


Improving Cardiac Imaging Quality at the Long Beach VA Cardiac Cath Lab: Results of a Nurse-Driven QI Project
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of Cath Lab Digest or HMP Global, their employees, and affiliates.
Autumn Baldwin, BSN, RN, RCIS; Miles Mesina, BSN, RN
Long Beach Veteran’s Administration Medical Center, Long Beach, California
The authors can be contacted via Autumn Baldwin, RN, BSN, RCIS, Cardiac Cath Lab Educator, at autumn.baldwin@va.gov
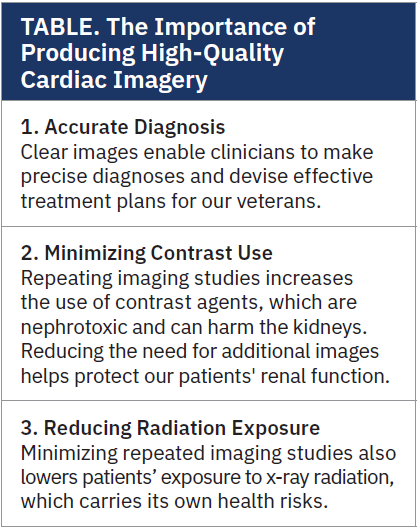 At the Long Beach VA Cardiac Catheterization Lab, we recently faced a critical challenge: our coronary angiography imaging quality was not meeting the high standards necessary for optimal patient care (and for useful images in the CathWorks FFRangio system). Through an extensive interdisciplinary discussion involving radiologic technologists, nurses, and other healthcare professionals, we identified that the primary issue affecting our imaging quality was the presence of artifacts producing suboptimal results. We know that high-quality images are crucial for making correct clinical decisions (Table). When these images are degraded or obscured by artifacts, they can be uninterpretable or confusing.
At the Long Beach VA Cardiac Catheterization Lab, we recently faced a critical challenge: our coronary angiography imaging quality was not meeting the high standards necessary for optimal patient care (and for useful images in the CathWorks FFRangio system). Through an extensive interdisciplinary discussion involving radiologic technologists, nurses, and other healthcare professionals, we identified that the primary issue affecting our imaging quality was the presence of artifacts producing suboptimal results. We know that high-quality images are crucial for making correct clinical decisions (Table). When these images are degraded or obscured by artifacts, they can be uninterpretable or confusing.
The clinician, by necessity, then must repeat part of the procedure, leading to additional radiographic contrast administration impacting renal function, as well as having increased radiation exposure to both the team and the patient.
Identifying the Problem
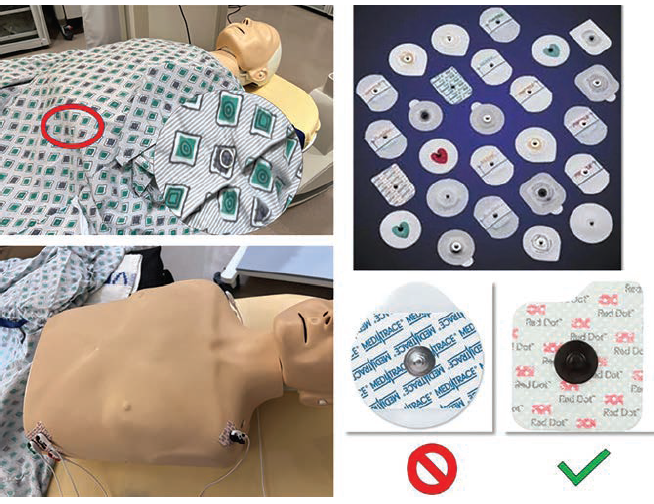
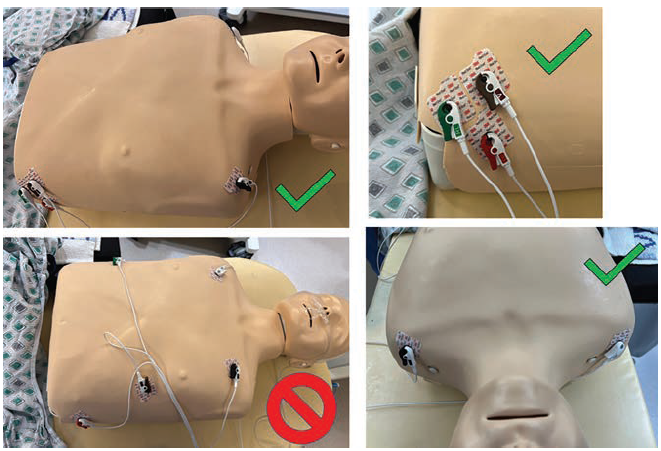
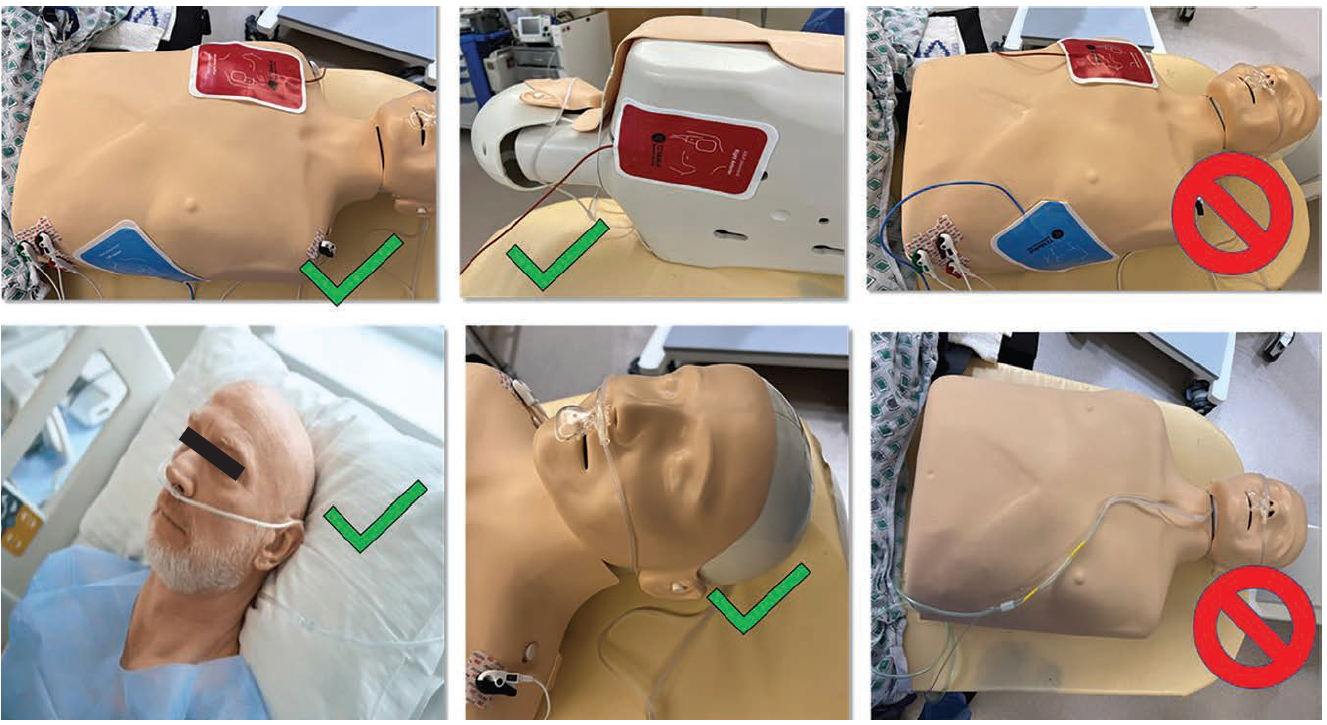
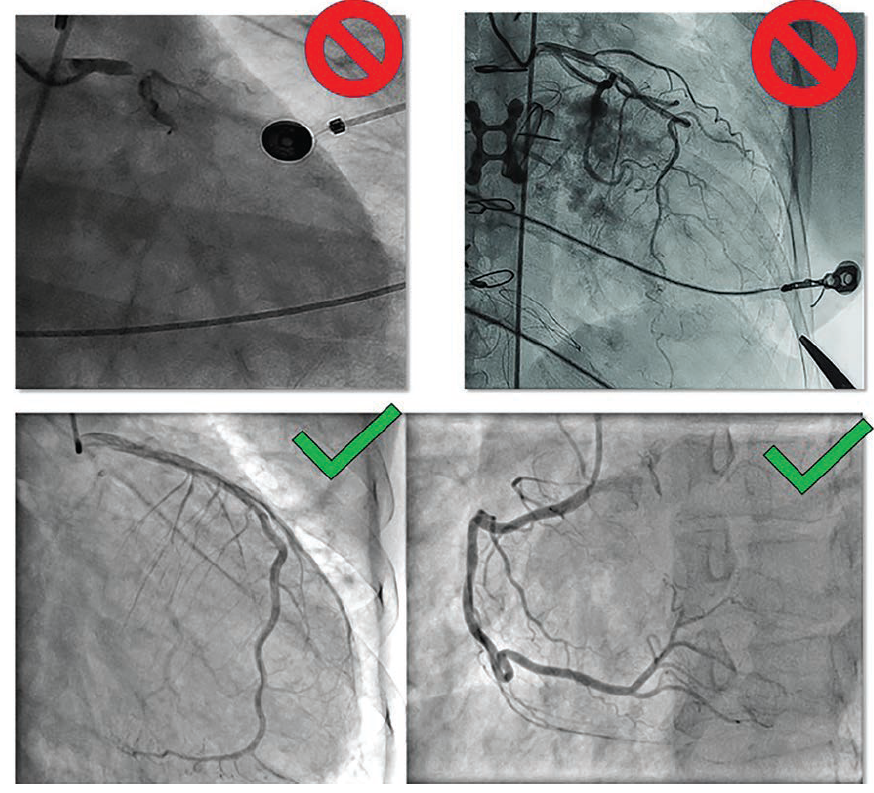
Artifacts in radiographic medical imaging are any unwanted elements or conditions that obscure the clarity of the images. Foreign objects in the image field can compromise the quality of the cardiac structures and may overlap with coronary vessels, making for an inaccurate interpretation. In the cath lab, some of these artifacts include wires or patches from electrocardiogram (EKG) leads, metal objects from gowns, underwear or jewelry (or metal prostheses), oxygen tubing, CO2 cables, and defibrillator pads (Figures 1-4). Some imaging artifacts were out of our control; that is, they were due to problems related to the operator’s technique of coronary arteriography and the activities performed by the physician operators. Proper angiographic techniques are designed to reduce or eliminate artifacts due to contrast streaming, vessel or branch overlap, image foreshortening, poor contrast injection, or any x-ray function (eg, underexposure or overexposure), any or all of which can reduces adequate image opacification. There are patient-related artifacts from implanted devices, like pacemakers, loop recorders, implantable cardioverter defibrillators (ICDs), coronary artery bypass graft (CABG) sternal wires, or orthopedic metal joints that may obscure or degrade image quality. Again, any physician-directed or patient-related artifacts, such as positioning, angiographic setup, and contrast injections were not part of this quality improvement project.
Action Plan for Improvement
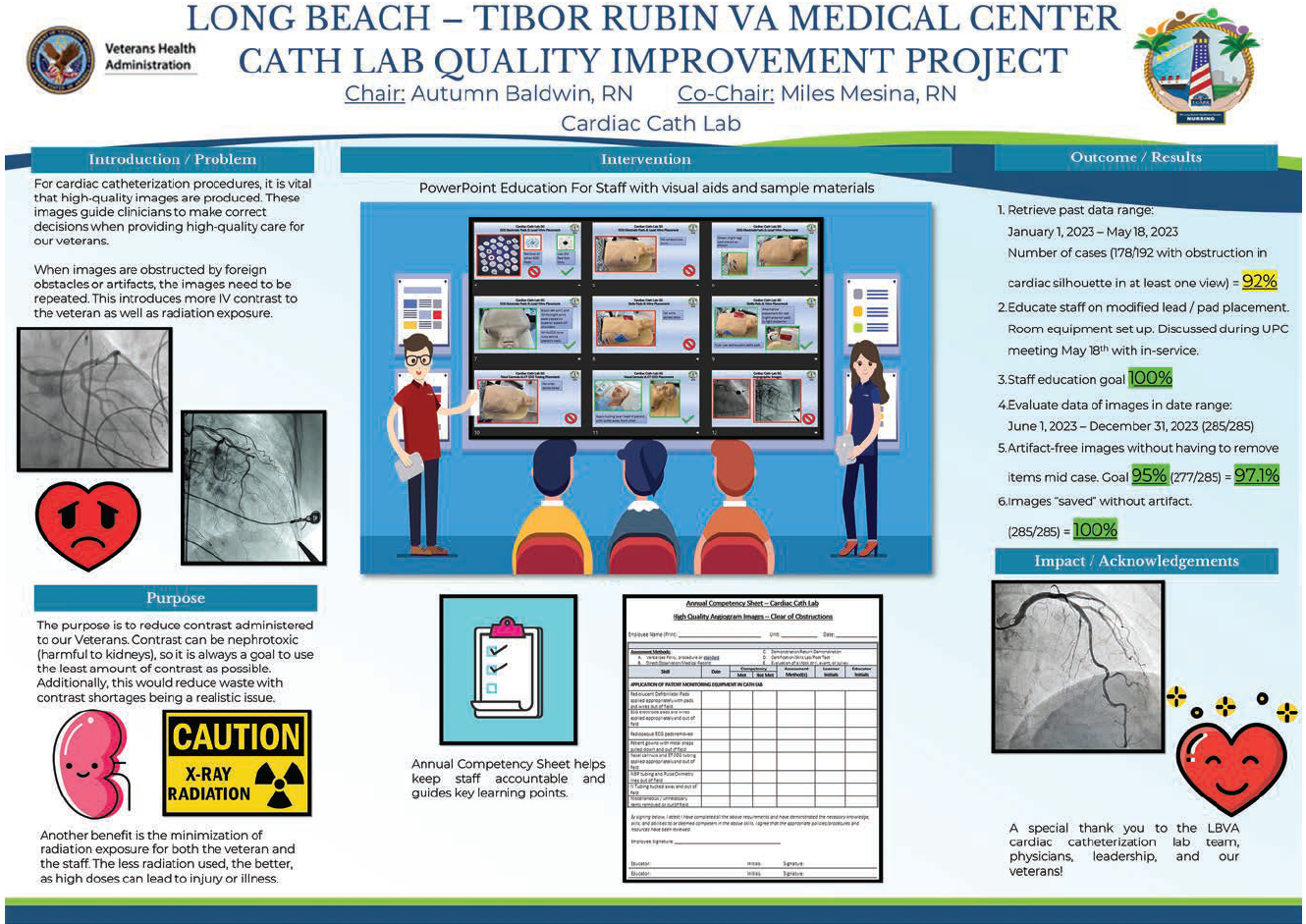
To address the issue, we conducted a thorough review of our past cases and found that an overwhelming number (92%) of our cardiac structural images contained some form of artifact. This alarming statistic prompted our immediate action. We developed a comprehensive educational initiative aimed at all staff members involved in cardiac imaging.
Components of the Educational Initiative
We proposed a 3-step approach.
Step 1: Creating Educational Materials.
We developed a series of visual aids and sample materials to clearly demonstrate the types of artifacts and their impact on imaging quality.
Step 2: Implementing Staff Training. Educational material, in the form of a PowerPoint presentation (example shown as part of Figure 5), was delivered to every staff member involved in the cath lab and imaging process. The training sessions emphasized the importance of removing potential artifacts before imaging and provided practical tips on how to do so effectively.
Step 3. Validating Results With Annual Competency Retraining. To ensure sustained improvement, we instituted an annual competency assessment. This involved tracking the frequency of necessary adjustments or retakes due to artifacts, and provided a metric for continuous improvement.
Monitoring and Results
We closely monitored the impact of our educational initiative over the following months. The results were remarkable. In the first month after implementing the new protocols, our success rate for artifact-free images improved dramatically, to 95-97%. By the third month, we achieved a 100% success rate, with all cardiac structural images free of artifacts and no need for retakes.
Limitations to Our Initiative
Although we achieved a high success rate with significantly improved imagery on the first attempt, we were unable to precisely calculate the exact dose of radiation and contrast reduction that would have been associated with fewer retakes, because each patient required specific views and operator-selected additional imaging with a highly variable contrast dose to visualize the vessels. In addition, some patients went on to have a percutaneous coronary intervention or additional studies. Lastly, we could not control for patient-related devices, which may have required additional images to visualize the coronary arteries without being obscured by device/vessel overlap.
Conclusion
The success of our initiative at the Long Beach VA Cardiac Cath Lab underscores the importance of continuous education and process improvement in healthcare settings. By addressing the root cause analysis of imaging artifacts and implementing targeted training, we were able to significantly enhance the quality of our cardiac imaging. This, in turn, has allowed our clinicians to make more accurate diagnoses and provide better care for our veterans, while also reducing the risk of nephrotoxicity and radiation exposure.
Our experience also highlights a crucial lesson for healthcare facilities everywhere, namely, investing in staff education and increasing attention to details that can lead to substantial improvements in patient care outcomes. The Long Beach VA Cardiac Cath Lab is now better equipped to provide the highest quality cardiac imagery, ensuring that our veterans receive the best possible care.
Sources and Recommended Reading
Rigatelli G, Gianese F, Zuin M. Modern atlas of invasive coronary angiography views: a practical approach for fellows and young interventionalists. Int J Cardiovasc Imaging. 2022 May; 38(5): 919-926. doi:10.1007/s10554-021-02489-5
Sorajja PS, Lim MJ, Kern MJ. (Ed.) Chapter 3. Coronary Angiography. In: Kern’s Cardiac Catheterization Handbook, 7th Ed. Elsevier; 2020.


