


“Clot in Transit”: Percutaneous or Surgical Approach?
Abstract
Clot in transit, a rare, life-threatening condition usually associated with pulmonary embolism, is a free-floating thrombus found on the right side of the heart waiting to embolize. The ideal treatment is still unclear, with surgical embolectomy, IV thrombolysis, catheter-directed thrombolysis, or anticoagulation as available options. Here we describe the case of an 80-year-old male who presented as a referral from an outside facility to be considered for catheter-directed thrombolysis after being diagnosed with submassive pulmonary embolism. An emergent transthoracic echocardiogram was done that showed a clot in transit. It was decided that the patient should go for emergent surgical embolectomy given the heavy clot burden. The surgery was uneventful, and the patient made a good recovery and was later discharged on rivaroxaban. This case demonstrates the rare finding of a clot in transit as a cause of submassive pulmonary embolism. The rarity of the disease stems in part from underdiagnosis, given the limited number of echocardiograms performed on patients with pulmonary embolism. Timely initiation of treatment is paramount to prevent the lethal sequelae of the disease. The most appropriate therapy, however, is still unclear for a clot in transit, but surgery appears to be superior, due to the risk with a percutaneous approach.
---
A clot in the right side of the heart is an unusual finding, especially in the absence of structural heart disease and atrial fibrillation. “Clot in transit” is a term that describes a free-floating thrombus in the right side of the heart waiting to embolize to the pulmonary arteries. Clot in transit is rare, with an incidence estimated at 4-18% in patients suffering from pulmonary embolism.1 Right-side clot in transit is considered a medical emergency owing to its high mortality rate, ranging from 21% in 14 days to 29% in 3 months.1 The treatment approach includes surgical embolectomy, thrombolysis, catheter-directed thrombolysis, and anticoagulation. The optimum treatment modality is unclear.2-4 Here we describe a case of bilateral submassive pulmonary embolism, where the patient underwent a successful surgical embolectomy with subsequent anticoagulation and had an excellent outcome.
Case Report
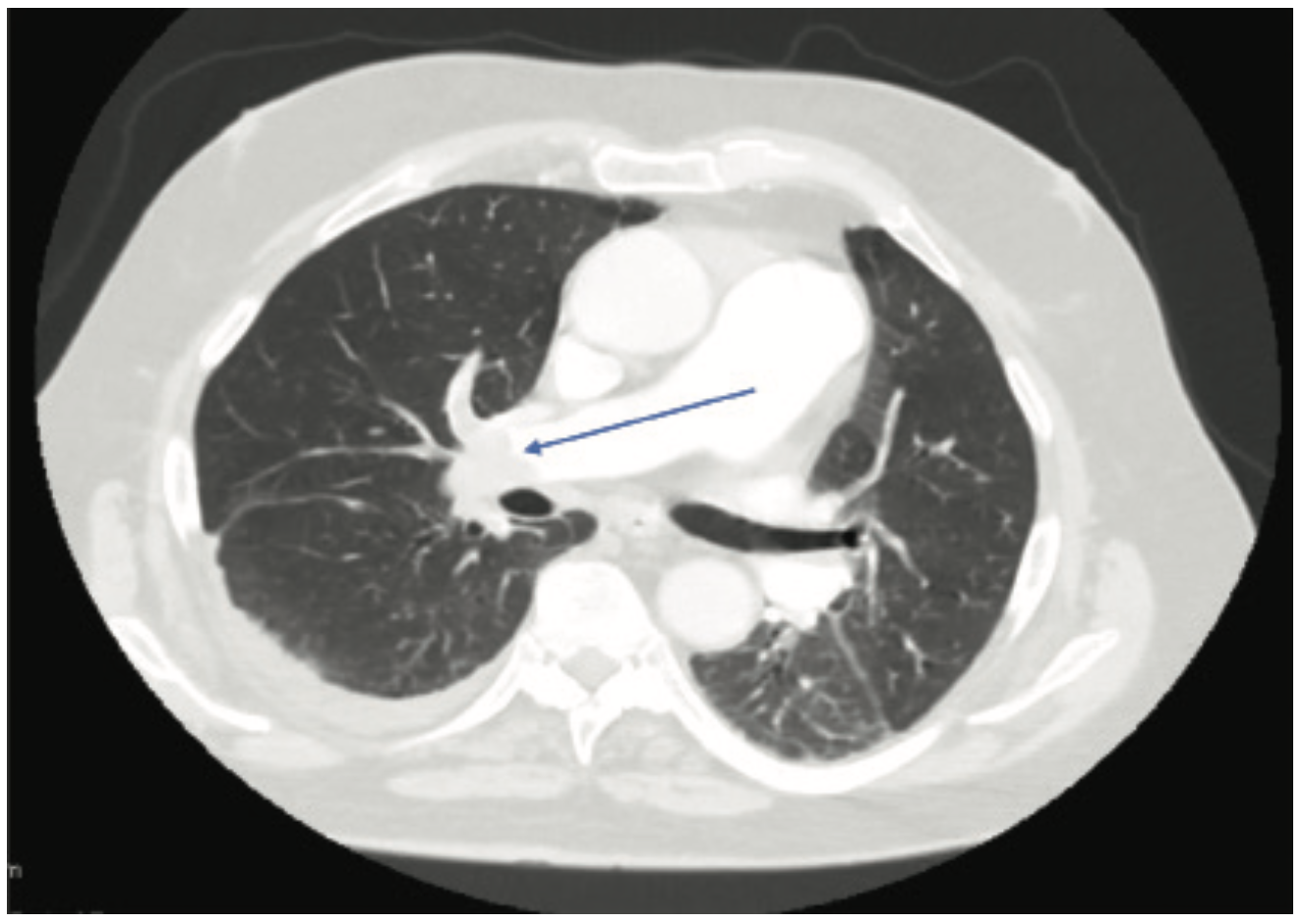
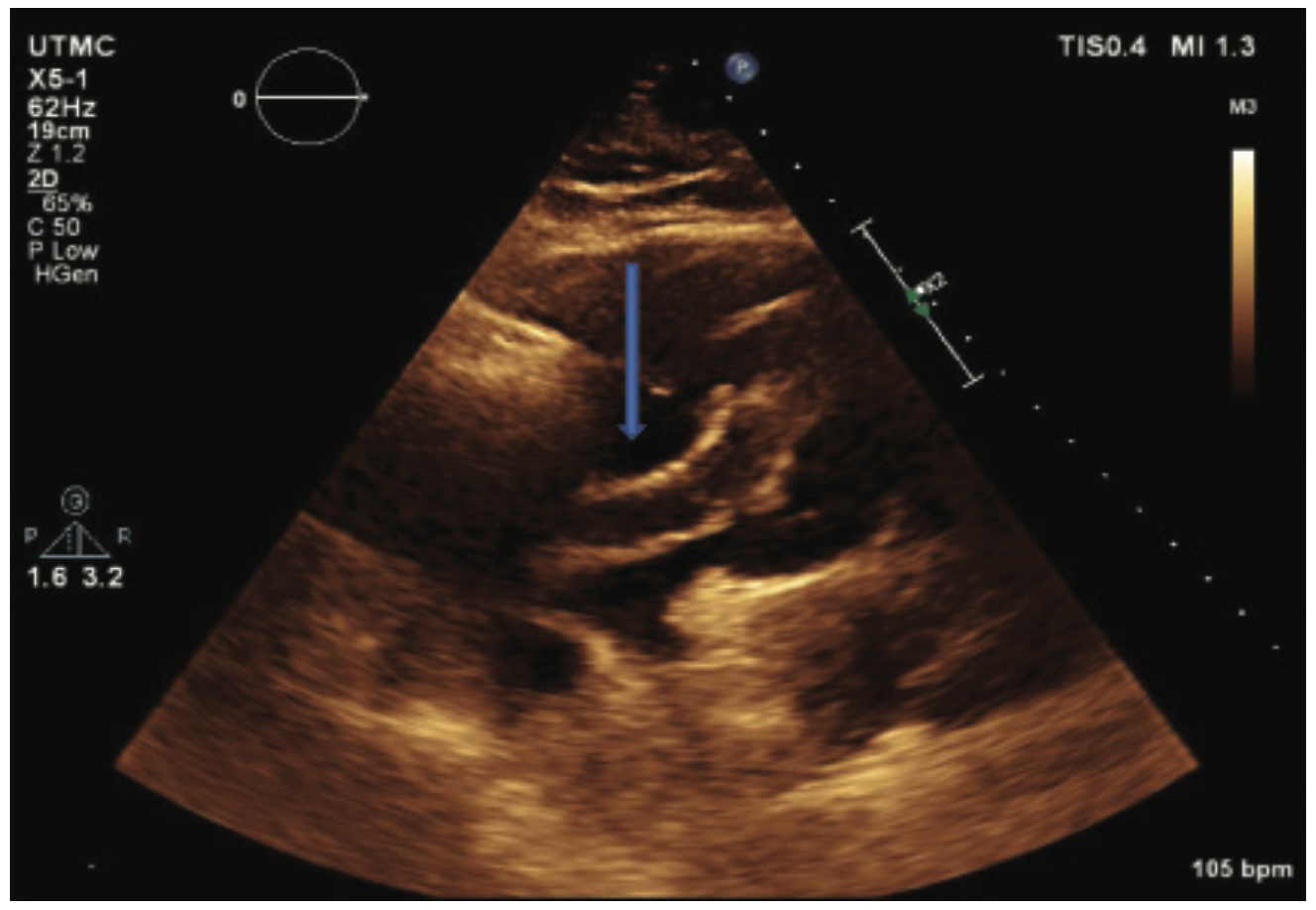
An 80-year-old male with no known past medical history presented to the emergency department at an outside facility with increasing dyspnea for the past ten days. Two weeks prior to his presentation, the patient had a fall. The patient had been immobile since then. Computed tomography (CT) angiogram of the chest showed a completely occluded right pulmonary artery and a partially occluded left pulmonary artery (Figure 1). Duplex of the lower extremity also revealed thrombosis of the left common femoral vein, femoropopliteal, and tibioperoneal veins. His BNP was also noted to be elevated at 306 pg/ml and his troponins were also elevated at 0.09 ng/ml (upper limit was 0.04 ng/ml). As he was hemodynamically stable, the patient was transferred to our facility for possible catheter-directed thrombolysis given his clinical picture of submassive pulmonary embolism. On arrival, an emergent bedside echocardiogram showed a clot in transit from the right atrium to the right ventricle (Figure 2), as well as a severely enlarged right ventricle and moderate tricuspid regurgitation. Due to the huge clot burden, right ventricular strain, and clot in transit, the patient underwent emergent surgical embolectomy. Surgery was successful in removing most of the clot with no complications. Intraoperatively, the clot was found to extend from the right atrium through the tricuspid valve into the right ventricle and all the way to the main pulmonary arteries. There was some residual thrombus in subsegmental areas that was left for medical treatment. The patient had remarkable improvement and was able to go home in a couple of days. He was discharged on rivaroxaban. On follow-up, the patient elected to have an inferior vena cava (IVC) filter placed, which was done successfully. Repeat CT angiography was done 4 months after presentation and showed resolution of the remaining thrombi. The patient continues to do clinically well on outpatient follow-up.
Discussion
Clot in transit of the heart is rare with a higher risk for catastrophic outcomes compared to proximal deep vein thrombosis (DVT), with the latter usually not requiring treatment other than the standard anticoagulation.5 In pulmonary embolism, free thrombi in the right side of the heart are an independent predictor of worse prognosis, with a mortality rate reaching as high as 44%6 compared to a mortality of 11-16% in patients with pulmonary embolism without right ventricular thrombus.1 These high mortality rates highlight the need for timely diagnosis and treatment.
Echocardiography remains the gold standard for risk stratification of pulmonary embolism as well as for making the diagnosis of intracardiac thrombi, with the added benefit of obtaining an idea of the clot origin. Morphologically, the right heart clots can be divided into two types, A and B. Type A clots have a worm-like shape, are very mobile, and usually represent peripheral venous clots that lodge temporarily into the right heart. Type B, on the other hand, are similar in shape to the left heart thrombi, less mobile, attach to the right atrial or ventricular wall, and have broad-based attachment, indicating that Type B clots develop within the right heart.7
Massive and submassive pulmonary embolism with right ventricular enlargement, strain, or positive cardiac biomarkers without intracardiac clots are critical, time-sensitive emergencies that often need multidisciplinary team collaboration for advanced intervention such as extracorpeal membraneous oxygenation as a bridge until proper treatment can be initiated.8 In such patients, catheter-directed thrombolysis has emerged as an important treatment modality alongside systemic thrombolysis and anticoagulation compared to surgical embolectomy.9 The optimum treatment modality for a clot in transit associated with pulmonary embolism is not clearly defined, with one study reporting no significant difference between therapeutic approaches (systemic thrombolysis, surgical embolectomy, catheter-directed thrombolysis, and anticoagulation)with regards to inpatient mortality.2 However, other studies have found some benefit to systemic thrombolysis compared to other treatment modalities10,11, possibly due to a faster initiation of treatment compared to other options.1
Conclusion
Clot in transit in the setting of massive/submassive pulmonary embolism is a life-threatening condition that requires multidisciplinary team involvement for timely diagnosis and urgent treatment. The modality of treatment should be tailored to the patient’s comorbid conditions and the expertise of the treating center should also guide the best course of action. Our patient had no significant comorbidities, and therefore surgical embolectomy was chosen as the safest option for treatment. After surgery, the patient underwent remarkable improvement and continues to do well.
The authors can be contacted via Ebrahim Sabbagh, DO, at ebrahim.sabbagh@utoledo.edu.
- Torbicki A, Galié N, Covezzoli A, et al. Right heart thrombi in pulmonary embolism: results from the International Cooperative Pulmonary Embolism Registry. J Am Coll Cardiol. 2003 Jun 18; 41(12): 2245-2251.
- Chartier L, Bera J, Delomez M, et al. Free-floating thrombi in the right heart: diagnosis, management, and prognostic indexes in 38 consecutive patients. Circulation. 1999; 99(21): 2779-2783.
- Chapoutot L, Nazeyrollas P, Metz D, et al. Floating right heart thrombi and pulmonary embolism: diagnosis, outcome and therapeutic management. Cardiology. 1996; 87(2): 169-174.
- Dalen JE. Free-floating right heart thrombi. Am J Med. 2017 May; 130(5): 501.
- Pacouret G, Alison D, Pottier JM, et al. 9Free-floating thrombus and embolic risk in patients with angiographically confirmed proximal deep venous thrombosis. A prospective study. Arch Intern Med. 1997 Feb 10; 157(3): 305-308.
- de Vrey EA, Bax JJ, Poldermans D, et al. Mobile right heart thrombus and massive pulmonary embolism. Eur J Echocardiogr. 2007 Jun; 8(3): 229-231.
- The European Cooperative Study on the clinical significance of right heart thrombi. European Working Group on Echocardiography. Eur Heart J. 1989 Dec; 10(12): 1046-1059.
- Chowdhury MA, Moza A, Siddiqui NS, et al. Emergent echocardiography and extracorporeal membrane oxygenation: lifesaving in massive pulmonary embolism. Heart Lung. 2015 Jul-Aug; 44(4): 344-346.
- Kearon C, Akl EA, Ornelas J, et al. Antithrombotic therapy for VTE disease: CHEST guideline and expert panel report. Chest. 2016; 149(2): 315-352.
- Dzudovic B, Obradovic S, Rusovic S, et al. Therapeutic approach in patients with a floating thrombus in the right heart. J Emerg Med. 2013 Feb; 44(2): e199-e205.
- Rose PS, Punjabi NM, Pearse DB. Treatment of right heart thromboemboli. Chest. 2002; 121(3): 806-814.



