first TAVI was performed in 2002 in Europe. Due to FDA restrictions, clinical trials did not commence in the United States until 2007, and recent results from the PARTNER (Placement of Aortic Transcatheter Valve Trial) were a significant highlight at the 2010 Transcatheter Cardiovascular Therapeutics (TCT) conference. There are currently 22 hospitals in the U.S. and 26 worldwide participating in the PARTNER trial.1 All of the participating facilities are large quaternary centers that are very experienced in the treatment of cardiovascular disease, with the principal investigators based at New York-Presbyterian Hospital/Columbia University Medical Center. The PARTNER trial has an estimated enrollment of 1,040 patients (active recruiting ended in March and August of 2009). It is anticipated that the study will conclude in late 2014.
As a manager or clinical professional in the cardiac cath lab, you may be familiar with the TAVI procedure. If you are one of the many who do not have the privilege of working in one of the centers in the PARTNER trial, you might be wondering what all this “buzz” is about.
Aortic stenosis is the most common valvular disease in our aging population, with a prevalence of 4.6% in adults over the age 75.2 This patient population is also fraught with multiple cardiovascular co-morbidities, such as diabetes, renal impairment, and fulminate vascular disease, which may mean that a standard open surgical approach to treatment is not feasible. The number of patients who have already received a catheter-based treatment for AS already exceeds 5,000 worldwide. During the TCT conference, Dr. Martin Leon, one of the principal investigators for the PARTNER trial, indicated that “balloon-expandable TAVI should be the new standard of care for patients with aortic stenosis who are not suitable candidates for surgery.”3
Devices
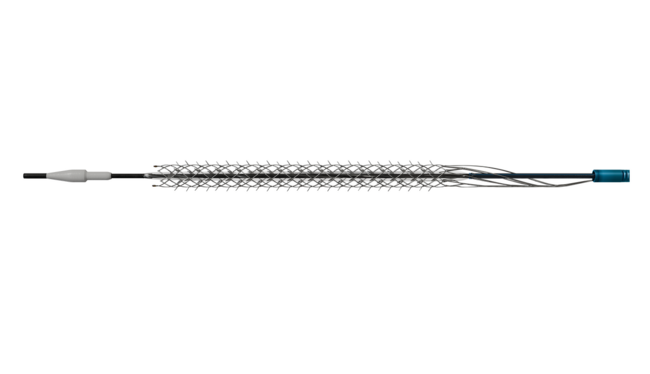
There are currently two devices available for performing the TAVI procedure. Edwards  Lifesciences manufactures the Sapien Transcatheter Valve (Figure 1) and Medtronic produces the CoreValve device. The Sapien Transcatheter valve is undergoing rigorous study through the PARTNER trial.* The Sapien valve is balloon-expandable and available in 23 mm and 26 mm sizes. The valve consists of a stainless steel frame with an integrated tri-leaflet bovine pericardial valve. The latest version of this valve has been reconstructed with a chromium cobalt frame.
Lifesciences manufactures the Sapien Transcatheter Valve (Figure 1) and Medtronic produces the CoreValve device. The Sapien Transcatheter valve is undergoing rigorous study through the PARTNER trial.* The Sapien valve is balloon-expandable and available in 23 mm and 26 mm sizes. The valve consists of a stainless steel frame with an integrated tri-leaflet bovine pericardial valve. The latest version of this valve has been reconstructed with a chromium cobalt frame.
In contrast, the Medtronic CoreValve (Figure 2) is similarly not commercially available in the U.S., though the FDA granted conditional approval for a trial in October 2010.** Thus, clinical  trials in the U.S. are expected to be underway very soon in 2011. Medtronic has been in the process of selecting sites for the U.S. clinical trial, and was hoping to enroll patients as far back as the summer of 2010, though it was delayed due to the lack of FDA approval at that time.4 The Medtronic device is a self-expanding valve. It that used to be criticized by European operators as requiring too complex an implant procedure, but with new improvements, operators now claim it can be implanted with very little hemodynamic support.5 The CoreValve also presents a very promising future, as the lower structural profile of the device may allow for alternative implant approaches.
trials in the U.S. are expected to be underway very soon in 2011. Medtronic has been in the process of selecting sites for the U.S. clinical trial, and was hoping to enroll patients as far back as the summer of 2010, though it was delayed due to the lack of FDA approval at that time.4 The Medtronic device is a self-expanding valve. It that used to be criticized by European operators as requiring too complex an implant procedure, but with new improvements, operators now claim it can be implanted with very little hemodynamic support.5 The CoreValve also presents a very promising future, as the lower structural profile of the device may allow for alternative implant approaches.
It should be noted that other companies are looking to venture into this projected high-growth market. Boston Scientific’s recent purchase of Sadra Medical, which develops the Lotus Valve system, a stent-mounted valve prosthesis and catheter delivery system, recently received serious industry attention. However, the most immediate access to these devices remains with the Edwards Lifesciences Sapien Valve, followed by Medtronic’s transcatheter valve system.
Patient Selection & Screening
The exciting outcomes reported in the PARTNER clinical trial appear to have appropriate patient selection as an important factor. The TAVI procedure is intended to act as an interventional therapy for patients who cannot tolerate the risk of traditional open-heart surgery, which poses other risks such as the need for cardiopulmonary bypass. Other potential indications include a porcelain aorta and previous mediastinal radiotherapy.6 Once again, collaboration is key! Patients should be selected for TAVI by a multi-disciplinary team that includes interventional cardiologists, cardiac surgeons, cardiac anesthesiologists, and imaging specialists.
Patients must be in stable condition prior the procedure, as their cardiac function must be preserved to sustain optimal hemodynamics during the implant procedure. Those in decompensated heart failure with severely depressed left ventricular function should undergo medical optimization and possible balloon valvuloplasty to allow for improvement in ventricular function, along with stress echocardiography to assess myocardial contractility reserve.
Immediate access to state-of-the-art, non-invasive diagnostics is essential for centers looking to perform TAVI procedures in the future. For example, the optimal plane for valve deployment is determined by 3-dimensional (3D) computed tomography (CT) prior to the procedure. Precise measurement of the aortic annulus diameter for valve sizing is important to ensure that the transcatheter system is able to “seat” the implant correctly. The 23 mm Sapien valve is available for annular sizes of 18-21 mm and the 26 mm valve is designed for an annulus of 22-25 mm. The relation among the annulus, plaque in the left coronary leaflet, and the distance to the left coronary ostium is also important.2
Transapical versus transfemoral approach
Perhaps the most exciting aspect of the TAVI procedure is the ability to access the implant site using either a transapical or transfemoral approach. The presence of significant peripheral vascular disease (PVD) is the principal determinant for which approach is used. If PVD is present, femoral access is likely to pose a high risk for complications, especially given the comparatively larger catheter sizes required for these implants. There have also been investigators that have chosen the transapical approach for patients who exhibit large atheroma in the aorta. The transfemoral approach has been the most commonly used approach in the U.S., and was the first cohort to be studied in the PARTNER trial, as enrollment for utilization of the transapical approach did not begin until one year into the study (in 2008).
Since the transfemoral approach is the most widely used vascular access site for cardiac cath procedures, today’s staff should feel confident in their existing skill set for assisting with access. The larger size of the catheters was alluded to earlier, and for the transfemoral approach with the Sapien valve, a 22 French (Fr) or 24 Fr sheath is used. New device developments on the horizon will allow sheath sizes to be reduced by permitting the balloon to be loaded onto the catheter in the descending aorta. More specifically, the newly designed Novaflex (Edwards Lifesciences) delivery system will allow an 18 Fr sheath for the 23 mm valve and 19 Fr for the 26 mm valve.***
The majority of cardiologists with whom Corazon has discussed TAVI technologies have expressed concern with the transapical approach, a technique not commonly used by U.S. interventionalists. In fact, based on Corazon interactions with cath lab staff, further trepidation exists regarding the required thoracic incision(s) associated with transapical access. Moreover, the transapical approach patient requires additional complex care, such as post-procedure chest tube placement and maintenance. Conversely, most of the cardiac surgeons at our client sites express complete confidence in the transapical approach, which usually involves a small thoracotomy incision to access the pericardium followed by a direct “puncture-approach” into the left ventricular apex. There was some debate at the 2010 TCT conference, as Dr. Jeffrey Moses of New York Presbyterian Hospital asked, “Why would we even conceive the transapical approach? Initially, when we were talking about the replacement of aortic valves, we weren’t really conceiving a surgical procedure.”4
A significant number of patients will benefit from the TAVI procedure, even if the less widely adopted transapical approach is used. The transapical approach avoids complex lesions associated with ileofemoral disease that can lead to dissections, occlusions, and perforations, facilitates valve crossing, and enhances the control of placement. For the transapical approach, a 26 Fr delivery system is used.5 The SOURCE registry, a European TAVI registry, indicates that transapical patients do exhibit a slightly higher mortality at 30 days compared to transfemoral patients (10.8% vs. 6.3%), though many experienced TAVI operators have argued that this initial data is not statistically sound enough to determine definitive treatment guidelines.7
The transapical patient population also has more co-morbidities that lead to an expected early mortality compared with the transfemoral population.7 Currently, there is a higher transplantation rate using the transapical approach in Europe when compared with patients enrolled in the U.S. PARTNER trial. This discrepancy is likely due to the fact that the trial mandates that U.S. physicians attempt the transfemoral approach first, with the transapical approach as a second-choice therapy.8
The TAVI procedure
The TAVI procedure requires that the catheter-based skills traditionally considered part of the interventional cardiologist’s toolkit partner with the anatomical interventions employed by  cardiothoracic surgeons to treat structural heart disease. Once again, Corazon believes that successful outcomes in the intra-procedural setting must involve a multi-disciplinary team of experts in cardiovascular disease management. Also, if the procedures are not being performed in a physical environment allowing for simultaneous modalities of monitoring, such as a hybrid suite, gathering the additional resources necessary to complete this procedure can be very daunting for traditional cath lab or operating room staff.
cardiothoracic surgeons to treat structural heart disease. Once again, Corazon believes that successful outcomes in the intra-procedural setting must involve a multi-disciplinary team of experts in cardiovascular disease management. Also, if the procedures are not being performed in a physical environment allowing for simultaneous modalities of monitoring, such as a hybrid suite, gathering the additional resources necessary to complete this procedure can be very daunting for traditional cath lab or operating room staff.
Most U.S. trial sites are reporting the use of general anesthesia during TAVI. This anesthesia is similar to the protocols being used with open-heart surgery patients to promote rapid extubation. The goal is to get the patient extubated as soon as the procedure is complete. Several of the investigational centers have described successful results with patients receiving moderate sedation instead of general anesthesia, especially for those deemed too high risk for general anesthesia induction.
Following are the basic steps for valve delivery using the transfemoral approach:
1) After wire introduction and introduction of a 6 Fr dilator, the artery is preclosed using an internal suture device; 2) A stiff wire is advanced through the diagnostic catheter, 15-18 Fr dilators are carefully advanced, the 22 Fr or 24 Fr delivery sheath is introduced, and then heparin is given.2
The major sequencing steps for the implant portion of the procedure have been described as the following:
1) After placement of the delivery sheath, proceeding to cross the aortic valve; 2) Dilation of the aortic valve; 3) Deployment of the “crimped” valve.
The diseased native valve is first dilated by balloon valvuloplasty under rapid right ventricular pacing, which facilitates subsequent entry of the new valve and allows flow while the new valve position is adjusted for optimal delivery location. The implant valve is crimped on a balloon just before implantation with a specially designed mechanical crimper. The balloon with the crimped valve is advanced with a delivery catheter, which integrates a nose cone at the distal end to facilitate advancement of the delivery system around the aortic arch and eliminates resistance when crossing the native aortic valve. After the bioprosthesis has reached the left ventricle, the delivery catheter is withdrawn into the ascending aorta and the valve is pulled into optimal position, with 50-60% of the assembly on the ventricular side of the aligned sinuses. After valve positioning and prior to deployment, it is important to secure reliable rapid pacing and to wait until the blood pressure falls below 50 mmHg. Pacing continues until the balloon is fully inflated. Prolonged inflation (five seconds after full inflation of the balloon) can be used to obtain maximum expansion of the valve. Primary operator experience has proven essential to more rapid procedure times with continued positive outcomes.
TAVI outcomes
Industry outcome trends reveal that patients with severe aortic stenosis exhibit a poor prognosis with conservative therapies. Unfortunately, there is a large subset of patients with co-morbidities such as a reduced left ventricular ejection fraction (LVEF), which may be a direct result of the aortic stenosis. A careful balancing act must be employed, because this same subset of patients also exhibits a relatively high operative mortality when treated with an open surgical approach. When looking at procedure outcomes, the primary quality indicator that Corazon advocates all programs critically evaluate is the mortality rate. Initial results related to mortality in the TAVI population appear highly encouraging — the 30-day mortality rate for this population has been reported in the 6-10% range.9 This mortality rate is clearly higher than the general open heart surgery (OHS) valve population, though this is currently believed to represent an appropriate outcome, as TAVI patients are typically older and have more chronic conditions compared with their OHS peers. Interestingly, there appears to be similar successful mortality results when examining U.S., European, and Canadian TAVI patient registries (REVIVAL II in the U.S. and Europe, and the Canadian Special Access registry).
There remains a significant difference in procedural success, i.e., proper implantation of the valve (76% vs. 96%) and 30-day mortality (16% vs. 8%) between patients receiving implants at the beginning of the clinical trials and those treated later.2 A learning curve remains one of the most important predictors of procedure success. Early in the development of transfemoral TAVI implant systems, despite limited operator experience and an early version of the valve and delivery system, the 30-day mortality rate was still considered acceptable. As with all disruptive technologies, operator skill or experience, technique, and equipment will continue to improve.
Distinct from mortality, data from the multi-national registries indicates that left ventricular function improves and mitral regurgitation diminishes significantly after valve implantation. The TAVI valve also appears to exhibit superior hemodynamic performance compared with open surgical bioprosthesis in terms of transprothetic gradients, though a higher incidence of aortic regurgitation has been noted. Fortunately, this mild aortic regurgitation seems to be predominantly evaluated as clinically insignificant. In patients with a diminished LVEF, TAVI is linked to better LVEF recovery in patients with severe aortic stenosis compared to open surgical valve replacement, according to a study in Circulation.10 Even more surprising, of those patients with a baseline LVEF 9 Corazon predicts that these functional findings associated with the TAVI procedure will continue to drive the surgical valve treatment “book of business” towards a catheter-based approach, as long as the outcomes continue to remain positive.
On a final note, our team continues to be impressed with the associated complication rates that have been reported with this procedure. Like all catheter-based procedures, the most prevalent complication of both the transfemoral and transapical approach seems to be major vascular access site complications. Invasive procedural staff will need to be prepared to handle the usual complications seen with obtaining transfemoral access (dissections, ischemia, and rupture). Furthermore, clinicians must develop extremely rapid recognition of access complications, particularly due to the larger catheter sizes required for these devices. The transapical approach is a completely different skill set for complication recognition and a major access site complication with this approach is associated with a 50% mortality rate.6
In addition to typical vascular access issues, like its open surgical cousin, the TAVI procedure is also under increased scrutiny for the potential development of thrombolic/embolic complications. There have been several recent analyses that have attempted to determine the impact of microemboli as a result of the implant procedure. In one study, the incidence of clinically silent cerebral embolic lesions on MRI images after TAVI was high, but, fortunately, the incidence of persistent neurologic impairment was low.11 A high level of scrutiny remains necessary, as PARTNER trial data show that TAVI results in a more frequent rate of major stroke (5% vs. 1% in the open surgical cohort). Deploying embolic protection devices during the procedure appears feasible and does not add significantly to procedure time, according to a study published in the November 2010 issue of JACC: Cardiovascular Interventions.12 Nonetheless, these cerebral protection devices remain under investigation, and hopefully will result in further reductions in both silent and clinically significant cerebral ischemia after TAVI. For experienced cath lab clinicians wondering about the incidence of emboli on renal function, a recent study in Canada found the incidence rate of acute renal injury following TAVI for severe aortic stenosis was 11
In conclusion
The paradigm shift for the treatment of ALL cardiovascular conditions has been moving rapidly towards a more a minimally-invasive approach over the last decade. To be better prepared for procedures like TAVI and what are likely to be more advanced structural heart disease therapies in the future, cath lab personnel must broaden their skill set in terms of the full spectrum of heart disease and advanced technologies. The success of the current technologies employed in the TAVI procedure, as well as the acceptable outcomes, should drive cath lab personnel to become familiar with these therapies. If TAVI continues to demonstrate improved quality of life and longevity compared to standard medical therapy or the more invasive, open surgical approach, then even the smallest of cath labs will need to be prepared for this disruptive technology to one day invade their space!
Ross is a Vice President at Corazon, offering consulting, recruitment, and interim management for the heart, vascular, and neuro specialties. To learn more, visit www.corazoninc.com or call (412) 364-8200. To reach Ross, email rswanson@corazoninc.com. Disclosure: Ross Swanson reports no conflicts of interest regarding the content herein.References
1. The PARTNER Trial: Placement of Aortic Transcatheter trial. Available at https://www.clinicaltrials.gov/ct2/NCT00530894. Accessed November 28, 2010. 2. Ben-Dor I, Waksman R, Satler LF, Pichard AD. Edwards Sapien aortic valve: transfemoral approach. Vascular Disease Management 2010; 7(1). Available online at https://www.vasculardiseasemanagement.com/content/edwards-sapien-aortic-valve-transfemoral-approach. Accessed December 15, 2010. 3. Clinical trial establishes catheter-based aortic valve replacement as new standard of care for patients who cannot undergo surgery. Cardiovascular Research Foundation, News & Events. September 22, 2010. Available online at https://www.crf.org/aboutus/news-and-events/215-clinical-trial-establishes-catheter-based-aortic-valve-replacement-as-new-standard-of-care-for-patients-who-cannot-undergo-surgery.html. Accessed December 17, 2010. 4. Wood S. Changing PARTNER: Program tweaks overshadow updates from transcatheter-valve studies. September 23, 2009. HeartWire: TheHeart.org. Available online at www.theheart.org/article/1006131.do. Accessed November 28, 2010. 5. Dmyterko K. TCT: Transfemoral approach should trump transapical techniques for TAVI. Cardiovascular Business. Available online at https://www.cardiovascularbusiness.com/index.php?option=com_conferences&article=24431&conference=21&event=6&topic=437. Accessed December 15, 2010. 6. Thomas, M. TAVI with the Edwards Sapien Valve: An update on the latest trial data and the future of aortic valve technology. Cardiac Interventions Today 2010 July/August. Available online at https://bmctoday.net/citoday/2010/08/article.asp?f=taviwith-the-edwards-sapien-valve. Accessed December 15, 2010. 7. Thomas M, Schymik G, Walther T, et al. Thirty-day results of the Sapien aortic bioprosthesis European Outcome (SOURCE) registry. Circulation 2010;122:62-69. 8. Transfemoral or transapical aortic valve implantation? Cardiovascular News International. September 13, 2010. Available online at https://www.cxvascular.com/cn-latest-news/cardiovascular-news---latest-news/transfemoral-or-transapical-aortic-valve-implantation. Accessed December 15, 2010. 9. Webb JG, Altwegg L, Boone RH, et al. Transcatheter aortic valve implantation: Impact on clinical and valve-related outcomes. Circulation 2009;119:3009-3016. 10. Circ: TAVI trumps SAVR in stenotic patients with decreased LVEF. Cardiovascular Business. Available online at https://www.cardiovascularbusiness.com/index.php?option=com_articles&article=24933&publication=26&view=portals. Accessed December 15, 2010. 11. MRI shows TAVI produces many silent cerebral embolic lesions. Target Health Global. Available online at https://blog.targethealth.com/?p=11319. Accessed December 15, 2010. 12. Nietlispach, F, Wijesinghe N, Gurvitch, R, et al. An embolic protection device for aortic valve interventions. J Am Coll Cardiol Intv 2010; 3: 1133-1138.Corrections: *This sentence originally incorrectly stated that the Sapien was commercially available in the U.S. It is not commercially available at this time. **This sentence originally stated that the FDA granted conditional approval for the Medtronic device. We clarified that the FDA has granted conditional approval for a trial of the Medtronic device. ***Novaflex was spelled incorrectly in the original version.