


Treating a Rare Delayed Iatrogenic Mid Femoral Pseudoaneurysm After Chronic Total Occlusion Revascularization
 Arterial pseudoaneurysms or “contained ruptures,” are rare complications of endovascular procedures.1 Arterial pseudoaneurysms are characterized by a defect in the layers of the vessel wall that can result in severe pain, nerve compression, or even hemodynamic instability. Treatment is often dependent on the size of the lesion, with larger defects at higher risk for expansion or rupture. Typical treatment modalities include manual compression, thrombin injection, or possibly open vascular repair.2 Usually pseudoaneurysms arise at puncture sites in the common femoral artery. We present a unique scenario of pseudoaneurysm resulting from endovascular repair of a mid superficial femoral artery (SFA) chronic total occlusion (CTO) by re-entry from the subintimal space. This case describes the use of a covered stent to exclude the pseudoaneurysm successfully. This minimally invasive approach could be a viable treatment option for pseudoaneurysms in locations not easily amenable for standard methods of repair.
Arterial pseudoaneurysms or “contained ruptures,” are rare complications of endovascular procedures.1 Arterial pseudoaneurysms are characterized by a defect in the layers of the vessel wall that can result in severe pain, nerve compression, or even hemodynamic instability. Treatment is often dependent on the size of the lesion, with larger defects at higher risk for expansion or rupture. Typical treatment modalities include manual compression, thrombin injection, or possibly open vascular repair.2 Usually pseudoaneurysms arise at puncture sites in the common femoral artery. We present a unique scenario of pseudoaneurysm resulting from endovascular repair of a mid superficial femoral artery (SFA) chronic total occlusion (CTO) by re-entry from the subintimal space. This case describes the use of a covered stent to exclude the pseudoaneurysm successfully. This minimally invasive approach could be a viable treatment option for pseudoaneurysms in locations not easily amenable for standard methods of repair.
Case Report
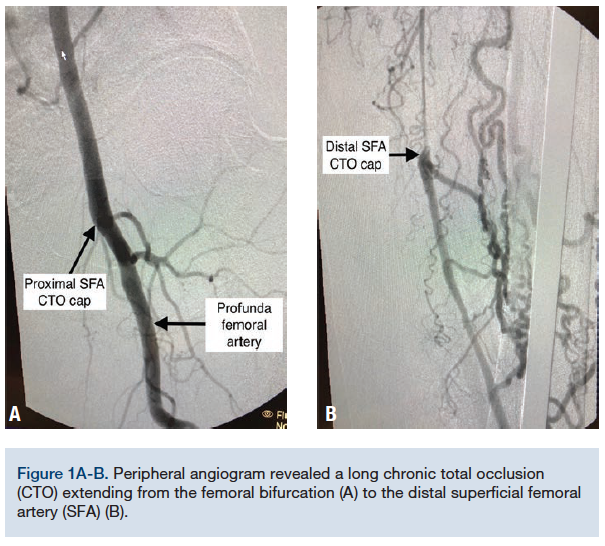
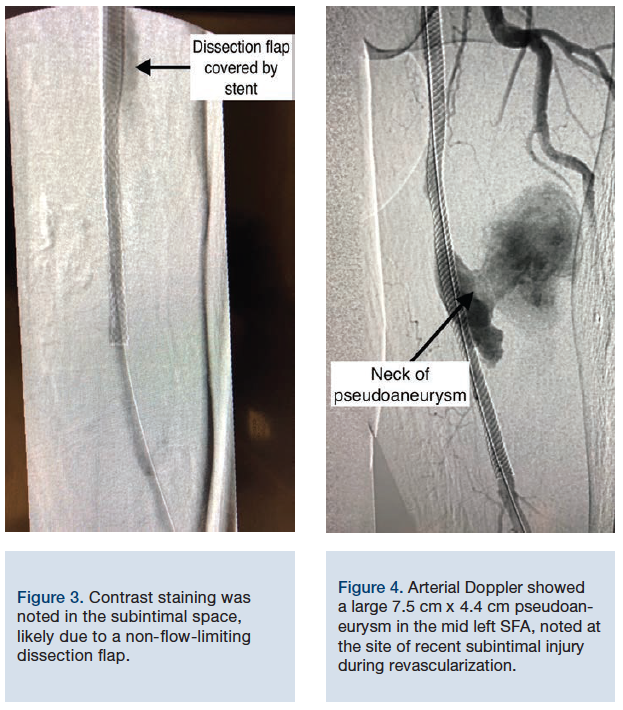
A 73-year-old Caucasian male presented with severe left lower extremity claudication, progressively worsening over the last year despite optimal medical therapy, and a failed exercise walking program. He had a 30-year history of smoking one pack per day and quit smoking 5 years ago. Comorbidities included severe chronic obstructive pulmonary disease and ischemic heart disease. Due to his comorbidities, he was deemed to be at prohibitive risk for surgical bypass. After arterial Doppler suggested severe occlusive disease, he underwent a peripheral angiogram that revealed a long CTO extending from the femoral bifurcation (Figure 1A) all the way to the distal SFA (Figure 1B). He underwent a complex intervention requiring antegrade and retrograde approaches using both right femoral access and left transpedal access. Both approaches were unsuccessful in crossing the occlusion. Tandem overlapping simultaneous balloon inflations were performed in the subintimal space, creating a connection to the true lumen (Figure 2). We were then able to advance a wire and complete the revascularization with angioplasty and stenting from the transpedal approach. Contrast staining was noted in the subintimal space that was likely due to a non flow-limiting dissection flap (Figure 3).
Post procedure, the patient had immediate resolution of his claudication and was doing well. However, one week later, he developed sudden, severe, mid-thigh pain, prompting him to present to the emergency department. On physical exam, distal pulses were normal, but the left thigh was firm and extremely tender, with limited flexion and extension due to pain. He was unable to ambulate and arterial Doppler showed a large 7.5 cm x 4.4 cm pseudoaneurysm in the mid left SFA, noted at the site of recent subintimal injury during revascularization (Figure 4). The stent was patent. Due to its size and location, the decision was made to attempt percutaneous covered stent placement in order to occlude the neck of the pseudoaneurysm.

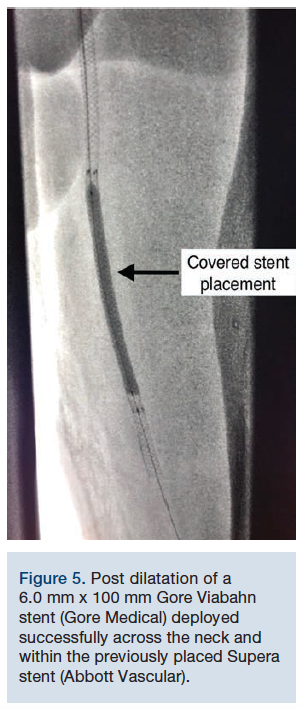
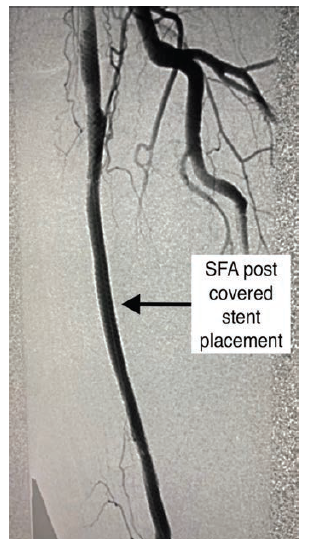
From the contralateral vascular access site, a 55 cm Raabe sheath (Cook Medical) was placed across the iliac bifurcation. An .018-inch Steelcore guidewire (Abbott Vascular) was advanced distal to the pseudoaneurysm and the decision was made to exclude it with a covered stent. A 6.0 mm x 100 mm Gore Viabahn stent (Gore Medical) was deployed successfully across the neck and within the previously placed Supera stent (Abbott Vascular) without complication. Post dilation was performed with excellent final angiographic results (Figures 5-6) showing patency of the SFA with successful exclusion of the pseudoaneurysm. The patient had immediate improvement in pain and was back to normal activity levels one week later. He was maintained on apixaban 5 milligrams twice a day and clopidogrel 75 milligrams daily.
Discussion
The Gore Viabahn balloon-expandable covered stent is a metal stent covered with a synthetic fabric of polytetrafluoroethylene (PTFE). It is frequently used to treat arteriovenous fistula lesions. This case directly highlighted the efficacy of using a covered stent to resolve a contained rupture that occurred in an unusual location. Gabrielli et al suggest that thrombin injections are safe and effective in treating simple iatrogenic pseudoaneurysms.3 However, due to the deep nature of the SFA, more conservative measures such as manual compression or thrombin injection would likely have been unsuccessful. Open surgical repair would involve a lengthy recovery time and was a higher risk in this particular patient.4
While pseudoaneurysms are usually located in the common femoral artery, this location is not optimal for covered stents due to a high risk of occluding the profunda femoral artery. There is also the possibility of stent fracture due to artery manipulation during hip flexion. However, the rare mid SFA pseudoaneurysm is an ideal location for correction with covered stent. A literature review has shown small cohorts in Asia using a similar approach in select patients. Xu et al evaluated a small group of drug users in China with self-inflicted femoral artery pseudoaneurysms and found that there was 100% procedural success rate that correlated with clinical improvement.5 Samara et al published a case report of an idiopathic SFA pseudoaneurysm that was successfully treated with covered stenting in Jordan.6 Although an off-label use of the device, the low risk and high reward rates identify a viable new treatment modality that could potentially replace the need for open surgical repair in the correct patient population. As indications for percutaneous procedures expand, endovascular operators will need to continue to remain familiar with all treatment modalities.
1University of North Texas Health Science Center, Fort Worth, Texas.
2Medical Director of Interventional Cardiology, Baylor Heart and Vascular Hospital, Fort Worth, Texas.
Disclosures: The authors report no conflicts of interest regarding the content herein.
The authors can be contacted via Hamza Malik, MS, OMS-1, at hamza.malik@my.unthsc.edu.
- Katzenschlager R, Uguruoglu A, Ahmadi A, et al. Incidence of pseudoaneurysm after diagnostic and therapeutic angiography. Radiology. 1995; 195: 463.
- Kreuger K, Zaehringer M, Strohe D, et al. Postcatheterization pseudoaneurysm: results of US-guided percutaneous thrombin injection in 240 patients. Radiology. 2005; 236: 1104.
- Gabrielli R, Rosati MS, Vitale S, Siani A, Caselli G. Thrombin injection and compression with removable guidewire in the treatment of postcatheterization femoral pseudoaneurysm. J Cardiovasc Surg (Torino). 2016 Aug; 57(4): 510-513.
- Kleczynski P, Rakowski T, Dziewierz A, Jakala J, Dudek D. Ultrasound-guided thrombin injection in the treatment of iatrogenic arterial pseudoaneurysms: single-center experience. J Clin Ultrasound. 2014 Jan; 42(1): 24-26.
- Xu J, Zheng Z, Yang Y, Zhang W, Zhao H, Bei E, Zheng M. Clinical evaluation of covered stents in the treatment of superficial femoral artery pseudoaneurysm in drug abusers. Mold Med Rep. 2018 Mar; 17(3): 4460-4466.
- Samara O, Saleh A, Alomari A, Nosaiba A, Hadidy A, Alsmady M. Giant spontaneous femoral artery pseudoaneurysm treated with covered stents. Sultan Qaboos Univ Med J. 2013 Aug; 13(3): E472-E475.


