


When Do You Decide Not to Take a STEMI Patient to the Cath Lab? Addressing an Ethical Dilemma
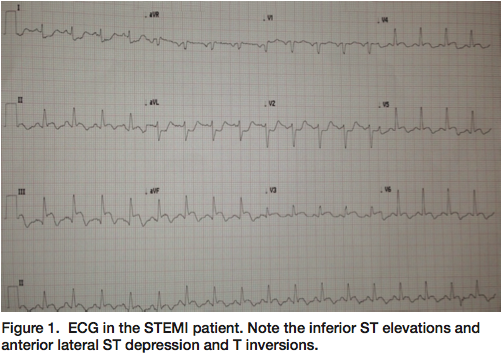 The ST-elevation myocardial infarction (STEMI) team was called in to the hospital for activation at 11:30pm on a Thursday night. I always try to get the electrocardiogram (ECG) sent to my smartphone while getting dressed and before driving in. The ECG showed acute inferior STEMI with anterior T-wave inversions (Figure 1). The ECG was not classic, but certainly was an inferior STEMI, obtained with the patient having “chest pain”. The cath lab team and I were en route to the emergency room (ER) when my fellow, Dr. Megha Agarwal, called me and said there might be some issues with consent. In the ER, I met the patient, a 60-year-old woman with a terminal illness, two weeks of atypical chest pain and shortness of breath. The chest pain was now associated with more severe shortness of breath which had been increasing over the last one week.
The ST-elevation myocardial infarction (STEMI) team was called in to the hospital for activation at 11:30pm on a Thursday night. I always try to get the electrocardiogram (ECG) sent to my smartphone while getting dressed and before driving in. The ECG showed acute inferior STEMI with anterior T-wave inversions (Figure 1). The ECG was not classic, but certainly was an inferior STEMI, obtained with the patient having “chest pain”. The cath lab team and I were en route to the emergency room (ER) when my fellow, Dr. Megha Agarwal, called me and said there might be some issues with consent. In the ER, I met the patient, a 60-year-old woman with a terminal illness, two weeks of atypical chest pain and shortness of breath. The chest pain was now associated with more severe shortness of breath which had been increasing over the last one week.
The patient was also affected by a terminal neurodegenerative illness with likelihood of one-year survival at less than 50%. She understood the state of her illness and prognosis. She was bedridden and had in attendance her two caregivers, one of which had her health care power of attorney. Despite her underlying disease and STEMI, the patient was alert, conversant, intelligent and coherent. She was a heavy smoker for many years, continuing to the onset of her recent symptoms, but otherwise had no coronary artery disease risk factors. To further complicate matters, the chest x-ray showed a large, right lung pneumonic consolidation and infiltrate. Her white blood cell count was 24,000 with normal hemoglobin, platelets, and renal function. Troponins were elevated at 10 ng/mL.
She was examined in bed, but at home was confined to a wheelchair and did not ambulate. Her blood pressure was 88/50, with a heart rate of 110 beats per minute and respirations at 22/minute. She had decreased breath sounds over the right lung with some rales in the left lung, a II/VI systolic murmur at apex, and diminished pulses in all extremities. She was afebrile. We concluded her pneumonia probably started 10 days earlier, but was now markedly worsened and associated with an inferior STEMI.
What to do? To cath or not to cath?
The patient had no family, but her full-time caregivers were present. She had lived with her disease for many years, and did not want any maneuvers that would prolong her life, given the terrible prognosis of her underlying illness. She specifically had declined resuscitation measures should anything happen to her. With her acute STEMI (which may actually have been a couple of days old), and her pneumonia, do you proceed to the cath lab or tell her that medical therapy would be a good alternative to revascularization? This was one of the most difficult decisions that I have had to make in many years. As the physician that would perform the angiogram and possible percutaneous coronary intervention, what was my obligation to proceed in the care of this particular patient? The rest of the story continues in a moment.
When should you not take a STEMI patient to the cath lab?
There are some clear situations where you should not take the STEMI patient directly to the cath lab. These “no-go” conditions, a.k.a relative contraindications (Table 1), can make the decision to defer cath fairly straightforward. Some of these include recent or active bleeding, fulminant infection, inability to understand procedure and give informed consent, severe anemia, hyperkalemia, severe hemodynamic or electrocardiographic instability, aortic dissection, central nervous system impairment or trauma. Of course, if the informed and competent patient declines the procedure, that’s the end of the discussion. (I always remind our fellows that we work for the patient; he/she is our “boss” in the clinical setting.)
Table 1. Contraindications to Cardiac Catheterization
- Absolute contraindications
Inadequate equipment or catheterization facility
- Relative contraindications
Acute gastrointestinal bleeding or anemia
Anticoagulation (or known, uncontrolled bleeding diathesis)
Electrolyte imbalance
Infection and fever
Medication intoxication (e.g., digitalis, phenothiazine)
Pregnancy
Recent cerebrovascular accident (<1 month)
Renal failure
Uncontrolled congestive heart failure, high blood pressure, arrhythmias
Uncooperative patientSource: Kern MJ. The Cardiac Catheterization Handbook. 5th edition. Elsevier Saunders: Philadelphia, Pennsylvania; 2011: 4.
Under all other circumstances and if the criteria for STEMI are met, we take the patient to the cath lab and proceed with PCI if the angiographic appearance of the infarct-related vessel makes PCI feasible. Under rare circumstances, we may not be able to perform PCI or we may need to refer the patient to the cardiothoracic surgeon. In patients in cardiogenic shock with STEMI, we may also proceed to do PCI of the non-infarct-related vessels.
What to do about informed consent?
No procedure can proceed without the patient’s consent unless there is overwhelming evidence that failure to treat would result in severe harm or death. In the circumstance where the patient cannot give consent and there is no one known that has the legal authority to speak for the patient (family, surrogate or designated individual with credentials), emergency lifesaving procedure consent can be obtained and signed by two physicians familiar with the critical issue and who both agree that the procedure is needed.
What would you tell a STEMI PCI patient with terminal illness and limited long-term prognosis about what is the best approach, especially if she is unsure of her own mind? What do we do with the patient who presents with a STEMI, but who has metastatic cancer, end-stage neurodegenerative disease, end-stage Alzheimer’s disease, or any of a number of pre-terminal co-morbid conditions which have a very limited life expectancy? What should we tell the patient and their family?
There are no pat answers. Each discussion with the patient and their family must be individualized. I can only tell you what I do and what I tell my fellows in these circumstances. First, after reviewing all the information, especially old ECGs and records, if available, I speak with the patient. I ask for the patient’s family to be present to share in the discussion, but I address the patient directly. I explain to the patient what I know is happening now, and what I understand has happened to him/her in the past that complicates the STEMI treatment. Then I ask the patient what they understand to be happening and what they think might be best for them. Then I listen and wait, actively listening without being distracted or having someone distract the patient.
What will STEMI PCI accomplish?
At this point, we should ask ourselves, what will the PCI in this setting for this patient accomplish? We may not know exactly what benefit might accrue, but we certainly know what the potential for harm may be. At this point in the process, the patient often asks a couple questions. Will this hurt? Will I live longer? Will I die sooner if I don’t have the procedure? Will I need a breathing tube or life support? Will I be a “vegetable” if something happens? What would you do if you were me?
These are the hardest questions with the least certain answers. If I can answer any of the questions with certainty, then of course I do. If I can’t, then I tell the patient that I do not know the answers and can only provide my best educated guess. The ultimate decision is always the patient’s. While the family has great influence at this point in a person’s life, I still want to hear directly from the patient whether they would like to proceed or not. If I cannot get a commitment from the patient that they want the procedure, then we defer, readdressing the issues and timing of cath later as clinically indicated.
What did we do?
 We spent about an hour talking to the patient about her options and wishes. She vacillated between wanting to do nothing and do everything. She was terribly conflicted, as was I. I understood that we might have little to offer, but that she might benefit by knowing whether opening the right coronary artery would add some quality time to her life. I suggested that we could do the angiogram and see if there was something that might help and only do revascularization if it could be done safely with low risk, so that we would not be put in the difficult situation of unwanted intubation and resuscitation during the PCI.
We spent about an hour talking to the patient about her options and wishes. She vacillated between wanting to do nothing and do everything. She was terribly conflicted, as was I. I understood that we might have little to offer, but that she might benefit by knowing whether opening the right coronary artery would add some quality time to her life. I suggested that we could do the angiogram and see if there was something that might help and only do revascularization if it could be done safely with low risk, so that we would not be put in the difficult situation of unwanted intubation and resuscitation during the PCI.
 She and her caregivers understood what I had explained and agreed to proceed. I knew that this was a difficult decision for her and prayed that I could get the procedure done safely and get her out of the lab alive. Consent for cath was signed. A “Do Not Resuscitate” (DNR) order was temporarily rescinded at the patient’s request (to be restarted after leaving the cath lab), and we went to the lab.
She and her caregivers understood what I had explained and agreed to proceed. I knew that this was a difficult decision for her and prayed that I could get the procedure done safely and get her out of the lab alive. Consent for cath was signed. A “Do Not Resuscitate” (DNR) order was temporarily rescinded at the patient’s request (to be restarted after leaving the cath lab), and we went to the lab.
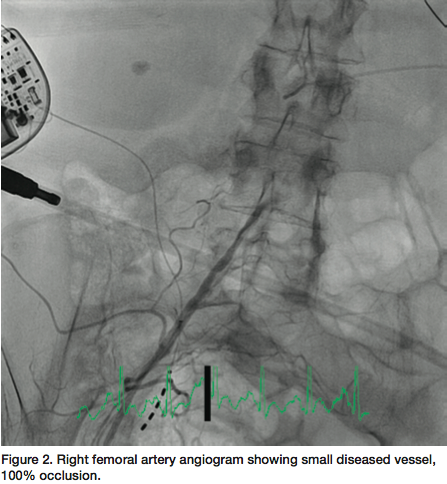
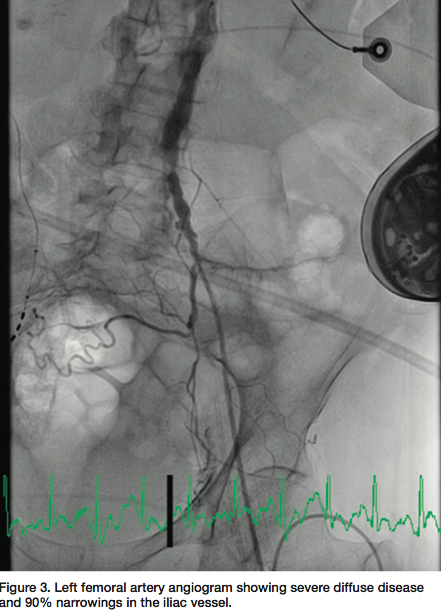
 Little did I anticipate that this patient would have the worst peripheral vascular and coronary artery disease I had seen in ten years. The procedure began from the femoral approach since she had bilateral wrist contractures and no pulses. Ultrasound-guided femoral artery access was used since there were no palpable femoral pulses. After an hour of attempts for access, we found that the right iliac artery was 100% occluded and the left femoral and iliac arteries were diffusely diseased, with serial 90% lesions to the aortic junction (Figures 2-3). We were able to pass 5 French catheters to the coronary ostia and found that both the left and right
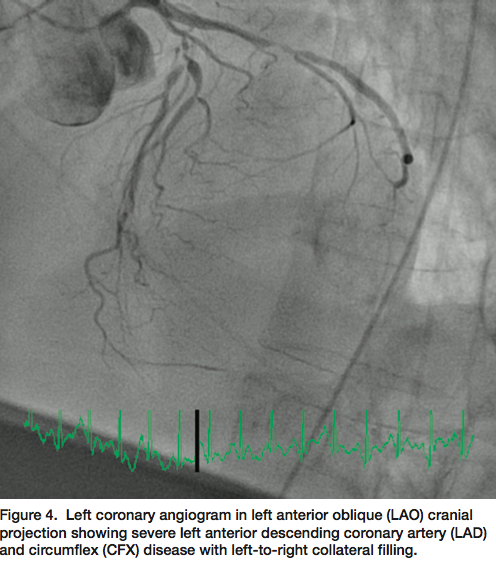
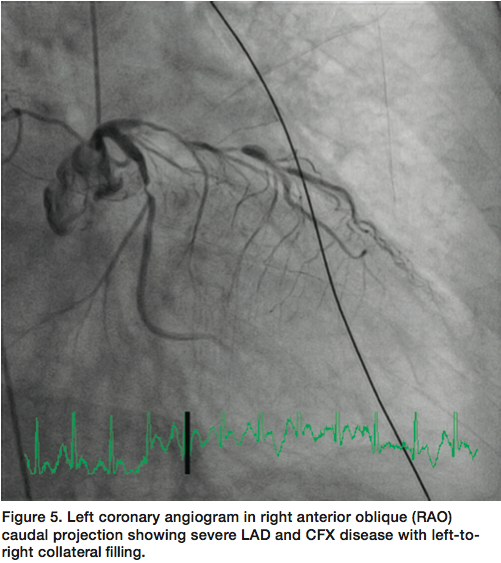
Little did I anticipate that this patient would have the worst peripheral vascular and coronary artery disease I had seen in ten years. The procedure began from the femoral approach since she had bilateral wrist contractures and no pulses. Ultrasound-guided femoral artery access was used since there were no palpable femoral pulses. After an hour of attempts for access, we found that the right iliac artery was 100% occluded and the left femoral and iliac arteries were diffusely diseased, with serial 90% lesions to the aortic junction (Figures 2-3). We were able to pass 5 French catheters to the coronary ostia and found that both the left and right  coronary arteries were severely and diffusely diseased, with multiple and serial critical lesions throughout (Figures 4-6). The left ventricular end diastolic pressure was 35 mm Hg and ventriculography was deferred. Based on the terrible state of all coronary arteries, the severely impaired left ventricle, and her underlying condition, I felt that PCI was futile. We concluded our procedure at 3am and transferred the patient to the recovery room. She felt she did not want to continue using the supplemental oxygen mask that was needed to maintain her oxygen saturations. She requested we remove the mask and two hours later she succumbed.
coronary arteries were severely and diffusely diseased, with multiple and serial critical lesions throughout (Figures 4-6). The left ventricular end diastolic pressure was 35 mm Hg and ventriculography was deferred. Based on the terrible state of all coronary arteries, the severely impaired left ventricle, and her underlying condition, I felt that PCI was futile. We concluded our procedure at 3am and transferred the patient to the recovery room. She felt she did not want to continue using the supplemental oxygen mask that was needed to maintain her oxygen saturations. She requested we remove the mask and two hours later she succumbed.
What did we learn?
 My team and I learned a great deal from this patient in working through her STEMI treatment. We learned that knowing the patient, especially knowing their state of mind regarding their wishes for their future, is always key to making good decisions. We learned that taking the time to talk with the patient and family when there is uncertainty on how and when to proceed is critical to everyone’s understanding of the potential risks and benefits of the procedure. We learned that sometimes you cannot do anything but try. We tried to provide the best information that permitted the best decision. We do this even though it may not be the outcome you would like. We learned that such decisions are easy when the patient says “no”. But it’s hard for the physician and his team to say “no”, especially when we have been trained and equipped to urgently revascularize patients presenting with myocardial infarction. As my younger colleague Dr. Arnold Seto reminded me, “Only with thoughtfulness and wisdom can we resist the pressures to act rapidly.” We must recognize that when there is nothing more we can do for the patient, we must make them comfortable and keep them company until the end.
My team and I learned a great deal from this patient in working through her STEMI treatment. We learned that knowing the patient, especially knowing their state of mind regarding their wishes for their future, is always key to making good decisions. We learned that taking the time to talk with the patient and family when there is uncertainty on how and when to proceed is critical to everyone’s understanding of the potential risks and benefits of the procedure. We learned that sometimes you cannot do anything but try. We tried to provide the best information that permitted the best decision. We do this even though it may not be the outcome you would like. We learned that such decisions are easy when the patient says “no”. But it’s hard for the physician and his team to say “no”, especially when we have been trained and equipped to urgently revascularize patients presenting with myocardial infarction. As my younger colleague Dr. Arnold Seto reminded me, “Only with thoughtfulness and wisdom can we resist the pressures to act rapidly.” We must recognize that when there is nothing more we can do for the patient, we must make them comfortable and keep them company until the end.
I hope this vignette stimulates you to think about how to approach some of our critically ill patients with serious co-morbidities coming into the cath lab.
I thank Drs. Agarwal and Seto for their insights into our story.



