



CE Article: Emergency Care in Athletics, Part 1

Objectives
- Upon conclusion of this activity, participants will be able to:
- Understand the various healthcare providers that make up the sports medicine team;
- Be able to describe the components of an emergency action plan (EAP) in athletics;
- Be able to recognize the importance of conducting training on the EAP;
- Understand use of the medical time-out as a tool to foster collaboration among members of the sports medicine team.
A 2014 consensus document spearheaded by the National Athletic Trainers’ Association (NATA) reported that an estimated 1.4 million secondary school athletes across nine sports, and approximately 209,000 college athletes across 25 NCAA sports, are injured annually in the United States.1 These injuries range from minor sprains and strains to more emergent conditions such as cervical spinal injuries. Additionally, the CDC reports that 2.6 million children up to 19 are treated in emergency departments each year for sports- and recreation-related injuries.2
When an athlete is injured, it poses the question of who takes care of them. While the simple answer to this is a physician of one specialty or another, the truth is that it is often a variety of different healthcare providers. This group generally all possess some background or expertise in the area of sports medicine, an umbrella term for the medical care provided to athletes.
While the entry-level EMS provider does not receive any specialized training in sports medicine, EMS is actually a component of this sports medicine team—and an important one. This article is intended to provide a more in-depth understanding of this team, the role of EMS within it, and ways EMS providers can participate.
The second part of this series will review common emergent conditions encountered in the sports arena.
The Sports Medicine Team
The sports medicine team is anyone who contributes to the care of an injured athlete. While the makeup of this group may differ depending on things like the geographic location or financial status of a school, some component of a sports medicine team will exist.
Most commonly an athletic trainer will lead this team. While commonly known for things like taping ankles and providing athletes with water, athletic trainers are actually multiskilled allied healthcare providers trained especially for handling prevention and treatment of injuries and illnesses in the physically active population (for more information see www.nata.org).3
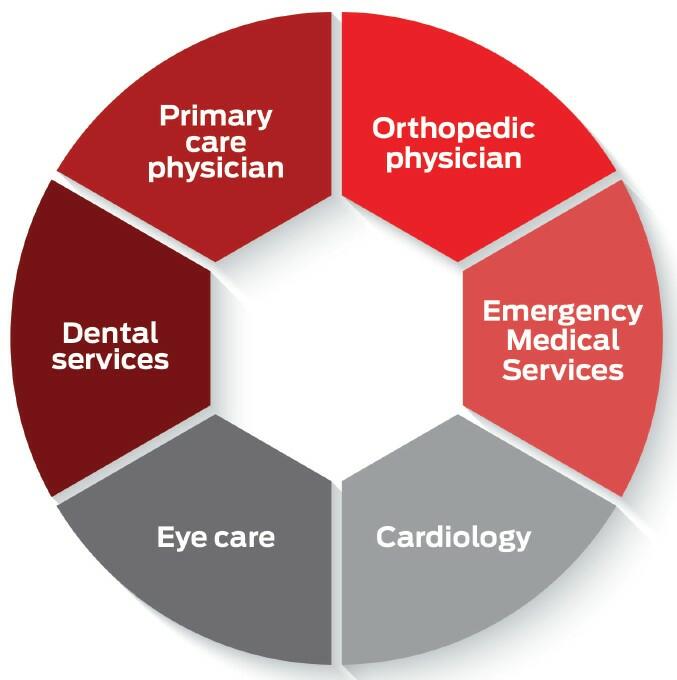
When present the athletic trainer typically serves as the “gatekeeper” to the rest of the healthcare system for the injured or ill athlete. They make initial patient contact and refer the athlete to other healthcare providers as necessary. Such referrals might include primary care physicians, specialty physicians such as orthopedic surgeons, dentists, optometrists, physical therapists, nurses, physician assistants, nurse practitioners, and certainly EMS and/or emergency room providers for conditions deemed emergent. This model allows for timely and collaborative patient care.
Figure 1 shows an example of this model. This model of sports medicine care is widely regarded as the gold standard, as the athletic trainer has the ability to develop rapport with athletes, as well as other members of the sports medicine team. Unfortunately, current data shows only 35% percent of secondary schools in the U.S. have access to the services of an athletic trainer on a full-time basis,4 and 34% of secondary schools have no athletic training services at all.4 In places with limited or no athletic training coverage, the EMS provider may be the first healthcare provider to contact the athlete/patient. It is important for EMS providers and agencies to recognize if they serve a school district where this is the case, as this should trigger additional discussions with school administrators prior to any emergency occurring.
Collaboration in Care
The goal of any sports medicine team is to ensure that injured or ill athletes receive the most appropriate care in the timeliest fashion. Obviously, this is especially critical with time-sensitive injuries and illnesses.
Consider the scenario of an EMS crew providing event standby for a Friday night high school football game. As a play ends, a player is noted lying facedown near the 50-yard line. Someone from the sidelines, possibly an athletic trainer, has already started out on the field, and after a few seconds at the athlete’s side, he looks in the direction of the ambulance and starts waving.
If no communication took place prior to the game, it might be unclear if this is a signal to respond to the field. Is the person waving an athletic trainer, a physician, or even any sort of healthcare professional? Is it acceptable at this venue to drive out onto the field? What equipment is needed, and are you providing that, or is it coming from the sidelines? What will be your best egress route from the facility once transport is initiated? These are just some of questions that might arise if they aren’t sorted out in advance.
Even more concerning in these types of scenarios is when members of the sports medicine team have differing views on how to provide emergent care. Standing over this injured athlete at the 50-yard line is hardly the time or place to sort out these differences.
In situations like this the keys to successful patient outcomes are preplanning and good communications among members of the sports medicine team. Two ways in which this can be facilitated are emergency action plan development and the pre-event medical time-out.
Emergency Action Planning in Athletics
Just as municipalities commonly utilize all-hazards approaches to preparing for potential emergencies, the same should occur in the world of sports. The emergency action plan (EAP) in athletics provides a framework to get the right people with the right equipment in the right place at the right time. The National Athletic Trainers’ Association’s position statement on emergency action planning in athletics recommends this written plan include the following:5
- A description of personnel who might be involved in a response;
- Communications specifics such as who will be summoned and how;
- A description of available and/or potentially needed emergency equipment (e.g., AED or spine board), its location, and its maintenance and training plans;
- Access and egress routes responders might use for each facility;
- Aeromedical landing zones and their coordinates at or near the athletics venue;
- Locations of hospitals and the closest trauma center;
- Directions to each athletics venue, including any gates or doors needing unlocked and who will be able to do that in a timely fashion;
- Venue-specific information—for example, a high school or college campus will often have multiple fields, gyms, or other sports venues and specific information for accessing each. Include the emergency equipment available at each.
- Documentation guidelines including who will document, what basic information will be documented, after-action review documentation, and personnel training and equipment maintenance records.
One major advantage when schools employ the services of an athletic trainer is that they will typically take the lead role in developing the EAP. It is important, however, that all stakeholders in emergency response have a seat at that table, and EMS providers should embrace that role. The development of this document is a chance for EMS providers to discuss their needs and concerns with aspects of the venue emergency response.
Once a consensus is reached and a final EAP is produced, distribute it to all stakeholders. An EAP that sits on the shelf at the local high school but isn’t shared with all members of the sports medicine team is really no better than having no plan. In the event a school employs no athletic trainer, it’s advisable for the local EMS agency to reach out to school administration to discuss either developing an EAP or revising what may be an outdated one.
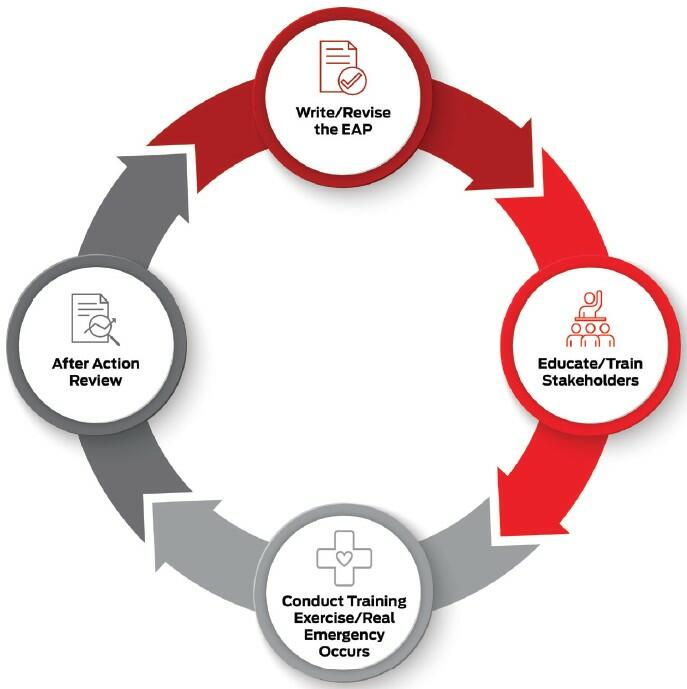
No matter who spearheads the development, an EAP should always be a “living” document. Any time an emergency response occurs, an after-action review should follow, and potential changes to the EAP should be discussed and implemented as necessary. Figure 2 shows what this cyclical process looks like.
It is also important for all members of the sports medicine team to review and rehearse aspects of the EAP on at least an annual basis. One example of this might be to conduct a training exercise posing a simulated emergency response.6 Athletic trainers, physicians, and fire/EMS personnel can assume their typical roles, allowing the EAP to be tested and areas of potential revision identified before the “real deal” occurs. An EMS agency might even consider approaching the local school athletic trainer (or, in their absence, school administration) to discuss working together on planning an athletics emergency training exercise. No matter who leads the exercise, this type of training is another great opportunity for all members of the sports medicine team to build trust and sort out differences.
The Medical Time-Out
In 2012, to further collaboration among members of sports medicine teams, NATA introduced the concept of holding a medical time-out prior to athletic events.7 The larger medical community, especially surgical services, has widely used this concept as a means of ensuring the right procedures are done on the right patients—it aims to prevent errors such as replacing a patient’s left knee when in fact they came in for a right knee replacement!
The use of the medical time-out in athletics is really geared toward improving communication and collaboration among all those at a venue who might be involved in responding to an emergency. This might include athletic trainers and team physicians from both teams, school administrators, sports officials, EMS crews staging at the venue, law enforcement or security personnel, and anyone else deemed pertinent.
This time-out should occur as a face-to-face meeting shortly before the start of the event. The following are some things to address:
- Introductions to each other and what each person’s role in a response might be;
- Is the venue EMS crew a dedicated standby unit or a duty crew that may have to leave for other calls?
- Clarification of what communication(s) will be utilized, such as hand signals to notify EMS it’s needed and what the emergency type might be. If radio or cell phone communication is utilized, identifying common frequencies and phone numbers of each team member is important;
- Identification of what emergency equipment is at the venue, its location, and who will bring it onto the field or court;
- Discussion of transportation of injured or ill athletes. Where is the closest trauma center? What are the access and egress routes from the facility? Is there an established aeromedical landing zone at or near the venue, and if so, what are the GPS coordinates?
- Review of any other pertinent aspects of the venue-specific EAP.
Putting It All Together
While emergencies in athletics fortunately don’t happen at every practice or game, they are certainly not rare. When they occur good communication and collaboration from all members of the sports medicine team are critical to the delivery of timely and appropriate patient care.
Quality working relationships take time and effort to build. Working together on the development of solid EAPs, training together on implementing them, holding medical time-outs prior to events, and taking advantage of interacting and communicating at every opportunity will help all members of the sports medicine team grow these relationships. The result will be not only meeting the standard of care for athletic emergency response but lasting partnerships that serve the community well.
Part 2 of this series will discuss the management of acute injuries and conditions.
References
1. Courson R, Goldenberg M, Adams KG, et al. Inter-association consensus statement on best practices for sports medicine management for secondary schools and colleges. J Athl Train, 2014 Jan–Feb; 49(1): 128–37.
2. Centers for Disease Control and Prevention. CDC Heads Up, www.cdc.gov/headsup/index.html.
3. National Athletic Trainers’ Association. Athletic Training, www.nata.org/about/athletic-training.
4. University of Connecticut, Korey Stringer Institute. Athletic Training Services in US Secondary Schools, by State, https://ksi.uconn.edu/wp-content/uploads/sites/1222/2021/02/AT-Services-By-State-Tables-1-4_2019_2020.pdf.
5. Andersen JC, Courson RW, Kleiner DM, McLoda TA. National Athletic Trainers’ Association position statement: Emergency planning in athletics. J Athl Train, 2002 Jan–Mar; 37(1): 99–104.
6. Potter BW, Martin RD. Testing the emergency action plan in athletics. Intl J Athl Therapy Train, 2009; 14(6): 29–32.
7. National Athletic Trainers’ Association. National Athletic Trainers’ Association Official Statement on Athletic Health Care Provider “Time Outs” Before Athletic Events, www.nata.org/sites/default/files/timeout.pdf.
Brian Potter, MS, ATC, NREMT, completed a BS in athletic training at West Virginia Wesleyan College and an MS in health and physical education at Marshall University. After spending 15 years practicing clinical sports medicine, he now works full-time in emergency services education as a specialist with West Virginia Public Service Training.







