



Promoting Innovation in EMS: Business Acumen Part 4—Putting It All Together
Over 2018 EMS World, in conjunction with the National Association of EMTs, will provide detailed implementation strategies for key recommendations of the Promoting Innovation in EMS (PIE) project. The PIE project utilized broad stakeholder involvement over four years to identify and develop guidance to overcome common barriers to innovation at the local and state levels and foster development of new, innovative models of healthcare delivery within EMS. Each month we will focus on one recommendation and highlight the document’s actionable strategies to continue the EMS transformation.
Over the last three columns we’ve discussed the costs of traditional EMS delivery, done a deep dive into revenue analysis, and explored the costs of innovative EMS delivery models. In our final column on EMS financial acumen, let’s put it all together and look at alternative payment models for EMS.
Economic Models 1.0 and 2.0
Since the inception of Medicare in 1965, ambulance transportation has been a covered benefit for Medicare beneficiaries.1 The key word in that sentence is transportation. If transportation is not supplied, Medicare coverage is not available (with one minor exception involving the cessation of CPR and presumption of death on scene by the ambulance crew). EMS is paid based on the transportation supplied, not the medical care provided. This is why Medicare generally refers to ambulance services as suppliers, not providers.
The current economic model for EMS is volume-based and simple: The more transports we do, generally, the more we get paid. Prior to 2002 each EMS agency billed according to its own pricing scheme, generally above their average cost (model 1.0). Following the introduction of the prospective payment schedule in 2002, EMS agencies billed according to a formula that involved the level of service and mileage but was still based on fee-for-service, with the service being transportation (model 2.0).
As the healthcare system moves toward value-based and outcome-driven economic models, our model becomes antiquated and, frankly, incompatible with demonstrating value. Few studies empirically show patient outcomes are better because they arrived at the hospital by ambulance as opposed to private vehicle, police car, or ride-share. In fact, the opposite has been shown: BLS care in cardiac arrest has better outcomes than ALS care, and penetrating trauma victims transported by police car have better survival rates.2,3
Alternative Economic Models (Model 3.0)
Let’s apply what we’ve learned in our previous columns to some alternative economic models being piloted across the country.
Ambulance response, treatment, and nontransport—Anthem announced in October 2017 it would reimburse ambulance services for response and treatment without transport in all 14 states in which it operates.4 The Healthcare Common Procedure Coding System (HCPCS) code for that service is A0998. Historically that HCPCS code has not been paid by Medicare and most insurers who follow the Medicare guidelines because Medicare does not consider A0998 a covered benefit (because there was no transport). But Anthem desired to decouple payment from transport as a way to remove the economic incentive for ambulance services to transport patients to EDs just to get paid. It is now paying medically necessary claims billed under the A0998 HCPCS code at 75% of the statewide average amount allowed for an ambulance transport.
Let’s run the numbers: If the statewide average ambulance transport payment allowable for Anthem were $800, a billed A0998 nontransport claim would be paid $600 (75% of $800). Recall that Anytown EMS’ average commercial payer revenue per transport was $800, so the ability to collect $600 as opposed to $0 for the nontransport would help keep Anytown EMS relatively fiscally whole for the response, even without transport.
Payment for treat-and-refer—Some payers, most notably Arizona Medicaid (AHCCCS), have begun paying for EMS response and referral without ambulance transport.5 Note the deliberate use of the terms EMS and ambulance. Under the AHCCCS pilot an EMS agency is eligible for the treat-and-refer payment even if it isn’t an ambulance supplier. In the AHCCCS program a first-response agency can respond to a 9-1-1 call, assess, treat, and refer the patient, then bill Arizona Medicaid for the service, even though they are not a licensed ambulance provider. The AHCCCS payment for this service is $203.80.
Recall that Anytown’s first-response cost per call was $50 ($50,000 annual cost to operate ÷ 1,000 responses). Receiving $203.80 for the response, if there is no transport, more than covers its cost.
Payment for the response vs. the transport—Under this model the ambulance is paid for the response whether or not the patient is transported. On the surface it may seem the same as the A0998 payment for nontransport, except the payment is the same whether the patient is transported or not. Under the A0998 model the ambulance is paid $600 for a nontransport and $800 for a transport. In the response-payment model, the payment is the same.
This means Anytown would have to determine the right payment for the response so it doesn’t lose money under the new model, especially considering the program may need to account for the additional costs of training providers and/or implementing new technologies to facilitate triage decisions. There may also be additional costs for online medical direction (if that is part of the triage process) and medical oversight and QA due to the added complexity of patient navigation.
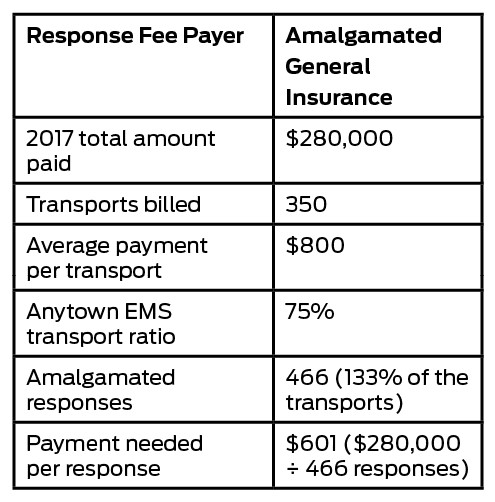
Let’s look at the numbers. Using this analysis, if Amalgamated General Insurance (AGI) offered at least $900 per response, Anytown EMS would generate the same revenue regardless whether the patient was transported. But as we explained in a previous column, Anytown should not be the one to propose the price. It’s possible AGI may be willing to pay more than $900 because it’s looking at potentially reducing downstream ED claim payments.
Population-based payment—This model is a little more complicated, but we can use all the data generated about the cost of service delivery and payment models to help calculate payments under it. A population-based payment is generally a fixed amount per covered member of the health insurer and is typically paid per month. The provider does not bill for each encounter. You may have heard this model referred to as a capitated or per member per month fee.
Let’s use the AGI example above, with the additional information that AGI has 5,000 insured members in Anytown’s jurisdiction. AGI paid $420,000 for ambulance transports in 2017 for the 5,000-member population. That’s an annual amount of $84 per member per year. Dividing that amount by 12 months is $7 per member per month. Each month AGI would pay Anytown $7 per insured member who resides in Anytown, or $35,000. The actual payment to Anytown EMS may change as the number of insured members changes, but the $7 is fixed. If an AGI member uses Anytown’s service, no bill is generated, since the capitated amount has already been paid, although it’s probable that Anytown would provide a monthly report to Amalgamated showing the number of member encounters it had.
Since it’s generally difficult to predict actual ambulance utilization, most capitated payment arrangements include a “risk corridor” to account for significant fluctuations in service utilization. This amount is typically 5%. This means that if the average transport volume for Amalgamated members is 29 calls per month, the call volume per month could fluctuate between 27 and 31. If the call volume trends higher or lower than that, the monthly payments could be adjusted.
If AGI desired services from Anytown that were more than just ambulance transport (MIH services, etc.), Anytown could add its costs for providing those services to the PMPM amount. For example, if Anytown estimated the MIH costs at $100,000 per year, plus a 5% risk corridor and another 5% for retained earnings, annually the charge to AGI for the MIH innovation would be $110,250, or $1.84 PMPM (110,250 ÷ 5,000 ÷ 12), for a total PMPM for ambulance and MIH services of $8.84.
For More
Sound complicated? Don’t worry—there’s help! The National Association of EMTs’ MIH-CP toolkit has electronic workbooks with examples EMS agencies can use as templates to perform this type of modeling.6
References
1. Centers for Medicare & Medicaid Services. CMS’ program history, www.cms.gov/About-CMS/Agency-information/History/.
2. Reinberg S. More Advanced Emergency Care May be Worse for Cardiac Arrest Victims: Study. U.S. News & World Report, https://health.usnews.com/health-news/articles/2014/11/24/more-advanced-emergency-care-may-be-worse-for-cardiac-arrest-victims-study.
3. Wandling MW, Nathens AB, Shapiro MB, et al. Association of Prehospital Mode of Transport With Mortality in Penetrating Trauma. JAMA, 2018 Feb; https://jamanetwork.com/journals/jamasurgery/article-abstract/2654239.
4. Erich J. ‘The Moment We’ve Been Waiting For’: Anthem to Compensate EMS Care Without Transport. EMS World, www.emsworld.com/news/218925/moment-weve-been-waiting-anthem-compensate-ems-care-without-transport.
5. Arizona Health Care Cost Containment System. Treat and Refer Recognition Program, www.azahcccs.gov/PlansProviders/NewProviders/treatandrefer.html.
6. National Association of Emergency Medical Technicians. MIH-CP Program Toolkit, https://www.naemt.org/initiatives/mih-cp/mih-cp-program-toolkit.
Matt Zavadsky, MS-HSA, NREMT, is chief strategic integration officer at MedStar Mobile Healthcare, the exclusive emergency and nonemergency EMS/MIH provider for Fort Worth and 14 other cities in North Texas. He is a member of the EMS World editorial advisory board.
Kevin G. Munjal, MD, MPH, is an emergency physician who completed an EMS fellowship with the New York City Fire Department (FDNY). He is founder and chair of the New York Mobile Integrated Healthcare Association (NYMIHA), an organization seeking to empower EMS providers to play a larger, more integrated role within the healthcare system by promoting new models of mobile healthcare.







