


“Winter is Coming… But Gets Well(ens)”: Two Rare Patterns of LAD Occlusion in the Same Patient, Suggesting Spontaneous Reperfusion
Abstract
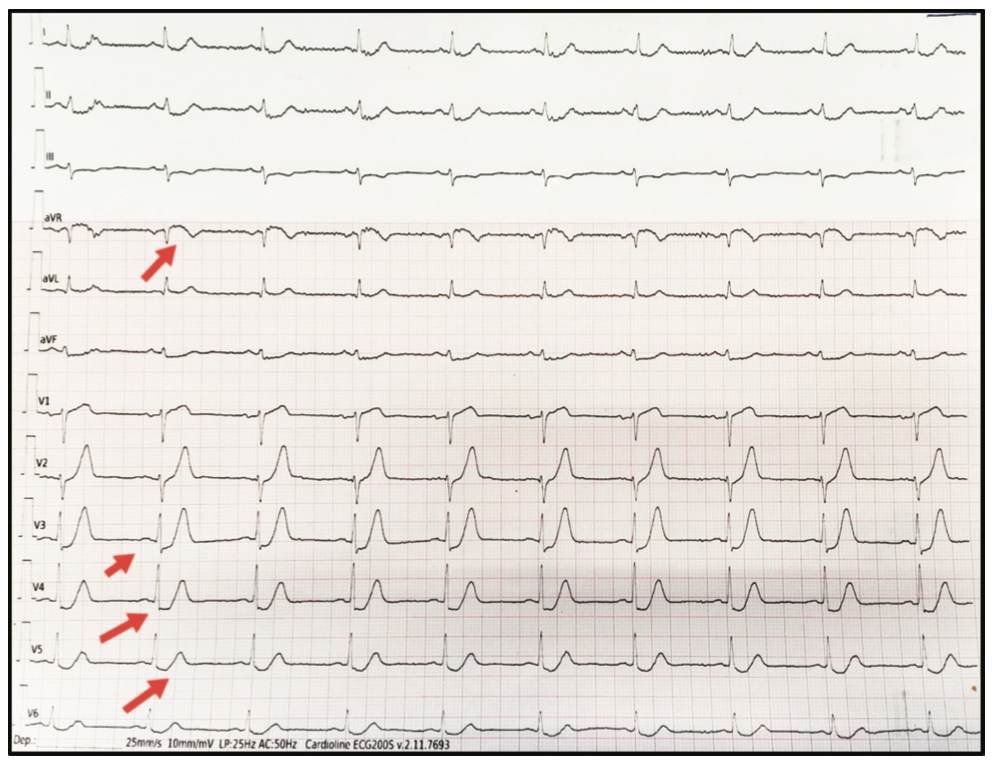
The de Winter and Wellens’ syndrome patterns are associated with acute left anterior descending coronary artery occlusion; however, it is very rare to find both patterns in the same patient. In this case, a decrease in the J point in the precordial leads is evident in the patient’s initial electrocardiogram, followed by an ascending ST segment with a symmetrical positive T wave and ST elevation in aVR, identified as a de Winter pattern. This is followed by the classic Wellens’ syndrome type B pattern in the second electrocardiogram, suggesting an anterior ST-segment elevation myocardial infarction with subsequent spontaneous reperfusion. It is an extremely rare event and we are unaware of any published reports describing both patterns coexisting in the same patient.
The electrocardiogram (ECG) is a diagnostic tool of high value in the approach to chest pain of cardiac origin. The full spectrum of electrocardiography abnormalities indicating acute coronary ischemia or occlusion requiring immediate cardiac catheterization goes beyond the well-known ST- segment elevation pattern. Several ECG patterns have been reported in association with acute myocardial ischemia due to critical stenosis or occlusion of a coronary artery. These patterns include de Winter, Wellens’ syndrome (types A and B), new left bundle branch block, preexisting left bundle branch block with Sgarbossa criteria, and hyperacute T waves, and their presence should be considered indicative of a ST-elevation myocardial infarction (STEMI).1-4
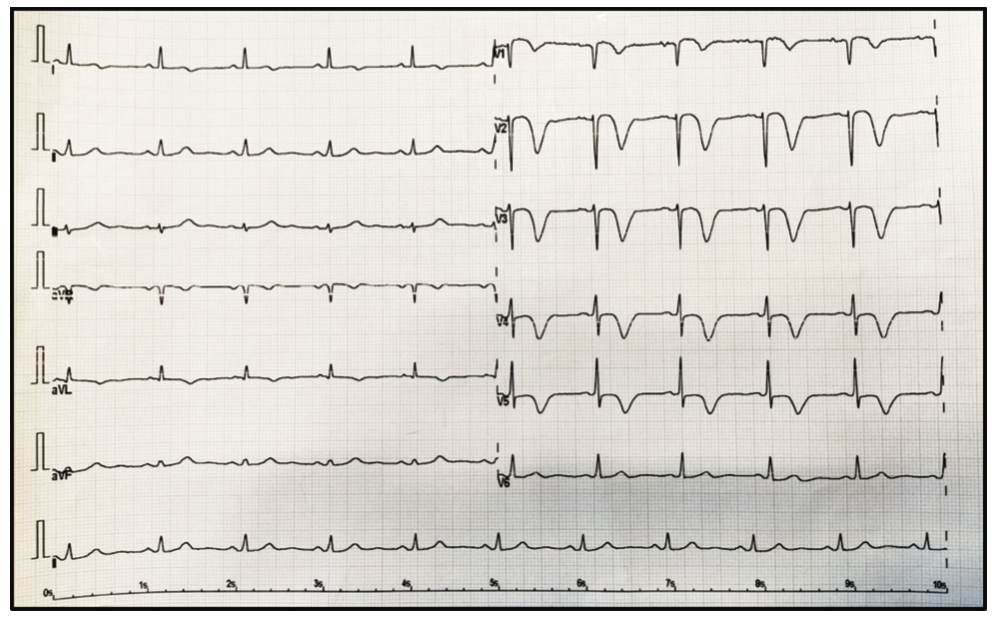
De Winter’s pattern refers to a negative slope of the ST segment from V1 to V3, with a tall and pointed T wave in addition to an elevation of the ST segment in aVR. This pattern is related to total proximal occlusion of the left anterior descending (LAD) coronary artery. There are two types of Wellens’ syndrome patterns: type A, characterized by biphasic T waves in V2 and V3, and type B, with deep and symmetrical negative T waves in precordial leads even up to V5. Type B is the most frequent Wellens’ syndrome pattern and has been correlated with significant stenosis of the LAD in coronary angiography.5,6
The frequency of these electrocardiographic patterns is low and finding them in the same patient is extremely rare. In this report, we discuss whether the coexistence of these patterns is related to an initial occlusion with subsequent spontaneous reperfusion.7
Case Report
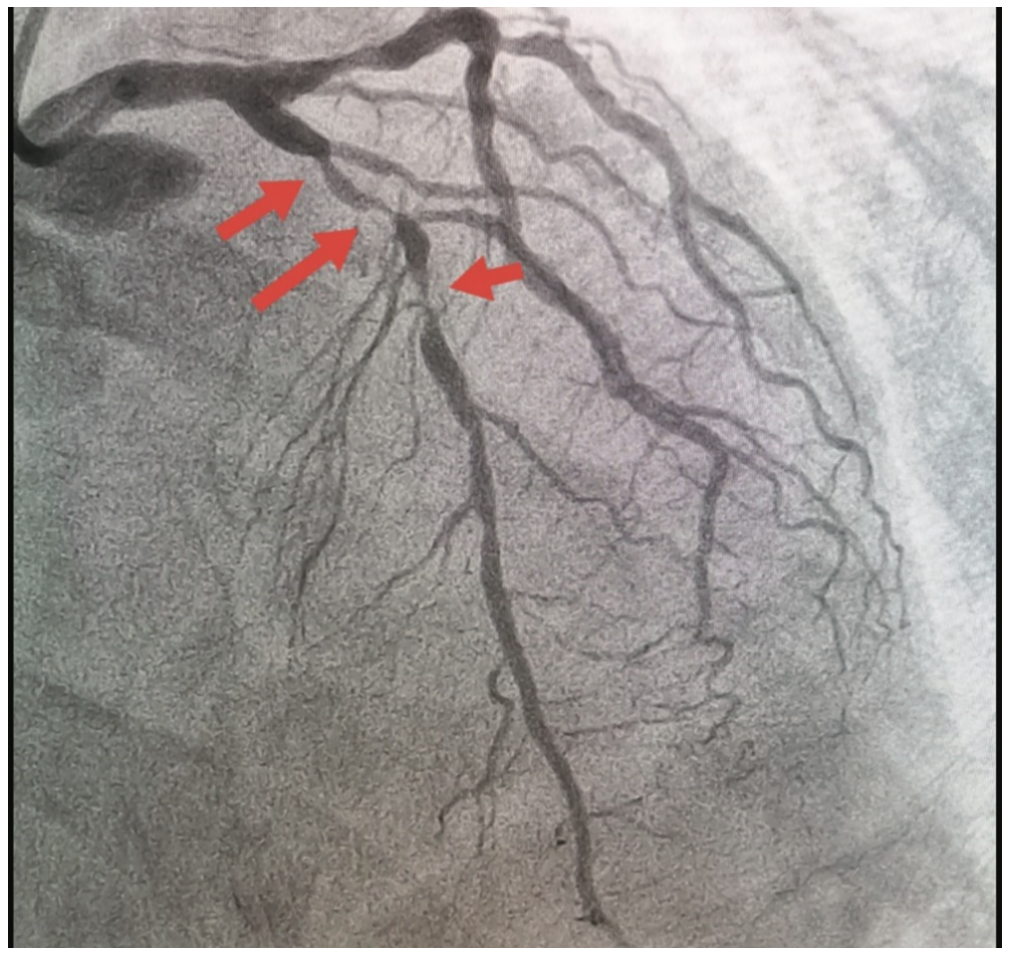
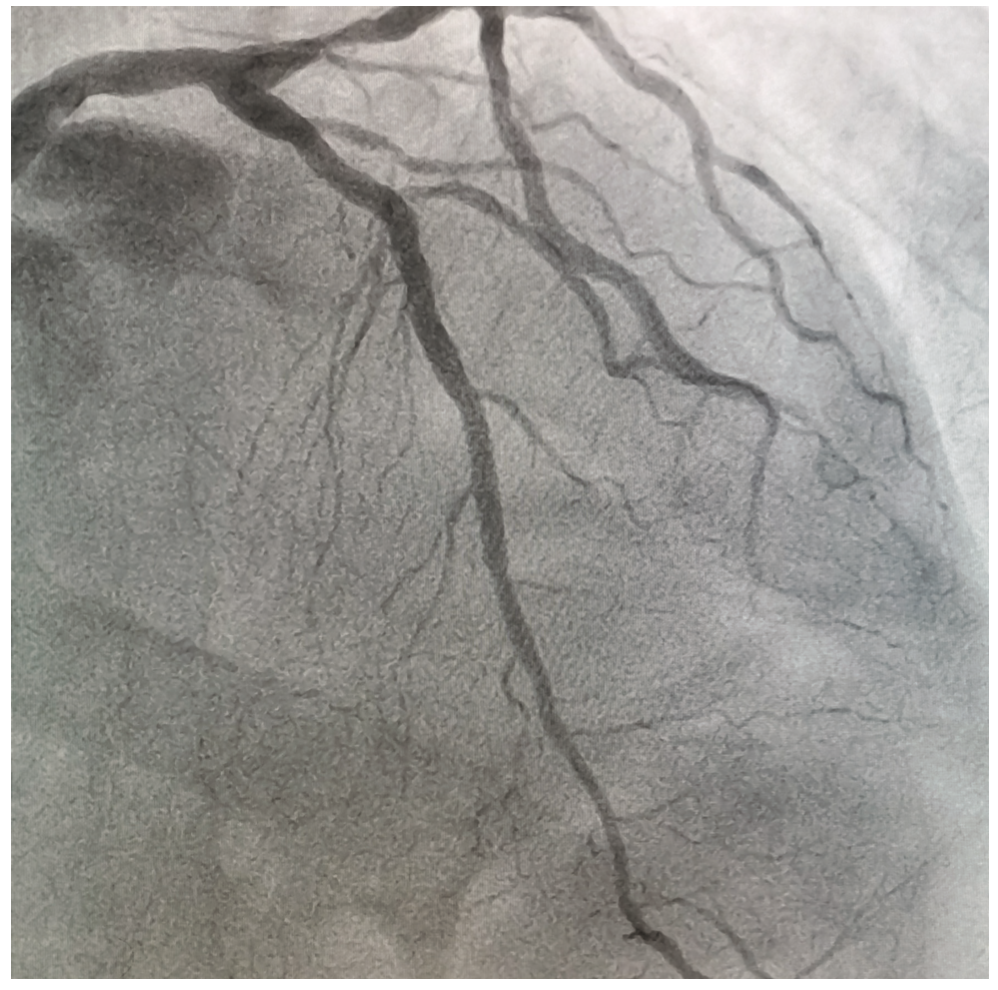
A 69-year-old male with cardiovascular risk factors including hypertension and a sedentary lifestyle presented with typical angina lasting more than 20 minutes. An initial ECG showed de Winter’s pattern (Figure 1) and biomarkers showed a troponin of 12 ng/mL. The patient was then transferred to our center for primary percutaneous coronary intervention. He did not receive thrombolysis, because he was transferred to a center with interventional capacity in less than 2 hours. Upon arrival, a new electrocardiogram was performed where a Wellens’ syndrome type B pattern was observed (Figure 2), suggesting spontaneous reperfusion. The coronary angiogram showed a 99% lesion in the union of the proximal segment with the middle of the LAD with TIMI-3 flow (Figure 3, Video 1). Primary percutaneous coronary intervention with drug-eluting stent implantation was performed, with the final result (Figure 4, Video 1) demonstrating TIMI-3 flow and TIMI myocardial perfusion (TMP) 3.
Video 1. Coronary angiography demonstrating a sub-occlusive lesion at the junction of the proximal and middle segments of the left anterior descending coronary artery.
Conclusion
The electrocardiographic behavior of this case corresponds to an acute total occlusion of the LAD, with the manifestation of a de Winter pattern in the initial ECG (Figure 1). The patient then experienced a spontaneous reperfusion that correlated with the subsequent Wellens’ syndrome type B pattern (Figure 2). We believe knowledge of these particular electrocardiographic patterns is extremely important, since patients benefit from early revascularization as part of the STEMI therapeutic algorithm.4,8
Wellens’ syndrome has been described as occurring in 14% to 18% of patients with unstable angina2,9, while the de Winter pattern is known to be in 2% of patients admitted with anterior wall infarction1. The coexistence of the De Winter and Wellens patterns in the same patient is an extremely rare finding. Of note, spontaneous reperfusion has only been reported in 15% of patients admitted with anterior infarction.10-12
Disclosure: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Juan Guzmán Olea, MD, at dr.jguzmanolea@gmail.com
References
1. de Winter RJ, Verouden NJW, Wellens HJJ, Wilde AAM; Interventional Cardiology Group of the Academic Medical Center. A new ECG sign of proximal LAD occlusion. N Engl J Med. 2008; 359: 2071-2073.
2. de Zwaan C, Bär FW, Wellens HJJ. Characteristic electrocardiographic pattern indicating a critical stenosis high in left anterior descending coronary artery in patients admitted because of impending myocardial infarction. Am Heart J. 1982; 103(4): 730-736. doi:10.1016/0002-8703(82)90480-X
3. Pellizzón OA, Andreani C, Najenson M. Wellens’ syndrome. Rev La Fed Argentina Cardiol. 2015; 44: 114-115. Accessed April 19, 2022. https://www.researchgate.net/publication/281653648_Wellens’_syndrome
4. Asatryan B, Vaisnora L, Manavifar N. Electrocardiographic diagnosis of life-threatening STEMI equivalents: when every minute counts. JACC Case Rep. 2019 Dec 4; 1(4): 666-668. doi: 10.1016/j.jaccas.2019.10.030
5. de la Torre FLM, Pérez FA, Echavarría SL, et al. “De Winter” pattern in patients with non-ST-segment elevation acute coronary syndrome. CorSalud. 2019;11(4):332-336. Accessed April 19, 2022. http://scielo.sld.cu/pdf/cs/v11n4/en_2078-7170-cs-11-04-332.pdf
6. Sankardas MA, Ramakumar V, Farooqui FA. Of occlusions, inclusions, and exclusions: time to reclassify infarctions? Circulation. 2021 Aug 3; 144(5): 333-335. doi: 10.1161/CIRCULATIONAHA.121.055827
7. Farag M, Peverelli M, Spinthakis N, et al. Spontaneous reperfusion in patients with transient ST-elevation myocardial infarction-prevalence, importance and approaches to management. Cardiovasc Drugs Ther. 2021 Jul 10. doi: 10.1007/s10557-021-07226-7
8. Ratzenböck E, Nestelberger T, Kühne M. The Winter gets Well(ens) – a rare pattern of left anterior descending artery occlusion. Cardiovasc Med. 2020; 23: w02089. https://doi.org/10.4414/cvm.2020.02089
9. de Zwaan C, Bär FW, Janssen JH, et al. Angiographic and clinical characteristics of patients with unstable angina showing an ECG pattern indicating critical narrowing of the proximal LAD coronary artery. Am Heart J. 1989; 117(3): 657-665. doi:10.1016/0002-8703(89)90742-4
10. Candelario RV. Síndrome de Wellens y patrón de Winter en deportista joven. Wellens syndrome and “de Winter” electrocardiographic pattern in young athlete. Sociedad Cubana de Medicina Intensiva y Emergencias. 2020; 19(2):19-21. Accessed April 19, 2022. http://www.revmie.sld.cu/index.php/mie/article/view/685/html
11. Carvajal CA, Ardila DJ. Síndrome de Wellens: reconociendo el peligro. Wellens’ syndrome: recognizing the risks. Revista Colombiana de Cardiología. 2015; 22(5): 244-248.
12. Migliore F, Zorzi A, Marra MP, et al. Myocardial edema underlies dynamic T-wave inversion (Wellens’ ECG pattern) in patients with reversible left ventricular dysfunction. Heart Rhythm. 2011 Oct; 8(10): 1629-1634. doi: 10.1016/j.hrthm.2011.04.035


