


SCAI Expert Consensus Document Supports Decreased Length of Stay for PCI
 We are joined this month by Arnold H. Seto, MD, MPA, Chief, Cardiology, Long Beach VA Medical Center, Long Beach, California. Dr. Seto was the chair of the Society for Cardiovascular Angiography and Interventions (SCAI) writing committee responsible for the recent publication Length of Stay Following Percutaneous Coronary Intervention: An Expert Consensus Document Update From the Society for Cardiovascular Angiography and Interventions.1 I interviewed Dr. Seto at the recent annual SCAI Scientific Sessions in San Diego, California, to gain further insight and understanding regarding the decision and rationale behind the recent update of 2009 Expert Consensus Document. There are many physicians and programs who have resisted fully engaging in an established use of a same-day discharge program due to potentially restrictive guidance, as in the 2009 guidelines. — Gary Clifton, Vice President, Terumo Business Edge
We are joined this month by Arnold H. Seto, MD, MPA, Chief, Cardiology, Long Beach VA Medical Center, Long Beach, California. Dr. Seto was the chair of the Society for Cardiovascular Angiography and Interventions (SCAI) writing committee responsible for the recent publication Length of Stay Following Percutaneous Coronary Intervention: An Expert Consensus Document Update From the Society for Cardiovascular Angiography and Interventions.1 I interviewed Dr. Seto at the recent annual SCAI Scientific Sessions in San Diego, California, to gain further insight and understanding regarding the decision and rationale behind the recent update of 2009 Expert Consensus Document. There are many physicians and programs who have resisted fully engaging in an established use of a same-day discharge program due to potentially restrictive guidance, as in the 2009 guidelines. — Gary Clifton, Vice President, Terumo Business Edge
Dr. Seto, thank you for joining me and congratulations to you and the writing committee for this updated consensus document. It has been almost a decade since the previous consensus document, so why now and what was the driving impetus to update the document?
The 2009 document was basically a rearguard action against the economic push from the InterQual (McKesson, now Change Healthcare) criteria taking percutaneous coronary intervention (PCI) off the inpatient-only list. Subsequently, Centers for Medicare & Medicaid Services (CMS) took it off the inpatient-only list as well, basically pushing patients to be reimbursed only at the outpatient level; that outpatient reimbursement scale is typically 28-38% lower than the inpatient scale. So, SCAI, in defense of prior practice and in the absence of good evidence that same-day discharge (SDD) was safe, rightfully said we are concerned by this, we think it needs to be studied more, and that the standard of care was still an overnight stay. Now, ten years later, the evidence is quite clear; eight randomized studies and three meta-analyses have all shown that SDD is safe and has at least equal outcomes in terms of death, major adverse cardiac events (MACE), and readmissions. In terms of other evidence, data and experience suggests any complications a patient might have will generally occur within the first six hours after PCI or after twenty-four hours, and so the traditional overnight stay alone would not be expected to change the outcomes of those complications. So, the driving forces to update the document were that times have changed, the evidence has evolved, and it is clear that SDD is a safe and reasonable, patient-centered option for PCI.
How will the consensus document help assuage or impact any questions physicians or hospitals may have around the medico-legal issues of same-day discharge for PCI patients?
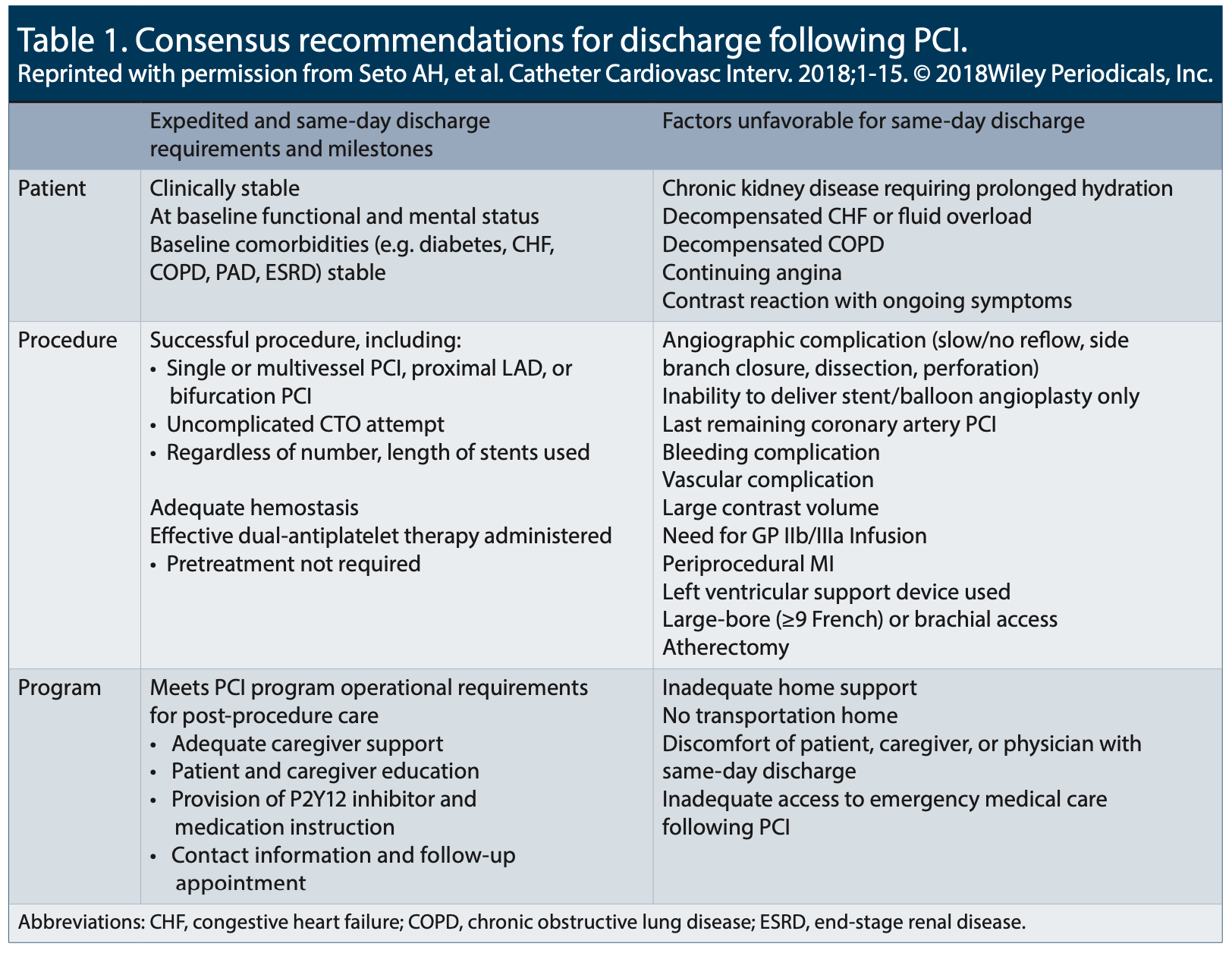
Reprinted with permission from Seto AH, et al. Catheter Cardiovasc Interv. 2018;1-15. © 2018Wiley Periodicals, Inc.
These guidelines are very relevant to medico-legal concerns. SCAI is the only organization that has published guidelines around length of stay (LOS) after PCI and in the 2009 document, explicitly stated that the standard of care for an elective PCI was an overnight stay. My motivation for initiating the process to update this conservative document was based on my concern that the 2009 document could actually inappropriately put a practitioner discharging patients the same day at medico-legal risk. Imagine a patient has a complication after PCI. If they were discharged the same day, an attorney might point to the 2009 document and say that the standard of care was violated. Updating the document to be more flexible and accommodating towards variations in discharge practices (in accordance with the evidence) can only be protective to our member physicians, and thus should have a significant impact as the only document people can point to in terms of guidance for how long a patient should stay in the hospital following a PCI.
Would you consider this document prescriptive?
The current document does not attempt to be prescriptive as to who should be discharged and when. It tries to set out guidance as to what milestones should be achieved in terms of patient, procedural, and program factors, and if all of the aforementioned milestones are met, then SDD is considered reasonable. In contrast to the prior document, the committee made great efforts not to exclude anyone from SDD based on any kind of anatomical factors; for example, the previous document stated that any patient receiving a stent greater than 28 mm, multiple stents, bifurcation stent, or proximal LAD stent should be excluded. Similarly, baseline factors such as comorbidities and age were previously excluded from SDD in the 2009 document, but were removed as exclusions in the document update, as long as the patient is stable and at their baseline state. Such factors, while associated with a higher risk patient and procedure, are not modified by overnight observation. So rather than take an exclusionary approach, we took the opposite approach and came to a consensus that in the absence of any evidence of harm, it is reasonable to discharge the same day if the patient is clinically stable. Overall, the document is trying to support good clinical judgement and not be prescriptive.
The document specifically calls out the 3 “P”s. Can you explain?
The Patient should be stable: they should be at their baseline mental status after conscious sedation. Their comorbidities should be stable in nature, not uncontrolled chronic obstructive pulmonary disease (COPD) or florid heart failure. The Procedure should be successful and have no complications: the vascular access site should be stable without bleeding. The procedure should not necessarily have involved anything extremely high risk such as a large-bore access or a circulatory support device. The Program or programmatic features should have been satisfied, such as having a responsible adult to accompany the patient home, provision for any medications including their dual antiplatelet therapy, subsequent discharge and follow-up paperwork and instructions, and patient education regarding the vascular access site, any potential complications, and when to return to the hospital. All these factors and more are discussed in the document, and should be evaluated before the patient is considered safe for discharge. The advantage of this model is that it is not exclusive to elective PCI, but can be extended to decide when non-elective acute coronary syndrome (ACS) patients can be discharged as well. The patient who has had a small troponin bump and is technically a non ST-elevation myocardial infarction (NSTEMI) patient could conceivably get their PCI and be discharged the same day if they are clinically stable and received their dual antiplatelet therapy. It is based on the clinical judgement of the provider, and we considered these practices reasonable, as opposed to the consensus document that previously excluded them.
In your opinion, is the United States ready for SDD?
Yes, I think the U.S. hospital system is ready, especially to avoid the costs associated with overnight hospitalizations. I think patients are ready, based on surveys that state that they prefer same-day discharge, provided that their practitioner feels it is safe and that they, the patient, feel comfortable with it. Practitioners are one potential resistance point and that will change over time; as providers see the clear evidence that SDD is at least equivalent to overnight hospitalization, they will feel more comfortable discharging patients the same day. I was surprised to see that only 26% of operators were routinely practicing SDD at the present time, but those rates are continuing to increase. We note that nationally, the rate of SDD is approximately 15% of all elective PCIs; it will continue to increase based on the economic and patient drivers, and the clear evidence for patient safety.
I want to thank Dr. Seto and if readers haven’t yet seen or obtained the 2018 consensus document, it can be accessed online: https://onlinelibrary.wiley.com/doi/abs/10.1002/ccd.27637.
In addition, please note that Terumo conducted a physician panel discussion on same-day discharge and the release of the new consensus document at the recent SCAI meeting. We anticipate providing a link to that video shortly.
— Gary Clifton, Vice President, Terumo Business Edge
Reference
- Seto AH, Shroff A, Abu-Fadel M, et al. Length of stay following percutaneous coronary intervention: An expert consensus document update from the society for cardiovascular angiography and interventions. Catheter Cardiovasc Interv. 2018 Apr 24. doi: 10.1002/ccd.27637. [Epub ahead of print]


