


Pushing Boundaries: Transradial Access for Complex PCI
Background
TAKERU PTCA Balloon Dilatation Catheters have been recently launched by Terumo. In this report, we summarize our initial experience with the TAKERU balloon catheter. Since July 1, 2019, we have used these balloon catheters routinely in our complex percutaneous coronary interventions (PCIs).
The 1.5 mm balloon catheter has a single midpoint Platinum-Iridium radiopaque marker (larger diameter balloon catheters have two markers) and is equipped with a 108 cm stainless steel proximal shaft and 21 cm stainless steel core middle shaft. The unique feature of this balloon catheter is the 23 cm hydrophilic coating that allows excellent tracking ability. The TAKERU 1.5 balloon catheter’s entry profile is 0.43 mm, relatively larger compared to the Sprinter Legend (1.25 mm) (Medtronic). However, the TAKERU balloon catheter has greater pushability based on bench testing results.
Clinical Case
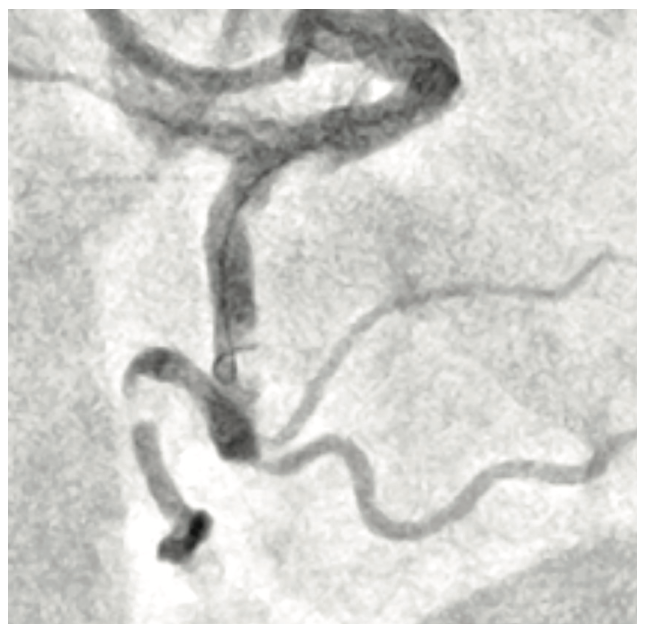
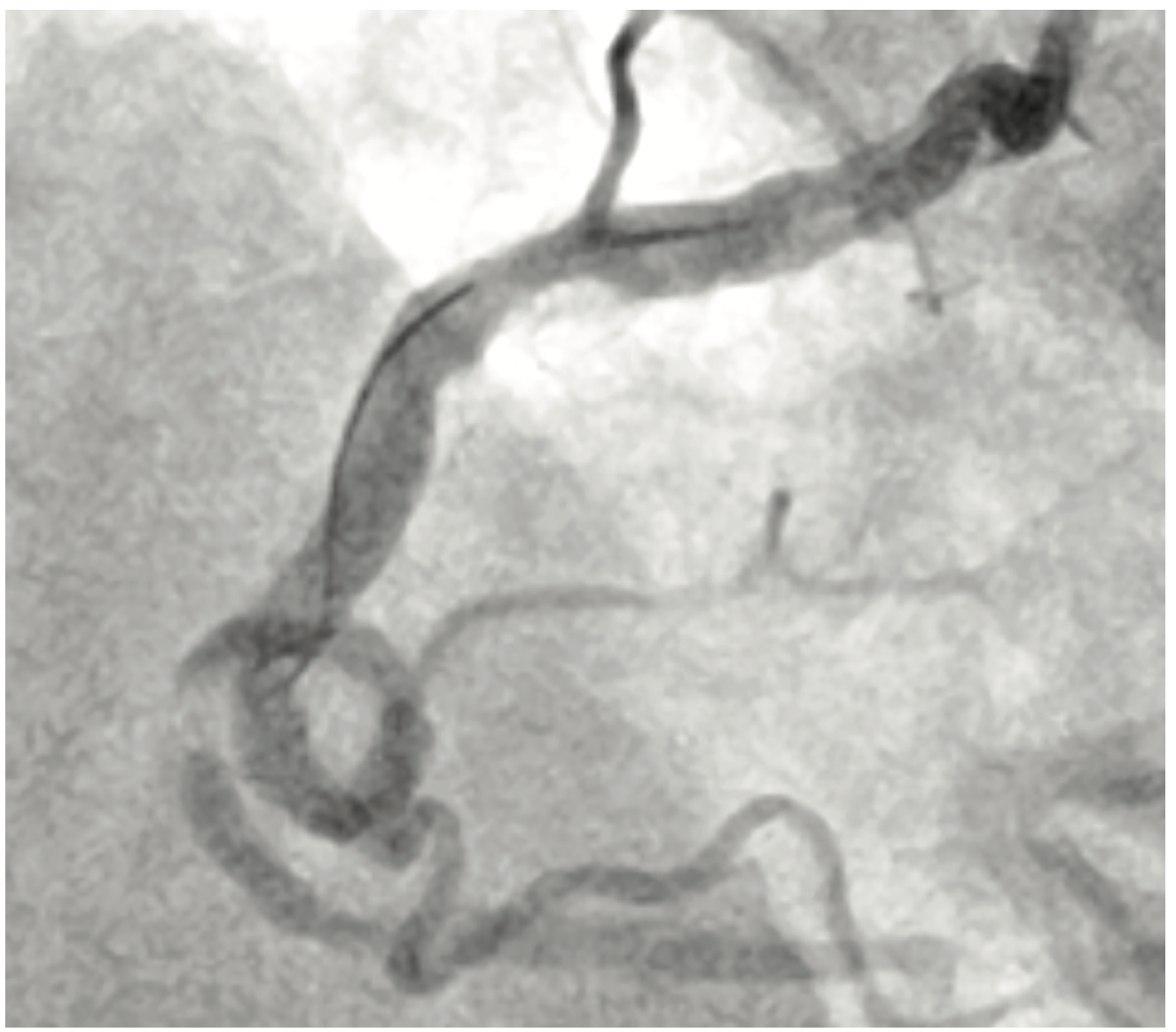
A 70-year-old gentleman presented with Canadian Cardiovascular Society (CCS) class III angina despite two anti-anginals (Metoprolol XL 25 mg daily and ranolazine 500 mg BID). His myocardial perfusion imaging demonstrated medium-sized inferior wall reversible defect with normal left ventricular function. His other comorbidities included chronic atrial fibrillation (on apixaban 5 mg BID), hypertension, and hyperlipidemia (on rosuvastatin 40 mg daily). His angiography revealed severe stenosis of the mid right coronary artery (RCA) involving a 360-degree loop. Further analysis of the angiogram revealed multiple contiguous lesions in the RCA with severe calcific lesions proximal and distal to the loop (Figures 1 and 2). Given severe tortuosity, rotational atherectomy would be challenging and we were hoping to achieve a good result using a balloon catheter strategy.
Procedure
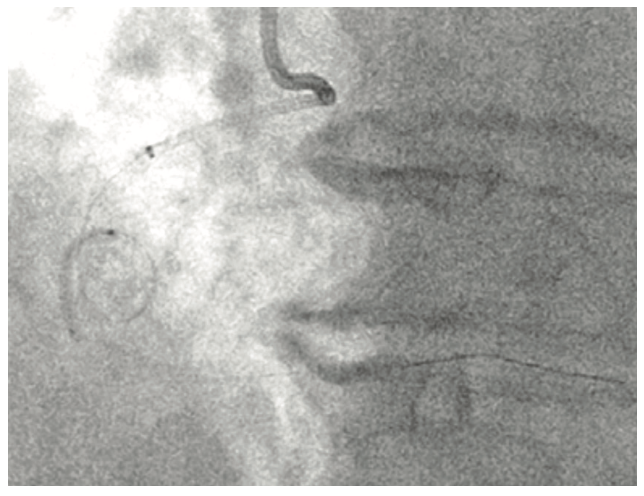
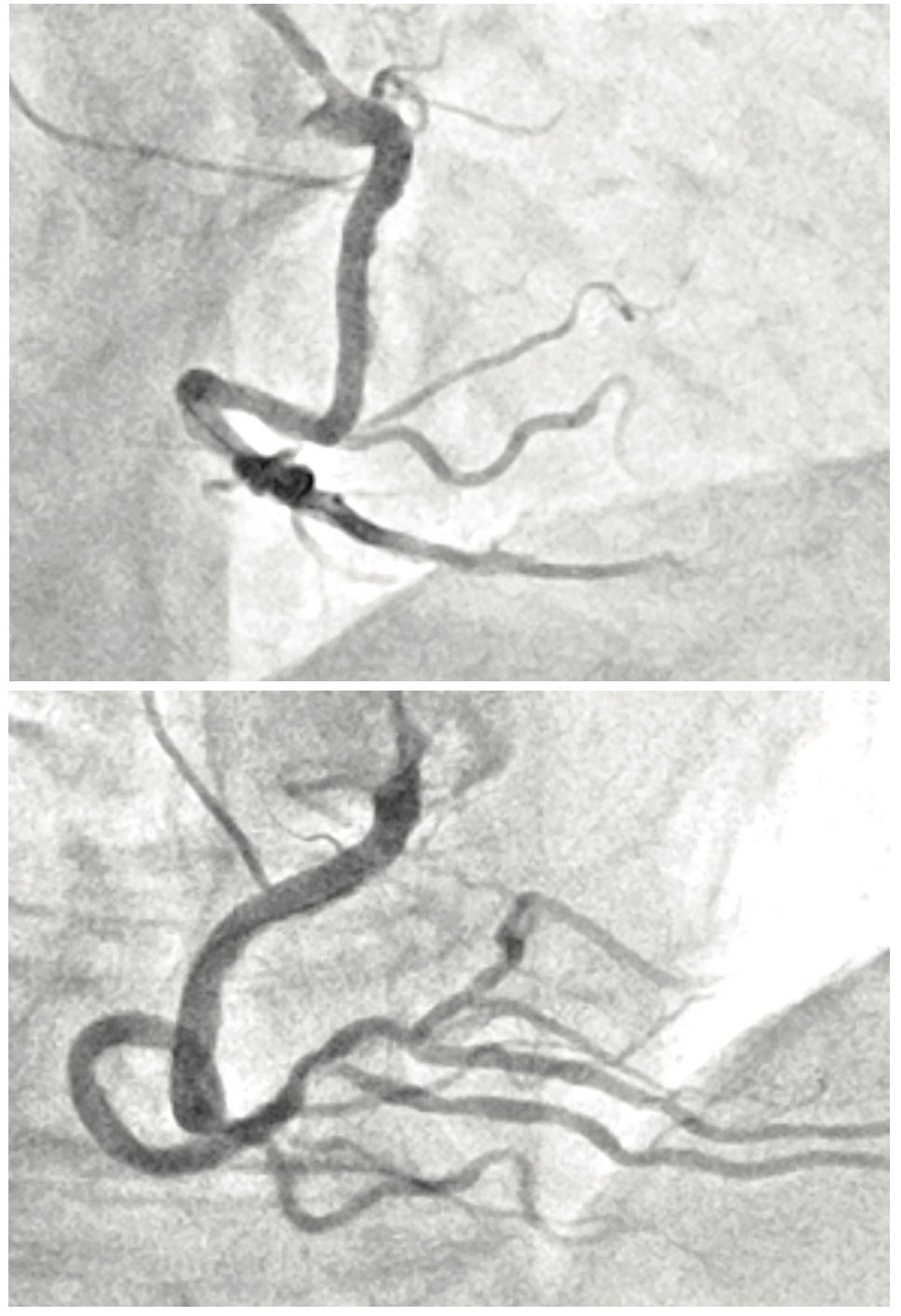
The RCA was engaged with the AL1 7 French (Fr) guide catheter via the right radial approach. After administering heparin to a goal ACT of >250s, we advanced a floppy coronary wire to the distal PDA using a microcatheter and subsequently exchanged it for a supportive guidewire. The loop did not unravel after placing the support wire and hence we introduced a 7 Fr guide catheter extension. We serially pre-dilated the lesions initially with a 1.5 mm x 15 mm, 2.0 mm x 20 mm TAKERU balloon catheter at 14 atm (Figure 3). We advanced the guide catheter extension further to the mid RCA using balloon catheter-assisted tracking and delivered several overlapping drug-eluting stents which were aggressively post-dilated with noncompliant balloons. Final angiography (Figure 4) showed no evidence of dissection or perforation. There was TIMI-3 flow and 0% residual stenosis. The patient was placed on triple therapy (aspirin 81 mg daily/clopidogrel 75 mg daily/apixaban 5 mg BID) for one month along with a proton pump inhibitor later dual therapy for 12 months.
Products Used
• Cordis 7 Fr AL1 Guide Catheter via right radial approach
• Asahi Grand Slam guidewire
• Medtronic Telescope guide extension
• Asahi Caravel microcatheter
• 1.5 mm x 15 mm RX TAKERU balloon catheter
• 2.0 mm x 20 mm RX TAKERU balloon catheter
Conclusion
TAKERU balloon catheters offer excellent pushability and tracking ability courtesy of the hydrophilic coating and low profile. This case demonstrates the aforementioned qualities in complex, calcific coronary anatomy.
This article is supported by Terumo Medical Corporation.
Disclosure: Dr. Khatri reports he is a consultant to Terumo Medical Corporation. PM-05636


