



Report: The 2022 FDNY Medical Special Operations Conference

See also:
- Voices of MSOC: Quick Q&As With Top Leaders From the Show
- MSOC: Afternoon Skill Stations
- Bonus Photo Gallery: MSOC 2022
For any EMT, paramedic, or EMS physician who wants to be prepared for any situation, an organization that wants to be on the cutting edge of EMS innovation, or anyone looking for a unique experience and a window into how one of the largest agencies in the country operates, the Fire Department of New York’s Medical Special Operations Conference (MSOC) is a dream come true. Over the course of a weekend and in preconference sessions and a skills competition on Thursday and Friday, attendees of the 2022 conference—held at the FDNY Fire Academy at Randall’s Island and the FDNY EMS Academy at Fort Totten, New York—were treated to informative speakers and engaging hands-on skill sessions that covered all manner of special operations in EMS. MSOC 2022 was the first in 3 years due to the COVID-19 pandemic. The conference is funded in part by the FDNY Foundation and attendee registration.

Attendees took in all MSOC had to offer, learning about a variety of topics and gaining valuable insight from presenters, FDNY EMS personnel, FDNY rescue paramedics, and FDNY special operations firefighters from rescue and squad companies. MSOC isn’t your average EMS conference; as FDNY EMS Chief Lillian Bonsignore said, “This conference is about the people, not the ‘stuff.’ I love it because I’m proud to show off our people’s dedication and knowledge. The experience of MSOC would not be possible without the efforts of people like the conference’s director, Dr. Doug Isaacs, the expertise of the presenters and instructors, and the enthusiasm of the participants.”
The big takeaways from MSOC were to make sure to prepare in the right way; to collaborate among fire, EMS, and law enforcement; and to always strive for improvement and research-based innovation.

When discussing training, nearly every presenter emphasized the importance of preparing realistically, especially for low-frequency but high-stress situations. Collaboration is crucial to provide what Isaacs called “good medicine in bad places.” Whether it’s joint operations between EMS and fire, lessons learned from the military, teamwork between BLS and ALS providers, or even FDNY fire and EMS working together to make MSOC possible, “things only work smoother when people are on the same page” said FDNY Battalion Chief Joseph Downey.
When it comes to change, innovation was on display, from successful programs like FDNY’s rescue paramedics to new technologies such as using drones and robots for EMS and fire and new techniques such as prehospital whole blood transfusion and new ways of thinking about mass-casualty incidents.
MSOC also highlighted the need for EMS to change its mind-set from “stage and wait” to getting involved in the rescue process with good proactive and appropriate medical practices. As Bonsignore told attendees, “When you show up, change happens. When you show up, things get better.”
Opening Ceremonies
The conference began with the FDNY EMS color guard and Pipes and Drums Band presenting colors and an FDNY EMT singing the national anthem.
The master of ceremonies was FDNY EMS Capt. Jordan Lucks. He introduced each of the following speakers who made some brief remarks:
FDNY EMS Chief Lillian Bonsignore: “I love this conference because I’m proud to show off our people’s dedication. This conference is about the people, not the ‘stuff.’ There are no obstacles we are not willing to take on. Over the last 2½ years, FDNY EMS has run toward the pandemic, not away. Thank you on behalf of the patients you’ve treated and people who can return to their families better than you found them. When you show up, things get better. It is appropriate that this is the start of EMS Week, and like all of EMS, FDNY EMS rises to the challenge.”
FDNY EMS Assistant Chief Jonathan Pistilli: “This is truly an international conference, with 26 states and 5 countries represented in attendance.”
FDNY Commissioner Laura Kavanagh: “Unlike many other first responders, EMS does most of their work where the public doesn’t see them, keeping people alive in extraordinary circumstances.”
Assistant Chief John Esposito, Special Operations Command chief, FDNY: “The training you do has to be as realistic as possible. Here at ‘the Rock’ [FDNY Academy], we have planes, trains, automobiles, ships, subways, and supermarkets. Train like you are going to have to play someday.”
Glenn Asaeda, MD, FDNY chief medical director: “This is the first MSOC conference in 3 years because of COVID. Special operations don’t take a break because of the pandemic.”

Lectures Overview and Takeaways
Saturday morning there were lectures from 6 different speakers that covered a variety of topics in medical special operations with expertise from various backgrounds.
The first speaker was Battalion Chief Joseph Downey, an accomplished and tenured leader with the FDNY and FEMA Urban Search and Rescue (USAR) system. Downey reinforced Asaeda’s opening remarks by discussing the impact of the COVID-19 pandemic on USAR actions and the lessons learned. He described how it was challenging to maintain training during the pandemic and how teams managed COVID-19 precautions and outbreaks during deployment to disaster areas. Downey stressed the importance of being prepared and having multiple options and backup plans, such as pretesting for teams, using limited resources (such as PPE) effectively through planning, thinking about extended-operations concerns such as housing and meals, and planning for team role redundancies if a COVID outbreak sidelines members.
The second speaker was Trevor Glass, who has extensive experience working in medical special operations around the world with the United Nations and as the owner and managing director of DART Solutions, a UK-based company that specializes in disaster and emergency management services. Glass focused on confined- and restricted-space medicine.
Glass defined confined space as an area like a ship’s hold or a basement. He referred to restricted space as an area where movement and space are severely limited. He discussed the processes and complications associated with situations where entrance and exit, atmosphere, and patient access are restricted. He shared how confined- and restricted-space situations are different from what most providers are used to, requiring adjustments to how they think and plan, like a focus on entering with less equipment, more hands-on assessment using the senses, and attentive monitoring of both the patient and the environment, including temperature, elements, and oxygen levels. Glass recommended that for restricted-space rescues, EMS downsize its gear—take a small rapid pack, not a large jump bag and lots of tools.
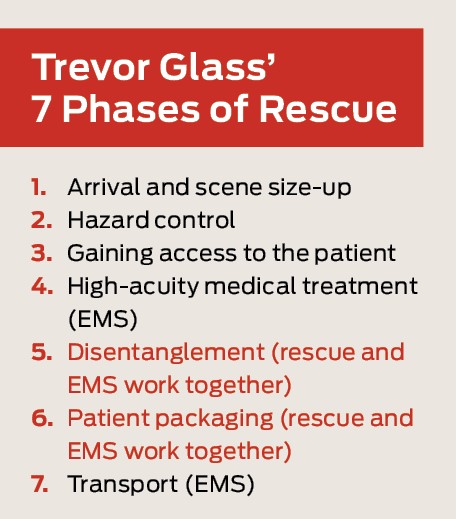
Further, he emphasized the importance of early pain control and patient temperature control for hyper- and hypothermia. “Elements and environment are the influencer here,” Glass said. “You may need to manage a patient for multiple hours.” He also emphasized that effective patient care and rescue do not happen in isolation. “Don’t let a good rescue get in the way of good patient care,” he said. Rescue and EMS need to be working together during stages 5 and 6 of his “7 stages of rescue.” Echoing other presenters, Glass also highlighted that for low-frequency, high-risk, and high-intensity situations like rescues in confined and restricted spaces, realistic training is key, leaving audience members with the adage, “If you can’t do it at home, don’t do it in a disaster.”
The third speaker, Robert Shabbick, discussed the unique operational and medical challenges of responding to a tunnel collapse, drawing from 35 years of experience in EMS and mine rescue in Pennsylvania. He described responses to explosions, collapses, fires, and other underground situations with the Pennsylvania Special Medical Response Team. In these situations monitoring the environment as well as the patient is crucial. In unstable incidents like a rescue underground, rescuers can easily become patients, so safety officers, appropriate PPE, and coordinated communication are paramount.

LTC Stephen Rush drew on his experiences with US Air Force pararescue to discuss both prolonged field care and prehospital response to multiple-casualty incidents (MCIs). Describing prolonged field care as “anything you haven’t planned for and don’t have the resources for,” he explained the lessons learned from his experiences, from making sure all team members were hydrated, fed, and on stable work/rest cycles to keeping a large whiteboard around to draw out plans and using the HITMAN (hydration, infection, tubes, medications, analgesia, nutrition) mnemonic for prolonged care incidents. Mirroring other presenters, Rush emphasized training how you work to “learn the choreography” of an incident, giving examples of both successful and unsuccessful simulations.
When he moved on to talking about MCIs, Rush proposed that the way most EMS providers are taught to handle large incidents with many patients is inefficient and can be improved. He noted research that showed typical START triage is often inaccurate. Instead of relying on algorithms and categories for triage, he suggested classifying patients as stable, unstable, or dead, based on Glasgow Coma Score or rpm: respirations, pulse, and mental status, then moving patients as quickly as possible. Immediate bleeding control for life-threatening hemorrhage should be the only skill used in the field before a patient is moved for transport, with the priority on moving patients as you find them to begin rapid treatment and transport to a surgeon. He cited several combat studies by the US military to support this approach.
The fifth presentation was from CJ Winckler, MD, and Lt. William Bullock from the San Antonio Fire Department, who explained their program of prehospital whole blood transfusions. The program, which began in 2018, borrowed innovations from the military and drew on research that whole blood is more effective for patients, and it has been very successful. According to Winckler and Bullock, more than 900 units of blood have been transfused for both medical and trauma patients. They advocated for similar programs in other locales, even urban areas, as the sooner patients can get blood, the better.

The last presentation of the morning came from Capt. Michael Leo and Chief Robert Delagi, who explained the FDNY robotics program and current and potential uses for unmanned flying drones in EMS. The goal of robotics in fire and EMS is to improve safety, speed, and efficiency. Using drones in an unstable incident can help get EMS out of the “stage and wait” ideology by allowing scene surveys from the air to identify patients and hazards and allow providers to act sooner. Drones can also deliver time-sensitive therapies and equipment. The robotics unit is starting to work with robotic search and rescue dogs as well.
While the department's use of drones is still in its early stages, Leo and Delagi were hopeful these capabilities will be useful for EMS soon.
Barry A. Bachenheimer, EdD, NREMT-FF, has over 36 years of experience in EMS, fire, and rescue in ALS and BLS capacities. He is also a college professor and EMS and fire instructor. He is a frequent contributor to EMS World.
Lea “LJ” Bachenheimer, NREMT, has over 6 years of experience in EMS. She is a student at the University of Wisconsin majoring in sociology/public policy with a health care focus.








