


Making Complex Simple
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Ori Waksman, MD1; Hayder Hashim, MD, FSCAI2
1Fellow, Cardiovascular Disease MedStar/Georgetown University; 2Assistant Professor, Division of Cardiology, Georgetown University; Interventional Cardiologist – Medstar Washington Hospital Center, Washington, D.C.
Revascularization of patients with unprotected left main disease poses a significant challenge due to the heightened risk of mortality and periprocedural hemodynamic collapse. Historically, such patients were managed surgically via coronary artery bypass grafting (CABG); however, randomized controlled trials (RCTs) demonstrating similar mortality and long-term outcomes with percutaneous coronary intervention (PCI) have shifted contemporary practice trends and broadened the use of unprotected left main percutaneous coronary intervention (ULM-PCI).
As the role of PCI expands, in order to address the challenges posed by difficult anatomy and complex lesion subtypes, interventional cardiologists and cardiac catheterization lab staff should be made aware of the array of available and innovative devices at their disposal.
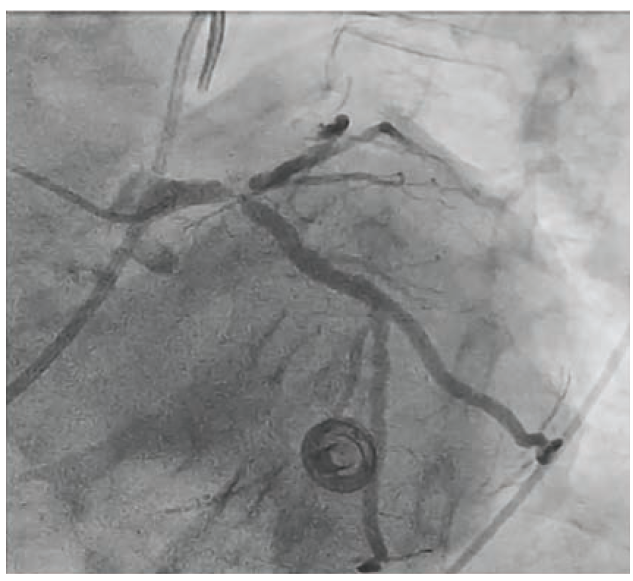
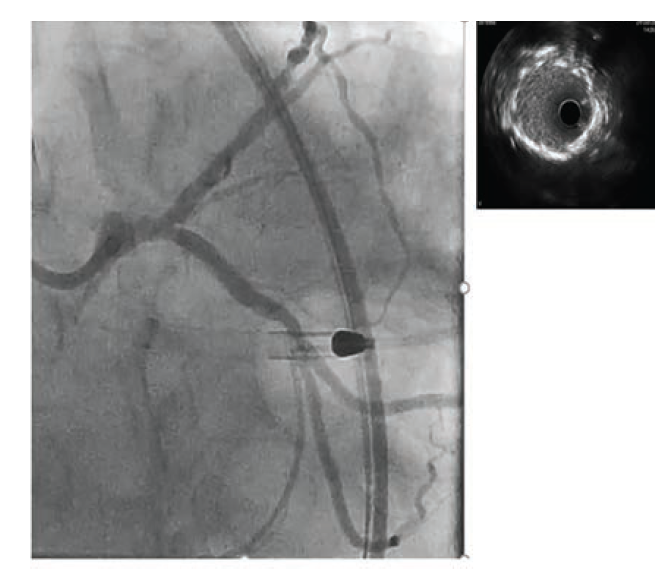
To illustrate this point, we present the case of an 86-year-old male with diabetes mellitus, paroxysmal atrial fibrillation (anticoagulated with apixaban), hypercholesterolemia, and left bundle branch block who presented to the emergency department with acute onset chest pain, shortness of breath and hypotension with a blood pressure of 88/62 mmHg. The patient was diagnosed with non-ST-elevation myocardial infarction (NSTEMI) and was emergently transferred to the cardiac catheterization lab, where the patient underwent left and right heart catheterization. Right heart catheterization demonstrated low cardiac output with elevated filling pressures. Coronary angiography revealed a codominant system, calcified Medina 1,1,1 critical left main disease, and ostial right coronary artery (RCA) disease (Figure 1).
Given these findings and systemic hypotension, an intra-aortic balloon pump (IABP) was placed and the patient was transferred to our hospital for coronary artery bypass grafting (CABG) evaluation. Due to advanced age, high frailty index, and patient preference, he was not considered to be a good surgical candidate and within 24 hours, he was brought back to the cardiac catheterization lab for intervention.
Planning
We opted to upgrade the IABP for an Impella CP (Abiomed) in order to provide greater hemodynamic support for this ULM-PCI. Distal left main Medina (1,1,1) bifurcation classification was to be reassessed using intravascular imaging.
Access
Due to the challenging anatomical and atherosclerotic peripheral vasculature, a single-access technique was preferred. A Perclose ProStyle closure device (Abbott Vascular) was deployed in a pre-close fashion, then the 8 French (F) IABP sheath was upgraded to a 14F short Impella CP sheath. Using a micro-puncture access kit, the hemostasis diaphragm of the 14F sheath was then accessed and a 7F 45cm PINNACLE® DESTINATION® Guiding Sheath (Terumo Interventional Systems) was inserted.
Intervention
A Launcher 7F Extra Backup (EBU) 3.5 (Medtronic) catheter was used to engage the left main coronary artery. Once the left main was successfully engaged, both limbs of the bifurcation, the left anterior descending (LAD) and left circumflex (LCx) arteries, were wired with the blue and white RUNTHROUGH® NS Izanai Coronary Guidewires (Terumo Interventional Systems). The different colors of the same quality RUNTHROUGH® NS Izanai wires (ie, a white wire was used for the LAD and a blue wire was used for LCx) are essential in bifurcation cases to help differentiate branches and minimize procedural confusion.
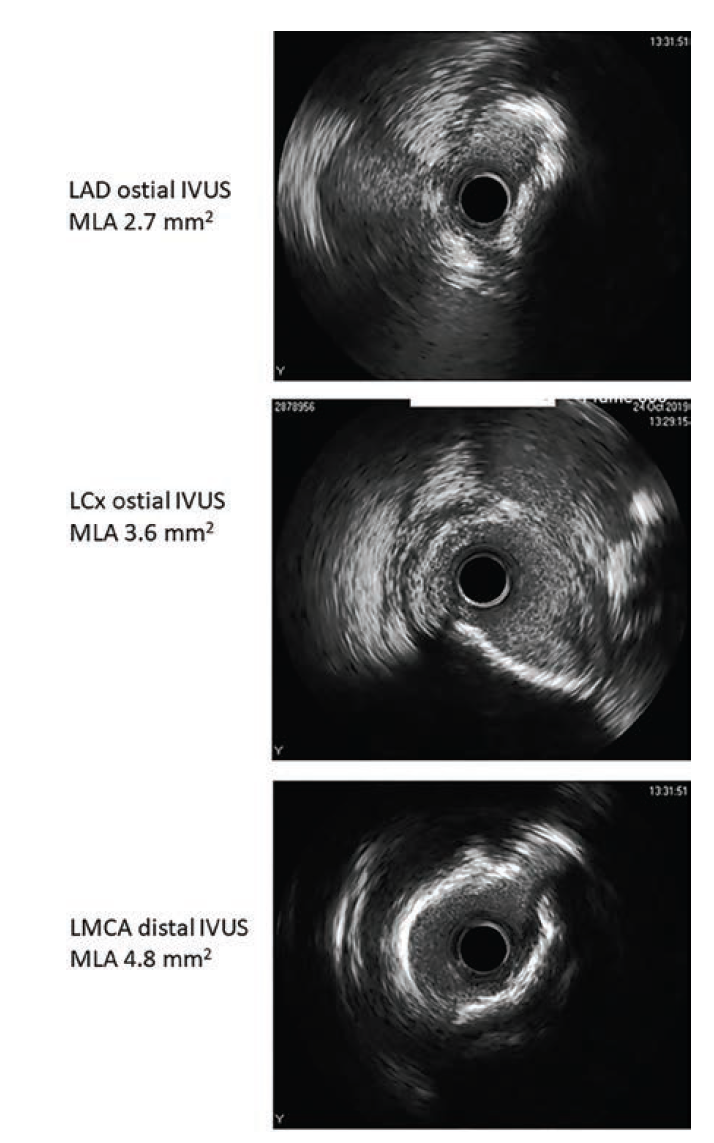
Given angiographic severe calcifications and the potential need for atherectomy, we opted to use Opticross HD intravascular ultrasound (IVUS) (Boston Scientific) for a better qualitative assessment of the lesion.
In order to facilitate delivery of the IVUS catheter, a 1.5 mm RX Takeru™ PTCA Balloon Dilatation Catheter (Terumo Interventional Systems) was used to predilate the ostium of the LCx and LAD, respectively. IVUS demonstrated dense calcification at the ostial LCx and LAD. However, the LCx calcium was found to be fractured and extended to less than <180 degrees, while the LAD calcification was severe and concentric at ~320 degrees (Figure 2).
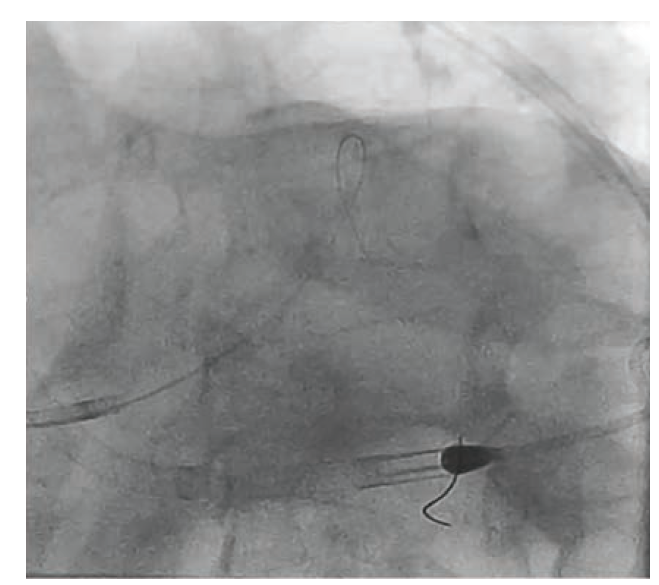
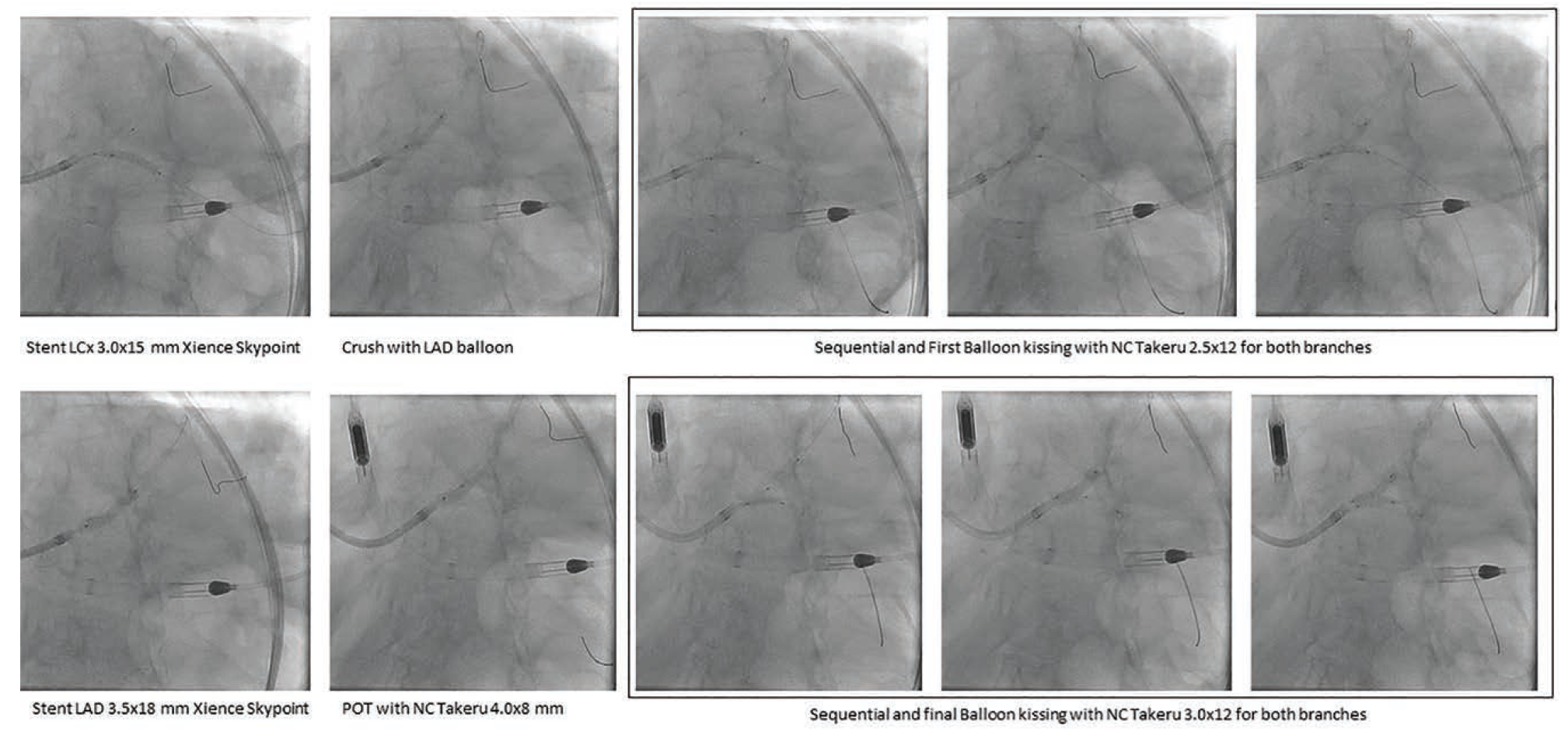
Based on the above assessment with IVUS, we elected to proceed with orbital atherectomy (Diamondback 360 orbital atherectomy system, Abbott Vascular) of the LAD, before which the LCX wire was removed and the LAD wire was swapped for a ViperWire with Flex Tip (Abbott Vascular) using a 1.7F distal tip FINECROSS® M3 Coronary Micro-Guide Catheter (Terumo Interventional Systems). Orbital atherectomy was performed with 4 passes at 80,000 RPM. The LAD (Figure 3) was treated with a 3.0 mm x 15 mm Takeru NC balloon. The LCX was rewired with the same Runthrough wire and a double kiss (DK) crush technique was used to stent the LM distal bifurcation with two Xience Skypoint drug-eluting stents (Abbott Vascular) (Figure 4 highlights the sizes and steps of the DK crush technique). IVUS assessment demonstrated well-opposed and well-expanded stents from the LAD and LCx into the distal LM (Figure 5).
At the conclusion of the procedure, the Impella CP was removed and the 14F sheath was removed over the wire. The pre-deployed ProStyle closure device was fully deployed and enforced with an 8F ANGIO-SEAL® Vascular Closure Device (Terumo Interventional Systems) with instantaneously effective hemostasis.*
*Angio-Seal Vascular Closure Device is not indicated for use in hybrid vascular closures as used in this article. Refer to the product labels and packaging insert for complete warnings, precautions, complications, and instructions for use.
Take-Home Points
It is imperative to have full knowledge and understanding of available equipment and technology in the catheterization lab to ensure smooth sailing and successful interventions in complex clinical scenarios. While the use of intravascular ultrasound confirmed Medina (1,1,1) angiographic classification, it was essential to select the right option for plaque modification and sizing of the vessels. IVUS also highlighted the importance of post intervention assessment of deployed stents, especially in critically important anatomical locations.
This case is sponsored by Terumo Interventional Systems.
Find More:
Grand Rounds With Morton Kern, MD
Peripheral Artery Disease Topic Center
The Latest Clinical & Industry News
Podcasts: Cath Lab Conversations
Cardiovascular Ambulatory Surgery Centers (ASCs) Topic Center


