

A First Report of an Active Fixation Leadless Pacemaker in a Patient Post Orthotopic Heart Transplant
Traditional transvenous pacemaker implantation is associated with long-term complications associated with transvenous leads, including risk of infection, malfunction, and potential risk of transvenous lead extraction.1 This is particularly true in younger patients who have a higher risk of these complications over their lifetime secondary to both duration and physical activity. This is reflective in the recently updated guidelines for implantable device implantation when compared to guidelines in adults.2
Symptomatic bradycardia from long sinus pauses associated with syncope is an albeit infrequent but accepted indication for pacemaker implantation.3 Given the infrequent need for pacing in this population, leadless pacemakers have been demonstrated to be safe and effective in this population.4 However, the ideal strategy for the long-term management of these devices in this population is not well established, as the potential for device retrieval and replacement might be an ongoing concern.
Patients with orthotopic heart transplantation (OHT) may experience bradycardia related to acute or chronic rejection as well as the consequences of a denervated and potentially ischemic heart.5 Pacemaker implantation is indicated in this population with severe symptomatic bradycardia.2,5 Leadless pacemaker implantation may provide an ideal form of pacing in this population if it is infrequently required, but considerations for long-term retrievability and the need for atrial-based pacing need to be considered. We present a case that, to our knowledge, is the first patient status post (s/p) OHT implanted with an active fixation leadless pacemaker.
Case Presentation
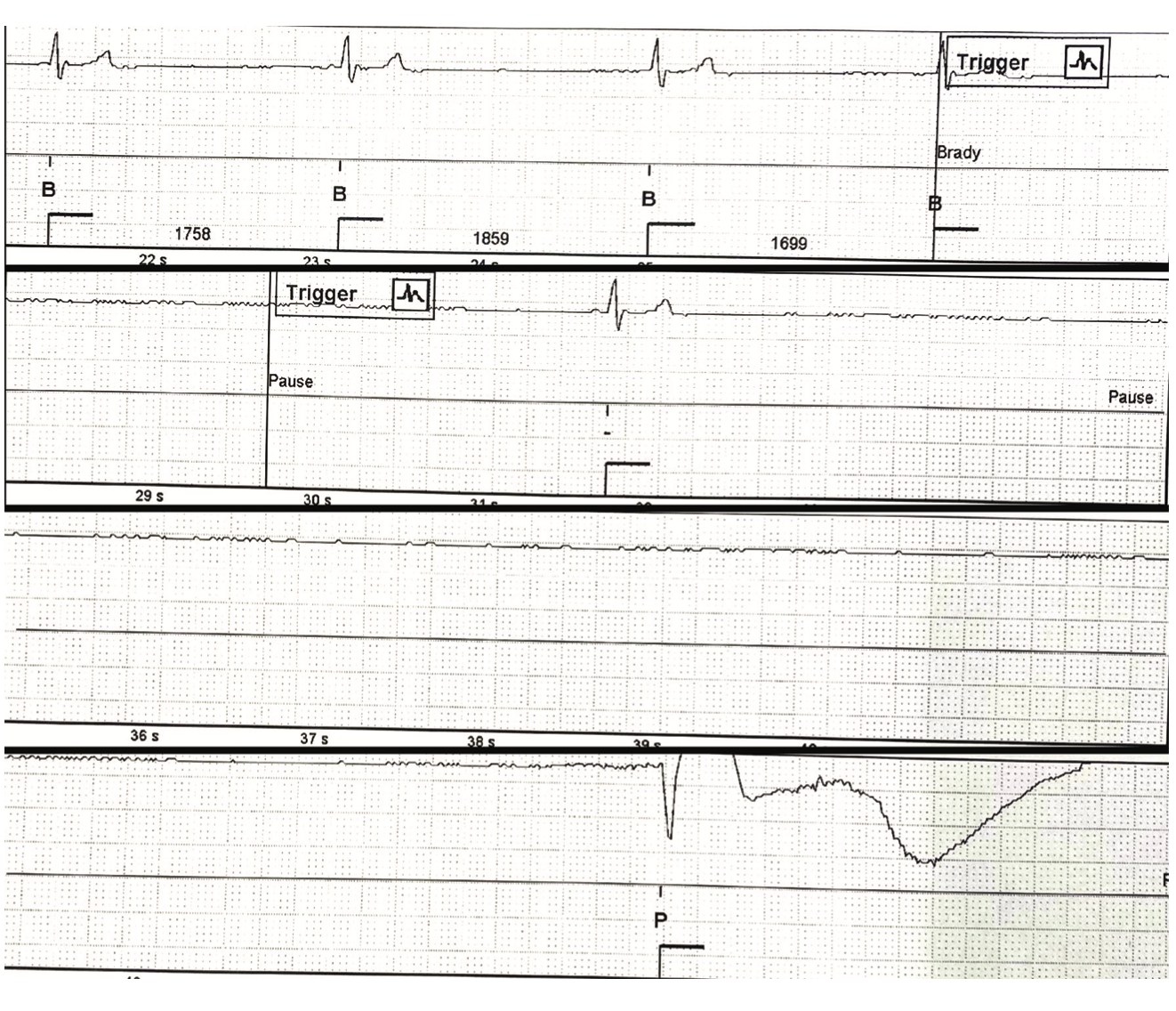
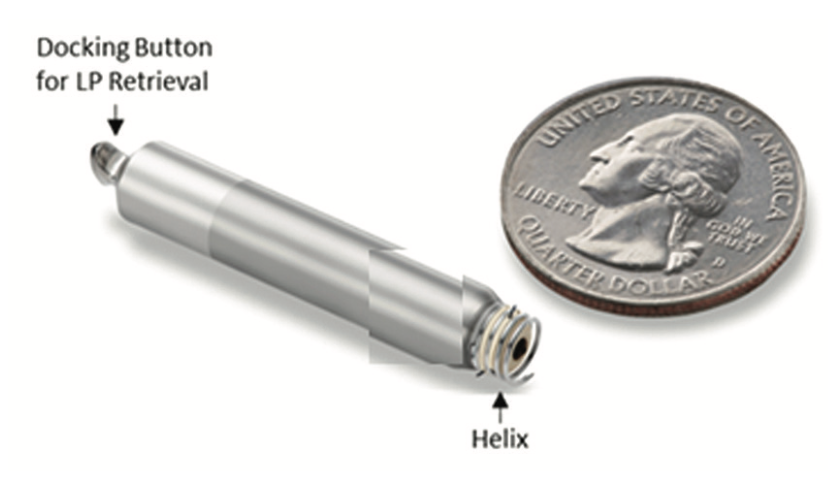
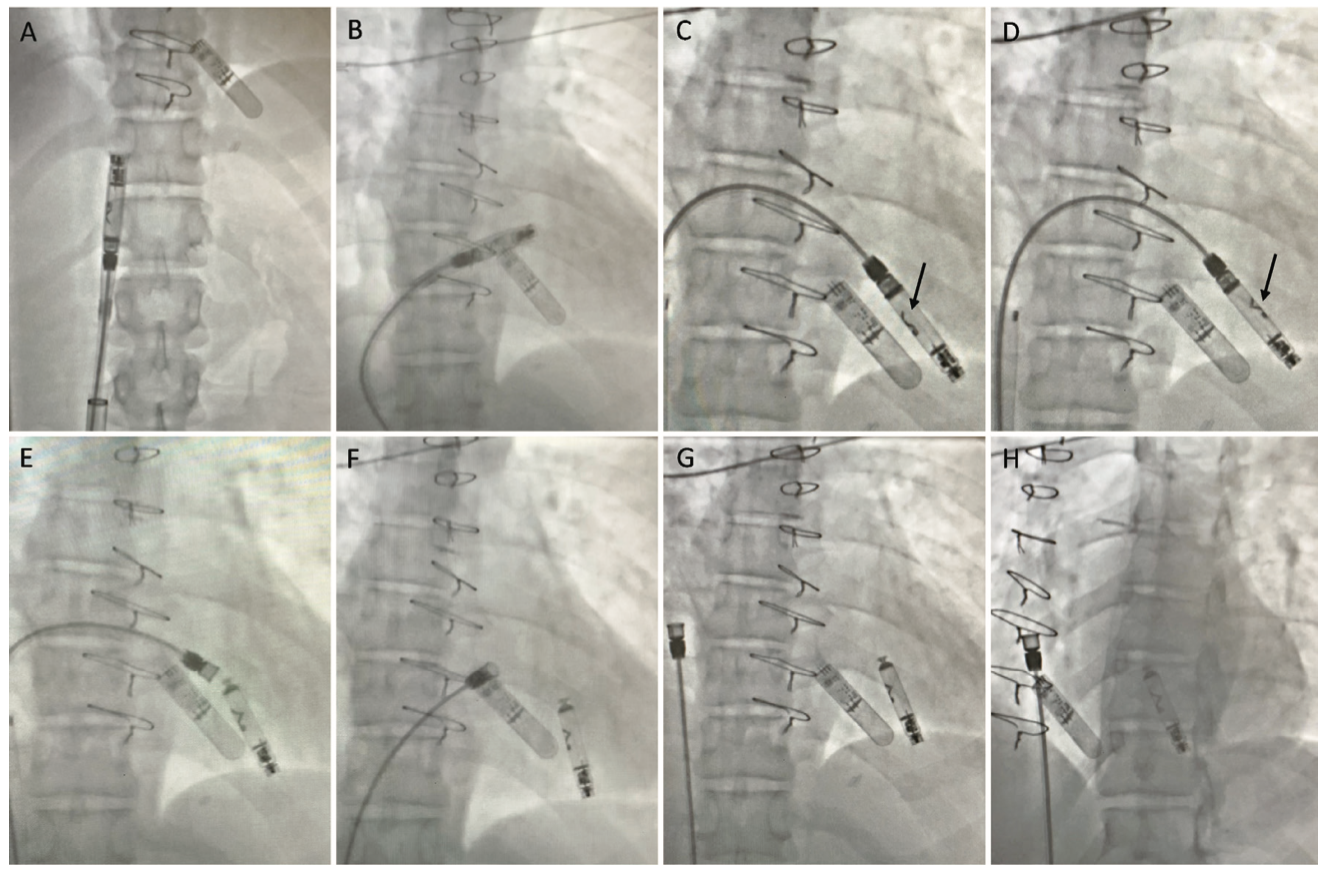
We present a case of a 39-year-old female with a past medical history of arrhythmogenic right ventricular cardiomyopathy, history of implantable cardioverter-defibrillator implantation with multiple shocks for ventricular tachycardia subsequent s/p OHT and subsequent redo OHT 14 years prior, who presented to the outpatient clinic for referral of presyncope. Of note, since transplant, the patient has done well from a heart failure standpoint. She is noted to be intolerant to tacrolimus with alopecia. She had a history of Class 1B rejection successfully treated with intravenous immunoglobulin, rituximab, and photopheresis twice (last treatment 6 years ago). She was recently noted to have Stage 4 chronic kidney disease (CKD) and underwent workup for renal transplant 1 year prior to presentation, but had subsequent improvement to Stage 2 CKD with plasmapheresis and medical management. The patient has remained very active in sports and shows adequate chronotropic competence. However, she was recently noted to have sporadic palpitations and presyncopal symptoms. An implantable loop recorder (ILR) was implanted and confirmed symptoms correlating with prolonged sinus pauses, with multiple pauses >10 seconds while awake and associated with near syncope (Figure 1). Given anticipated low pacing burden requirement, a desire to preserve venous vasculature given her young age, and recent renal dysfunction with concern for possible progression to renal failure, a shared decision to proceed with leadless pacemaker implantation was made. She underwent successful implantation of an active fixation Aveir leadless pacemaker (Abbott) in the right ventricle (RV) (Figure 2) as part of the LEADLESS II IDE trial. Device deployment was performed under fluoroscopic guidance (Figure 3). Acute implantation thresholds were noted to be 1.0V, sensed R-waves = 3 mV, impedance = 300 ohms with subsequent threshold increase to 2.25V approximately 10 minutes after deployment. Device was programmed to VVI 40 bpm, RV capture 5.0V @ 1.5 ms, 730 ohm impedance noted with 4.5 mV sensed R-wave. Successful hemostasis of the access site with figure-of-8 stitch and manual pressure was obtained.
At her postprocedure check, her threshold had increased to 6V @ 0.4 ms and 4.5 V at 1.5 ms. Given the infrequent pacing need, it was decided to follow conservatively. At 6 weeks, the capture threshold remained unchanged. At 3-month follow-up, she was noted to have minimal pacing burden (1%) with complete resolution of presyncope, and was able to participate in all physical activity without restriction. She continues to do well now more than 1 year postprocedure.
Discussion
To the knowledge of the authors, this is the first case of an active fixation leadless pacemaker in a transplanted heart. The current presentation posed several unique challenges. First, the patient is s/p redo OHT and has the potential for recurrent episodes sequelae of chronic rejection. Second, the patient’s recent renal dysfunction to Stage 4 CKD requiring evaluation for hemodialysis and renal transplantation raised the importance of preservation of venous vasculature. Third, and perhaps most important, given the patient’s young age, the anticipated need for multiple devices during the patient’s lifetime further increases the risk of venous vascular complications with a lead-based pacing system. For this reason, given the need for multiple devices over the patient’s lifetime and small transplanted heart, the additional consideration for a device that was designed to be removable was critical. Furthermore, in the patient with OHT, the long-term risk of atrioventricular block due to rejection remains a concern. The patient had a history of rejection and is intolerant to tacrolimus. If required, the patient could be a candidate for upgrade to a dual-chamber leadless pacing system with the additional placement of an atrial leadless pacemaker in clinical trial or in anticipation of eventual approval.
The smaller than average anatomical size of the transplanted heart necessitated consideration of the location of device implant, factoring in potential retrievability of the pacing system. The implanted leadless pacemaker is designed to be fully retrievable.6 The original Nanostim device system has been demonstrated to have approximately 90% chronic retrievability rate postimplantation.7 The anatomical placement of our device at the RV apex lent itself to a high postimplant RV pacing threshold, which remained an initial concern. However, while relocation of the device to RV basal or mid-septum may have resulted in a lower threshold, several benefits from its current location resulted in us accepting this higher threshold. Maintaining a freely mobile docking portion of the device has been demonstrated to correlate with extractability, and this is less likely to be seen with device deployment further up the septum, as the device may end up getting encapsulated on the basal RV.8 A low anticipated pacing burden (≤1% at 3 months) given the patient’s inherent chronotropic competence allowed for reduced concerns regarding a significant effect on battery longevity.
Leadless pacing has been used in patients with cardioinhibitory syncope. Turagam et al conducted a retrospective multicenter cohort analysis of 72 patients with cardioinhibitory syncope with on average almost 8 episodes per year, who received either a conventional transvenous pacemaker (n = 48) or a leadless pacemaker (n = 24).4 In this series, there were no differences in efficacy or safety when comparing the 2 groups, with both groups resulting in >90% freedom of recurrent events during 1 year of follow-up.
Post-OHT patients often require pacemaker implantation. In their 10-year analysis (1997-2007) of patient outcomes from the UNOS/OPTN database, Cantillon et al found that almost 11% of patients required pacemaker implantation.9 Indeed, patients who received pacemaker implantation were shown to have an excellent prognosis that was better than the nonpacemaker group in this retrospective series. Given the excellent outcomes, pacemaker implantation will likely continue to be a necessary component to the care of this patient population. This illustrates the importance of long-term strategies for device management.
Leadless pacing has been reported in the transplanted population. Rordorf et al report a small series of 7 patients posttransplant.10 Five patients had paroxysmal atrioventricular block, 1 patient had sinus arrest, and 1 patient had postconversion pauses. All patients were implanted with the Micra VR (Medtronic), which is not recommended to be retrieved. Interestingly, the patients on average had 3 ± 3 placement attempts for pacing thresholds, which may reflect the unique injury or inflammatory patterns in the transplanted heart, and could result in higher chronic thresholds, much like we experienced in our patient.
Conclusion
The myriad anatomic, physiologic, and clinical factors in a post-OHT patient and the need for pacing for symptomatic sinus arrest were successfully circumvented with the use of an active fixation leadless pacing system. We were able to address the needs of our patient with good clinical outcomes and anticipated long-term durability, allowing for long-term planning for device replacement and/or upgrade.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Drs Trivedi and Kleinhans have no conflicts of interest to report regarding the content herein. Dr Doshi reports consulting fees and participation on the steering committee for the AVEIR trial.
References
1. Cantillon DJ, Exner DV, Badie N, et al. Complications and health care costs associated with transvenous cardiac pacemakers in a nationwide assessment. JACC Clin Electrophysiol. 2017;3(11):1296-1305. doi:10.1016/j.jacep.2017.05.007
2. Silka MJ, Shah MJ, Silva JNA, et al. 2021 PACES expert consensus statement on the indications and management of cardiovascular implantable electronic devices in pediatric patients: executive summary. Heart Rhythm. 2021;18(11):1925-1950. doi:10.1016/j.hrthm.2021.07.051
3. Kusumoto FM, Schoenfeld MH, Barrett C, et al. 2018 ACC/AHA/HRS guideline on the evaluation and management of patients with bradycardia and cardiac conduction delay: a report of the American College of Cardiology/American Heart Association task force on clinical practice guidelines, and the Heart Rhythm Society. J Am Coll Cardiol. 2019;74(7):932-987. doi:10.1016/j.jacc.2018.10.043
4. Turagam MK, Gopinathannair R, Park PH, et al. Safety and efficacy of leadless pacemaker for cardioinhibitory vasovagal syncope. Heart Rhythm. 2020;17(9):1575-1581. doi:10.1016/j.hrthm.2020.05.006
5. Hamon D, Taleski J, Vaseghi M, Shivkumar K, Boyle NG. Arrhythmias in the heart transplant patient. Arrhythm Electrophysiol Rev. 2014;3(3):149-155.
6. Reddy VY, Exner DV, Cantillon DJ, et al. Percutaneous implantation of an entirely intracardiac leadless pacemaker. N Engl J Med. 2015;373(12):1125-1135. doi:10.1056/NEJMoa1507192
7. Lakkireddy D, Knops R, Atwater B, et al. A worldwide experience of the management of battery failures and chronic device retrieval of the Nanostim leadless pacemaker. Heart Rhythm. 2017;14(12):1756-1763. doi:10.1016/j.hrthm.2017.07.004
8. Minami K, Neužil P, Petrů J, et al. Retrieval of long-term implanted leadless pacemakers: a single-center experience. JACC Clin Electrophysiol. 2020;6(14):1744-1751. doi:10.1016/j.jacep.2020.06.010
9. Cantillon DJ, Tarakji KG, Hu T, et al. Long-term outcomes and clinical predictors for pacemaker-requiring bradyarrhythmias after cardiac transplantation: analysis of the UNOS/OPTN cardiac transplant database. Heart Rhythm. 2010;7(11):1567-1571. doi:10.1016/j.hrthm.2010.06.026
10. Rordorf R, Savastano S, Bontempi L, et al. Leadless pacing in cardiac transplant recipients: primary results of a multicenter case experience. J Electrocardiol. 2020;60:33-35. doi:10.1016/j.jelectrocard.2020.03.010
11. Reddy VY, Exner DV, Doshi R, et al. Primary results on safety and efficacy from the LEADLESS II-Phase 2 Worldwide Clinical Trial. JACC Clin Electrophysiol. 2022;8(1):115-117. doi:10.1016/j.jacep.2021.11.002

