Initial Experience With Zero-Fluoroscopy Pulsed Field Ablation for Atrial Fibrillation: A Case Study and Workflow Analysis
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2024;24(11):24-30.
Hany Demo, MD, FACC, FHRS
Swedish Covenant Hospital, Endeavor Health Medical Group, Chicago, Illinois
Catheter ablation, specifically pulmonary vein isolation (PVI), has become a cornerstone in the treatment of symptomatic, drug-refractory atrial fibrillation (AF). However, the traditional reliance on fluoroscopy for catheter navigation during ablation has raised concerns about cumulative radiation exposure to both patients and health care providers.1-6
A zero-fluoroscopy approach for traditional thermal ablation methods such as radiofrequency (RF) ablation and cryoablation has been increasingly described in the literature and is progressively gaining adoption in clinical practice. The integration of intracardiac echocardiography (ICE) and electroanatomical mapping enables a zero-fluoroscopy approach that reduces radiation exposure while maintaining procedural efficacy and safety.7-12
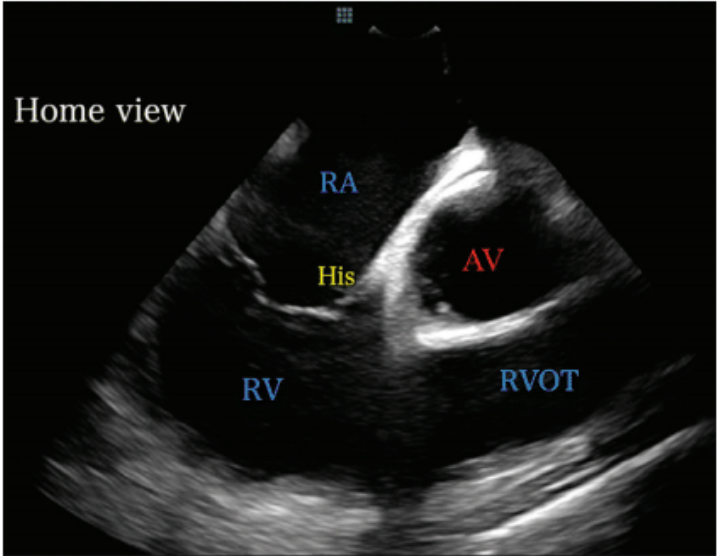
AV=aortic valve; His=bundle of His area; RA=right atrium; RV=right ventricle; RVOT=right ventricular outflow tract.
Pulsed field ablation (PFA) is an emerging non-thermal modality for PVI that promises similar efficacy but a better safety profile,13 particularly when integrated into a zero-fluoroscopy workflow.
This article outlines our initial experience with zero-fluoroscopy PFA for AF, focusing on patient selection, procedural workflow, and practical tips for incorporating this technique into clinical practice. The findings provide insights into the feasibility and effectiveness of zero-fluoroscopy PFA, highlighting key considerations for adopting this innovative approach.
Case Presentation
The case involves a 64-year-old man with paroxysmal AF refractory to multiple antiarrhythmic drugs, including amiodarone and flecainide. The patient had a history of hypertension and was at low risk for stroke (CHA2DS2-VASc score of 1). Given the patient’s symptomatic burden and failure of pharmacological therapy, catheter ablation was recommended. PFA was chosen due to its favorable safety profile, particularly concerning the reduced risk of esophageal and phrenic nerve injury. The decision to perform the procedure without fluoroscopy was based on our experience with ICE and electroanatomical mapping, which we believed would allow for accurate and safe catheter navigation and ablation. The PulseSelect PFA ablation system (Medtronic) was used.
Preprocedural Planning
The patient was scheduled for PFA using a zero-fluoroscopy approach. Preprocedural imaging, including transesophageal echocardiography (TEE) and cardiac magnetic resonance imaging (MRI), was not performed. ICE was used to assess atrial anatomy and rule out left atrial (LA) thrombus. Anticoagulation (apixaban) was held the morning of the procedure.
LA=left atrium.
Vascular Access and Introduction of ICE Catheter
The procedure was performed under deep sedation. Under vascular ultrasound guidance, percutaneous femoral vascular access was obtained using the modified Seldinger technique. A long 10 French (F) sheath, short 10F sheath, and 7F sheath were placed in the right femoral vein. A 9F ICE catheter was advanced through the 10F sheath. The catheter was guided through the left femoral vein up to the right atrium (RA).
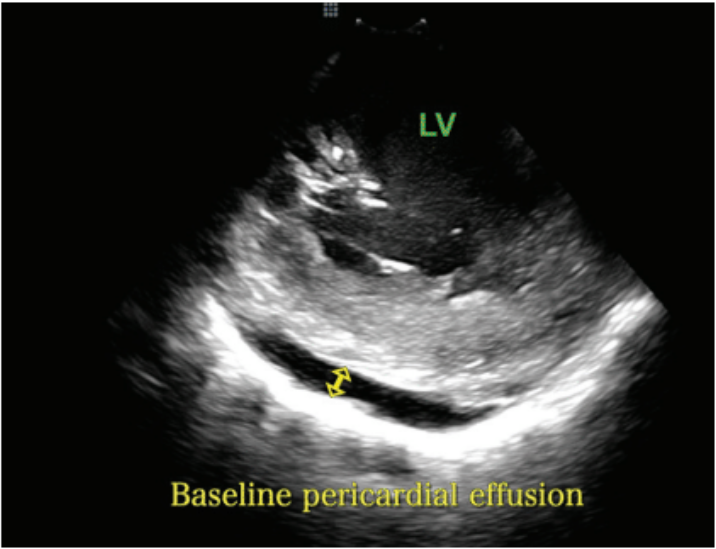
Obtaining Baseline Images
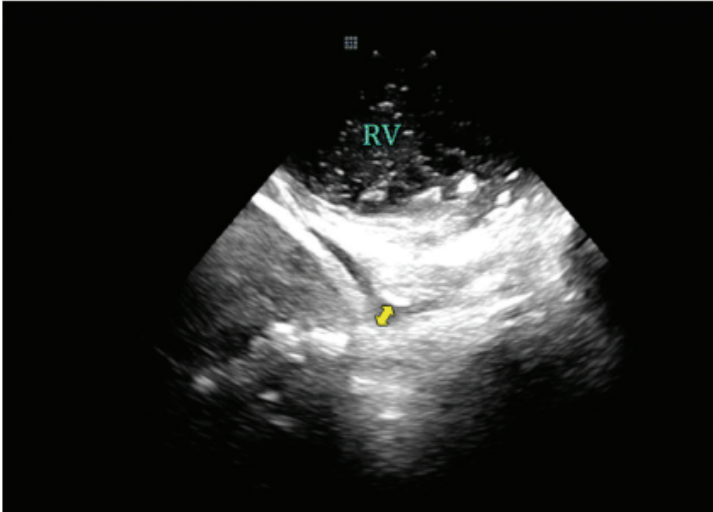
Once in the RA, the ICE catheter was minimally rotated clockwise or counterclockwise until the “home view” was seen. The home view is where the RA, tricuspid valve (TV), right ventricle (RV), and aortic valve (AV) are seen (Figure 1). From this position, an anterior curve was applied to the ICE catheter prior to advancing the ICE catheter across the tricuspid valve and into the RV. Once in the RV, the anterior curve was released and the catheter was used to assess for the presence of any pericardial effusion around the RV (Figure 2). To assess for fluid around the LV, the ICE catheter was rotated clockwise until the LV was in view (Figure 3). These images were stored and served as a useful comparator in the event of hypotension later in the case.
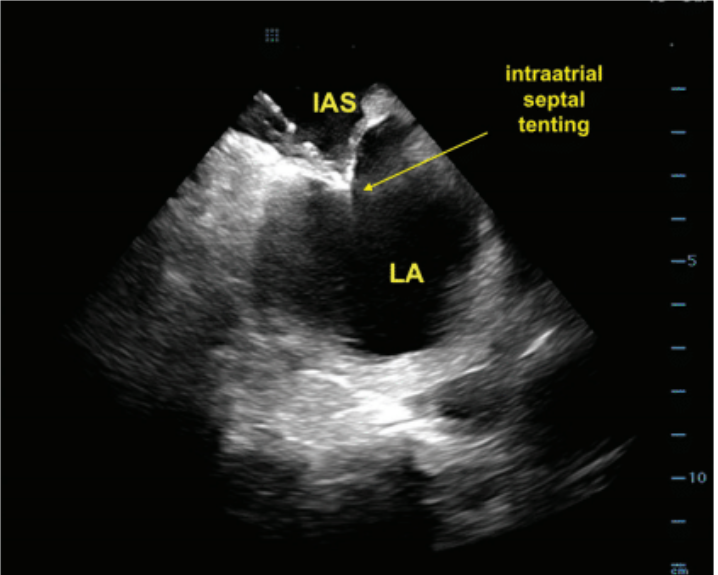
Transseptal Puncture
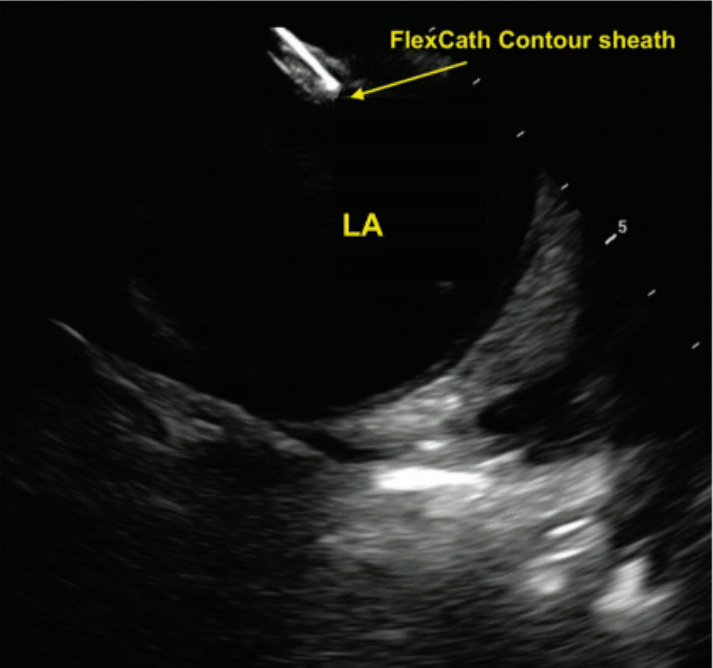
ICE was used to visualize the fossa ovalis and guide the transseptal puncture. A VersaCross RF transseptal wire (Boston Scientific) was used for transseptal access. The wire was advanced to the superior vena cava (SVC) through the short 10F sheath. The short sheath was then removed and a 10F FlexCath Contour sheath (Medtronic) and dilator assembly were advanced over the wire for zero-exchange transseptal access. The puncture was performed with real-time ICE imaging, ensuring accurate puncture without the need for fluoroscopic guidance. The transseptal assembly was withdrawn from the SVC down to the fossa. The sheath was manipulated to achieve tenting of the septum in a satisfactory location (Figure 4). Transseptal puncture was performed by delivering RF energy thorough the RF wire. The transseptal sheath was then advanced into the LA under continuous ICE monitoring (Figure 5).
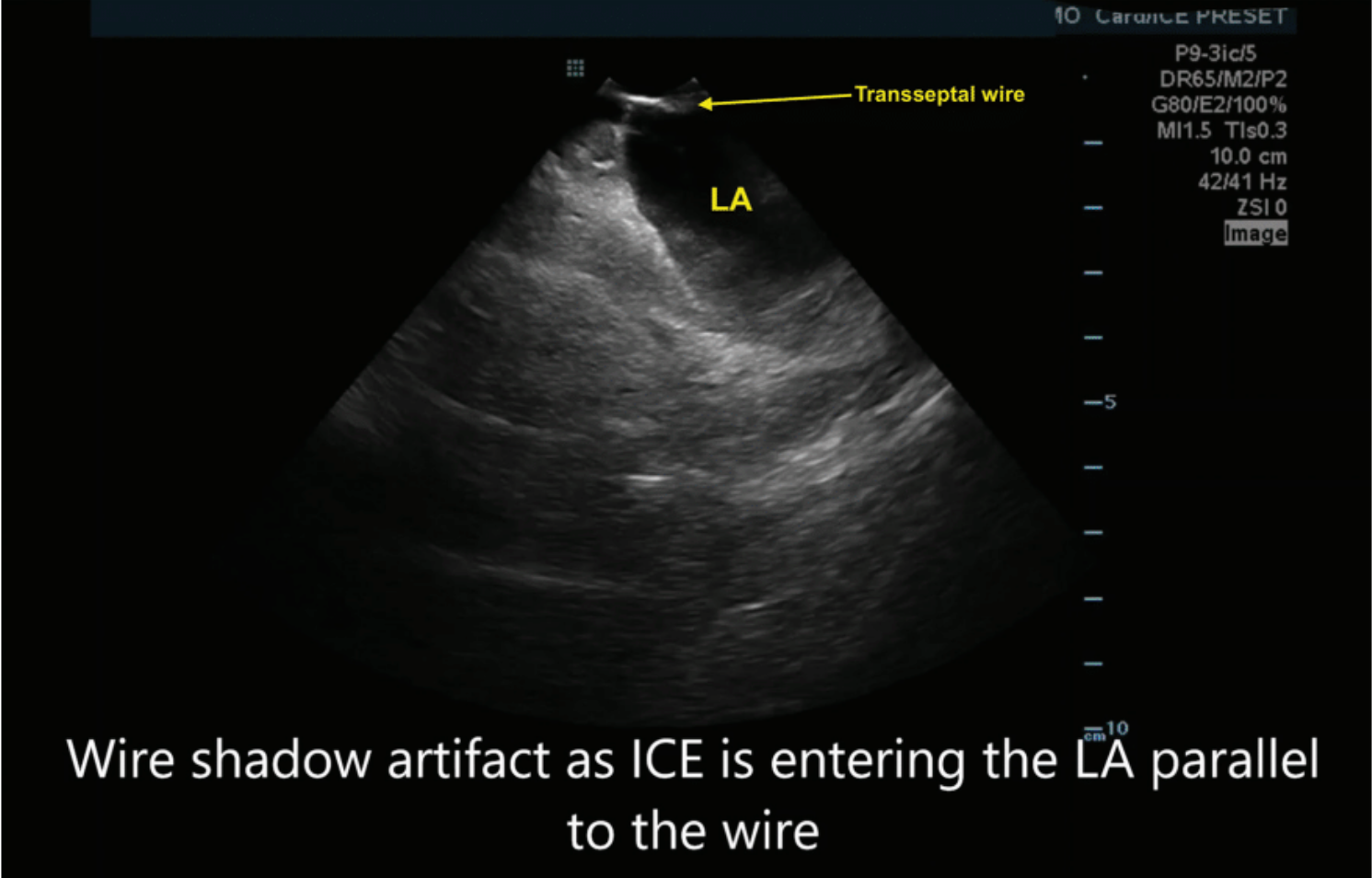
Placing the ICE in the LA
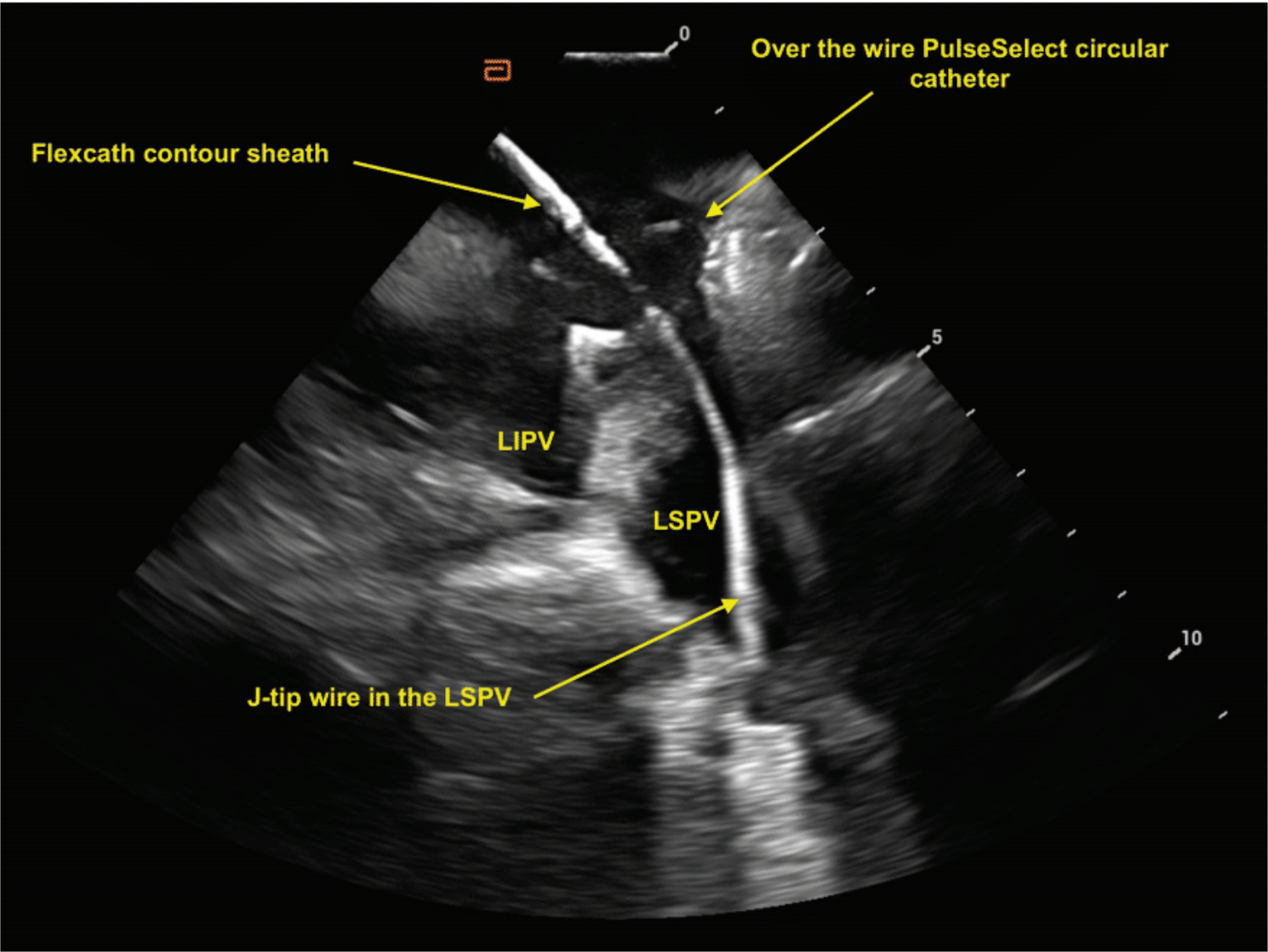
While all 4 PVs could be seen from the RA, excellent visualization of the PVs was obtained when the ICE catheter was advanced into the LA. To achieve this end, the ICE catheter was placed through the hole created by the transseptal puncture. Following transseptal sheath exchange, the pigtail wire was left in the mid LA. The FlexCath Contour-dilator assembly was then pulled back into the RA while keeping the wire in the LA. Next, anterior tilt was placed so that the tip of the ICE catheter approximated the entry point of the wire into the transseptal hole. The ICE catheter was then advanced from the RA to LA next to the wire through the same hole (Figure 6). The FlexCath-dilator assembly was advanced into the LA, and the dilator and wire were then removed. With the ICE catheter in the LA, placing posterior tilt resulted in improved visualization of the left PVs. With the posterior tilt removed, clockwise rotation resulted in visualization of the right-sided PVs.
PFA
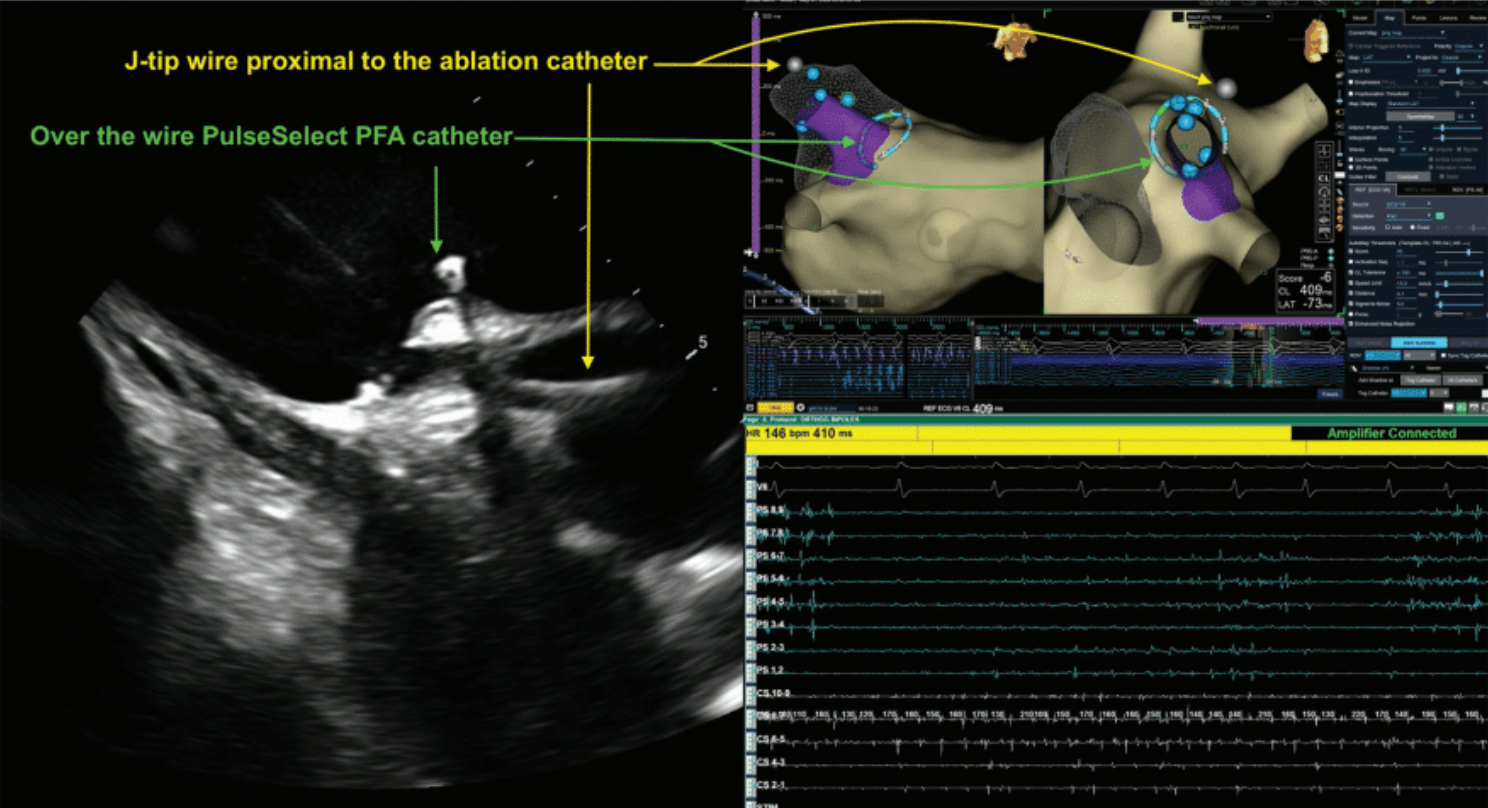
Current first-generation FDA-approved PFA catheters available in the United States are over-the-wire multielectrode catheters that lack tissue contact indicators, which is important for maximizing lesion depth with PFA. The wire must be distal to the PFA catheter and without any contact with the catheter electrodes to avoid any potential arcing during energy delivery. The catheter should be rotated after each successful PFA application to overlap lesion sets and achieve PVI.
©2023 Medtronic. All rights reserved. Used with the permission of Medtronic.
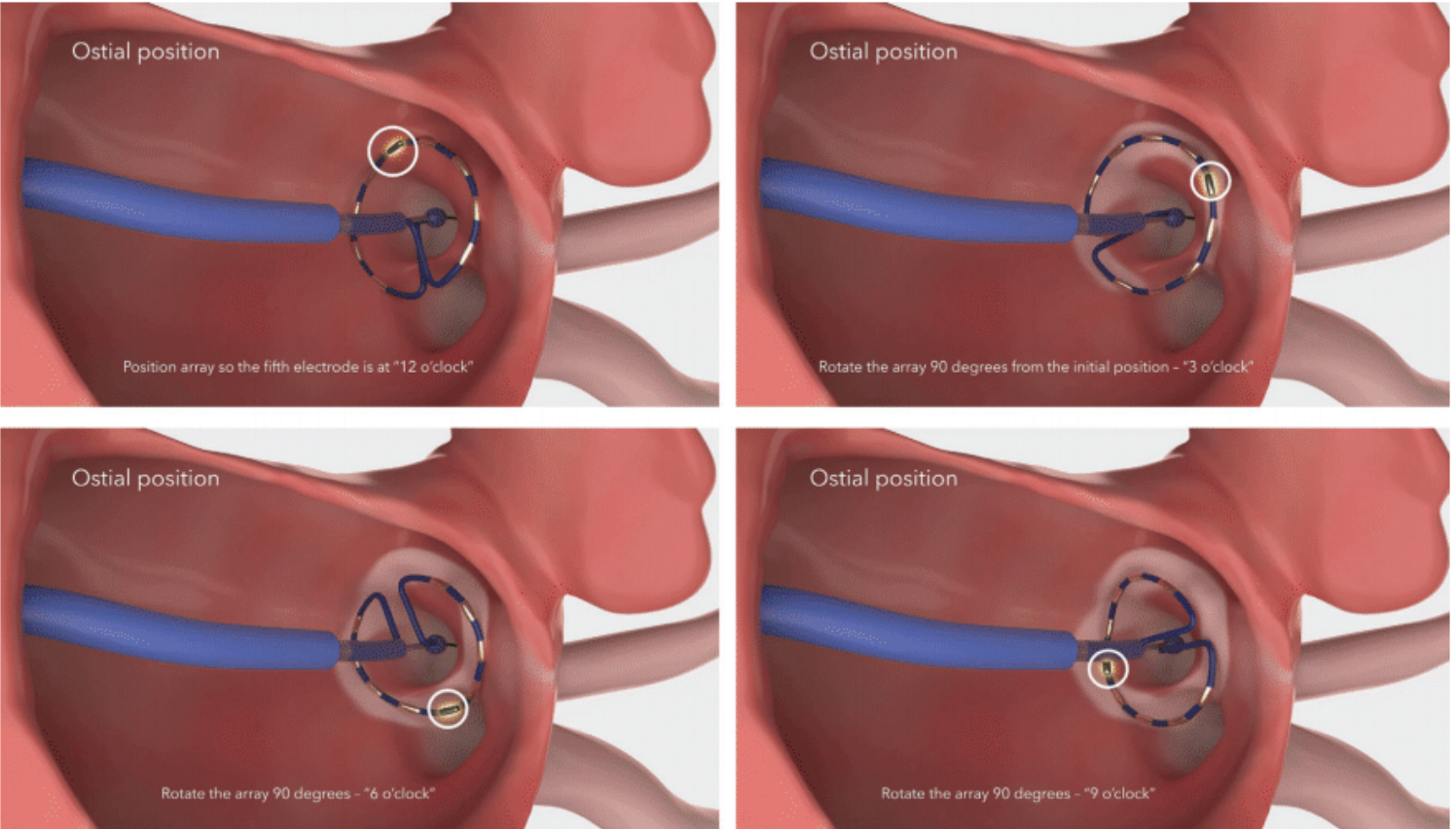
During PFA, the integration of ICE and mapping systems allows for accurate registration of the wire and catheter position within the 3D map, obviating the need for fluoroscopic verification (Figure 7). The map shift is minimal when the coronary sinus catheter is used as a reference for the map. ICE provides real-time, high-resolution visualization of intracardiac structures, enabling precise catheter manipulation and accurate identification of anatomical landmarks. Additionally, the continuous feedback from ICE allows for real-time assessment of adequate catheter contact with the atrial tissue (Figure 8), which is crucial for a successful PFA procedure. The mapping system provides detailed spatial information, enabling the identification and localization of PV ostia, the LA posterior wall, and other critical sites. This spatial precision is crucial in PFA, where lesion sets must be carefully tailored to achieve complete and durable PVI while avoiding gaps that could lead to AF recurrence. The PulseSelect PFA catheter is designed with 20° forward tilted array to ensure contact where the 5th electrode is the first electrode to contact the tissue. Our workflow includes highlighting electrode 5 on our mapping system and tagging it as a lesion once a satisfactory PFA application is delivered. The catheter is then rotated 90° to overlap lesion set and electrode 5 is tagged in its new location. In our stepwise ostial-antral approach, at least 4 ostial and 4 antral applications are applied with electrode 5 tagged at the 12, 3, 6, and 9 o’clock positions in the vein to ensure contiguous PVI (Figure 9).
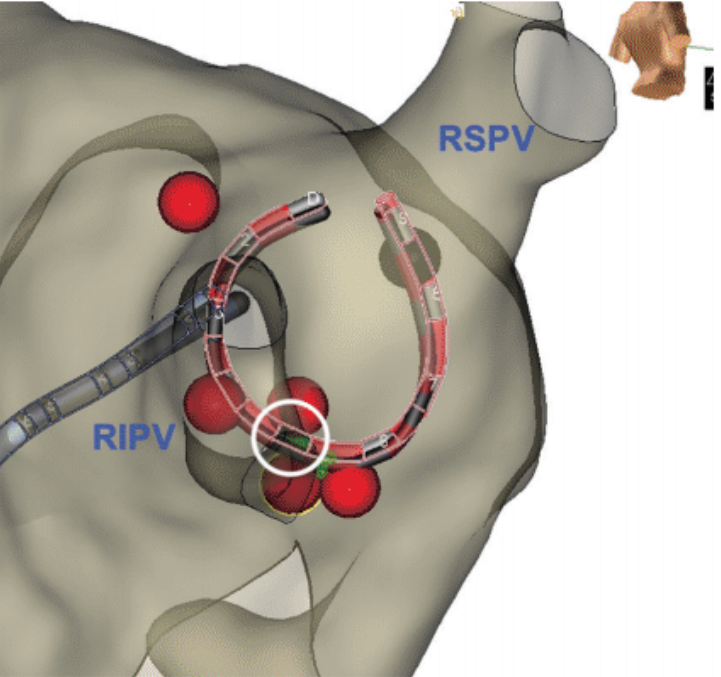
RSPV=right superior pulmonary vein.
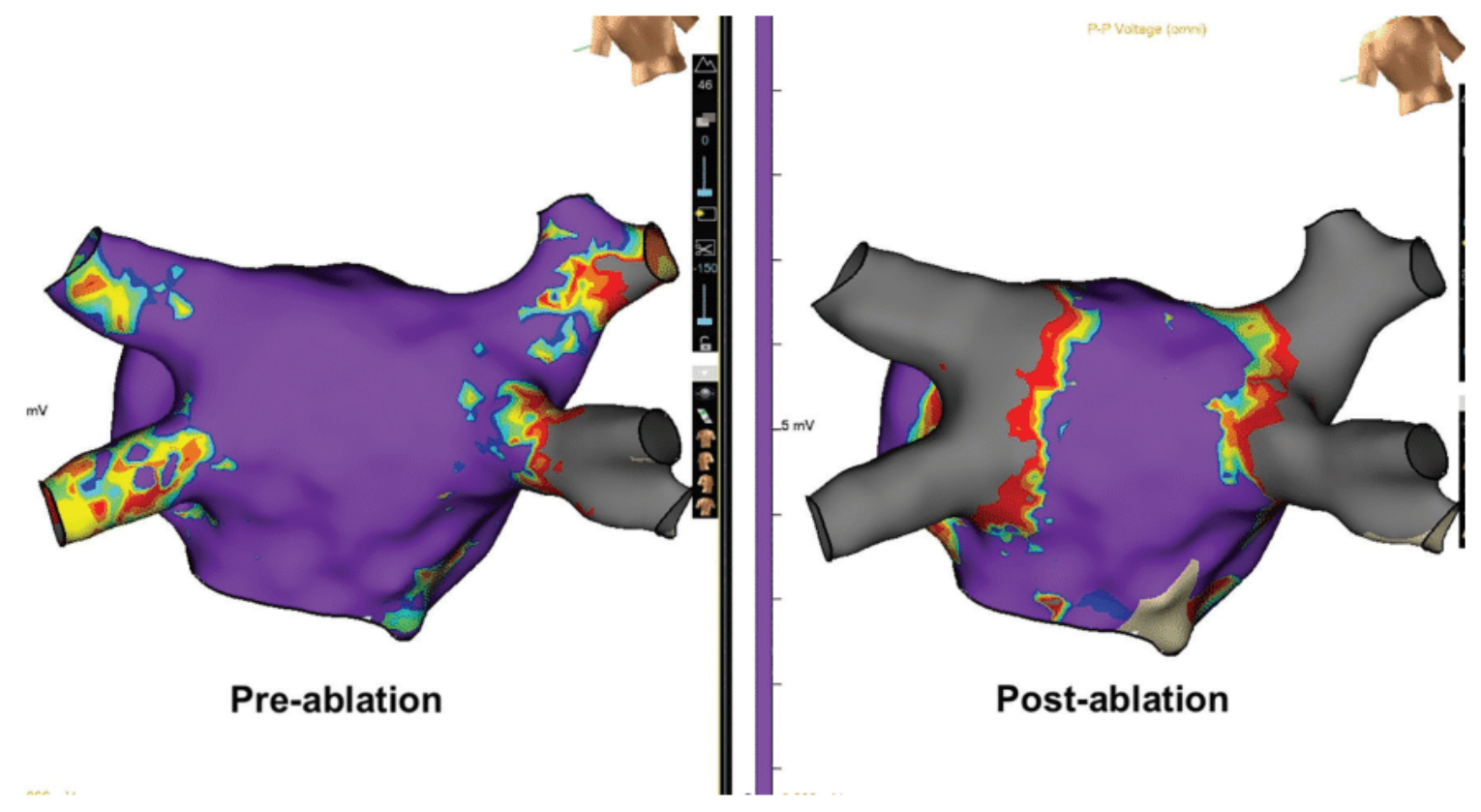
The non-thermal nature of PFA allows for rapid lesion formation with minimal discomfort to the patient. All PVI is confirmed by post-ablation voltage mapping (Figure 10) as well as entrance and exit block testing.
Postprocedural Monitoring
After the ablation, the patient was monitored in the post-anesthesia care unit for 3 hours before being discharged home on continued anticoagulation with instructions for follow-up in 2 weeks. No immediate complications were observed.
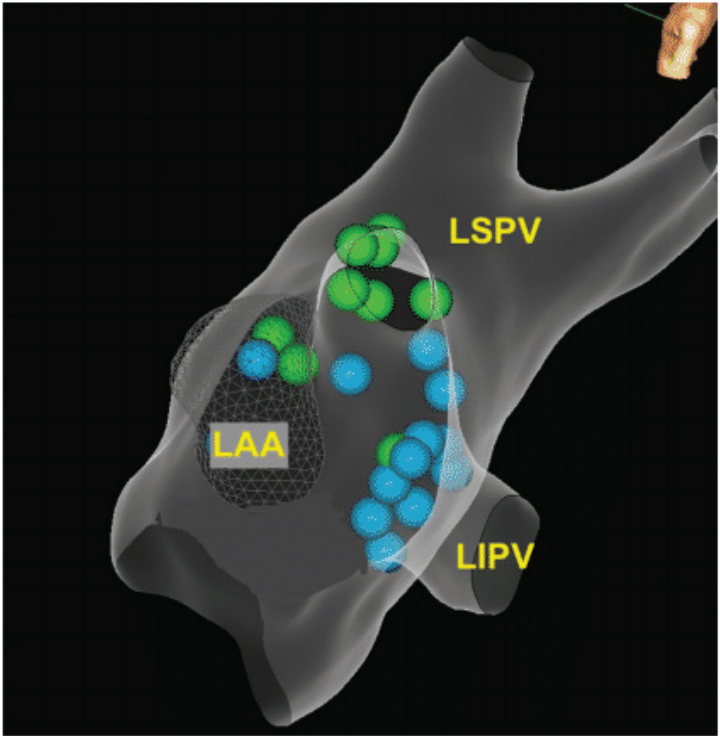
LAA=left atrial appendage.
Discussion
To our knowledge, this is the first report of zero-fluoroscopy ablation using the PulseSelect PFA catheter. Our initial experience with zero-fluoroscopy PFA for AF has been positive, demonstrating that this technique is both feasible and effective when integrated with ICE and advanced electroanatomical mapping. The non-thermal nature of PFA, combined with the radiation-free approach, offers significant advantages in terms of safety and patient outcomes. The learning curve is steep for operators accustomed to fluoroscopy-based techniques, but more manageable for those already experienced with fluoroless methods.
The long-term benefits of adopting this technique make it a valuable addition to the electrophysiologist’s armamentarium. Continued refinement of the procedure and further studies on long-term outcomes will be crucial in defining the role of zero-fluoroscopy PFA in AF management.
While zero-fluoroscopy PFA represents a significant advancement, several challenges must be addressed for widespread adoption. These challenges include the need for precise ICE imaging and interpretation, especially during transseptal puncture, and the reliance on both ICE and electroanatomical mapping for catheter localization. Electrophysiologists must gain proficiency in ICE imaging and become adept in the use of advanced electroanatomical mapping systems to fully realize the potential of this approach. Training programs should emphasize the integration of these technologies, focusing on the understanding of ICE images and the nuances of non-fluoroscopic navigation.
Ongoing technological developments in PFA catheter design and pulse delivery systems are expected to further enhance the efficacy, efficiency, and safety of this approach. Future studies are needed to establish the long-term durability of PFA lesions and to compare clinical outcomes with those of established thermal ablation techniques. As these technologies evolve, zero-fluoroscopy PFA has the potential to become the standard approach for AF ablation, providing a safer and more precise alternative to conventional methods.
Disclosure: Dr Demo has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. He reports consulting fees and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Abbott and Medtronic.
Video
Transcript
In this initial case study, what specific criteria did you use for patient selection for zero-fluoroscopy pulsed field ablation (PFA), and how do these criteria differ from those used in conventional ablation approaches?
The PulseSelect pulsed field ablation catheter (Medtronic) was approved for both paroxysmal and persistent atrial fibrillation (AF). So, selection for the initial cases included both paroxysmal and persistent AF patients. Given the safety profile of the PFA technology for patients with persistent AF, we did posterior wall isolation without worrying about esophageal fistula or rise or reduction in the esophageal temperature and without monitoring the esophageal temperature overall, and that was different than our previous practices. Whenever we isolate the posterior wall, we always worry about esophageal injury.
In your initial experience with zero-fluoroscopy PFA, what specific challenges did you encounter, and how did you address them?
PulseSelect is an over-the-wire catheter and the wire has to be more distal to the catheter to prevent any arcing with the PulseSelect catheter itself. It is an .032” wire. We connected this wire to our mapping system to visualize the wire on the mapping system, since we are not using fluoroscopy to make sure that the wire is more distal to the catheter. So, we connected to the mapping system and the wire was presented as a dot on the mapping system. We always made sure that the wire was distal to the catheter to prevent arcing. Also, we utilized intracardiac echocardiography (ICE) to ensure contact. We know contact is very important for PFA ablations and ICE helps significantly to ensure contact.
What are your thoughts on the future of zero-fluoroscopy PFA in the treatment of AF, and what additional research do you think is needed to establish its long-term efficacy and safety?
Zero-fluoroscopy PFA is safe and durable. It reaches the same efficacy as you would use fluoroscopy with the PFA, and that has been proven. There are more and more publications now about zero-fluoroscopy PFA using the different PFA systems, including the PulseSelect system or the systems from Boston Scientific and Johnson & Johnson MedTech. With all these PFA catheters, there are case reports and studies with zero fluoroscopy. In terms of the long-term efficacy, I think what we are learning over time is that PFA as a technology is different than thermal ablation. It is safer for the things that we know. It is safer for phrenic nerve injury, with zero reports of phrenic nerve injury, pulmonary vein stenosis, and esophageal injury. Those are the things we used to worry about during thermal ablations. But there are also new things that we are paying more attention to with PFA that we need more research on, specifically, hemolysis for example. With radiofrequency, we never used to worry about hemolysis, the rise in creatinine, the rise in LDH, or the reduction of haptoglobin. That was not on our radar at all. But this is now something that we are all looking deeper and deeper into. Is it catheter specific? Is it technology specific? We need to know more about it. So, there is definitely room for a lot of research in that regards.
Also, there are reports of coronary spasm that took place with PFA ablation. Again, not all PFA catheters are created equally. In my experience with the PulseSelect catheter, that has not been the case. As of right now, it is not reported, but we need to know more about that. So, I think in these areas, we need more data and research.
Regarding durability for posterior wall isolation or extrapulmonary vein isolation, a study was presented at APHRS last month on short-term durability (about 30 to 60 days). Patients had an initial PFA ablation, and 30 to 60 days later they went back for a Watchman (Boston Scientific). They remapped the pulmonary veins and found the durability to be 98%. So, we need to make sure this is reproducible and we need to know if that is also the case with posterior wall isolation.
Is there anything else that you’d like to add?
Over the past few years, zero fluoroscopy has taken off and more and more operators are doing zero fluoroscopy. PFA is not much different. If anything, it is the same workflow, it is just a different sheath and a different catheter. As a matter of fact, to do PFA with zero fluoroscopy is easier than cryo, because with PFA, we just need to ensure contact of the catheter with the atrial tissue. Whereas with fluoroscopy, we need to make sure that the balloon is sealed with the vein, we have to use color Doppler, and we have to use other measures. But with PFA, all we need to know is there is contact with the tissue. So, I think if someone had already done zero-fluoroscopy RF ablation or cryoablation, I think the same thing can be applied for PFA.
The transcripts have been edited for clarity and length.
References
1. Vano E, Arranz L, Sastre JM, et al. Dosimetric and radiation protection considerations based on some cases of patient skin injuries in interventional cardiology. Br J Radiol. 1998;71(845):510-516. doi:10.1259/bjr.71.845.9691896
2. Kovoor P, Ricciardello M, Collins L, Uther JB, Ross DL. Risk to patients from radiation associated with radiofrequency ablation for supraventricular tachycardia. Circulation. 1998;98(15):1534-1540. doi:10.1161/01.cir.98.15.1534
3. Calkins H, Niklason L, Sousa J, et al. Radiation exposure during radiofrequency catheter ablation of accessory atrioventricular connections. Circulation. 1991;84(6):2376-2382. doi:10.1161/01.cir.84.6.2376
4. Rehani MM, Ortiz-Lopez P. Radiation effects in fluoroscopically guided cardiac interventions: keeping them under control. Int J Cardiol. 2006;109(2):147-151. doi:10.1016/j.ijcard.2005.06.015
5. Park TH, Eichling JO, Schechtman KB, et al. Risk of radiation induced skin injuries from arrhythmia ablation procedures. Pacing Clin Electrophysiol. 1996;19(9):1363-1369. doi:10.1111/j.1540-8159.1996.tb04216.x
6. McFadden SL, Mooney RB, Shepherd PH. X-ray dose and associated risks from radiofrequency catheter ablation procedures. Br J Radiol. 2002;75(891):253-265. doi:10.1259/bjr.75.891.750253
7. Razminia M, Willoughby MC, Demo H, et al. Fluoroless catheter ablation of cardiac arrhythmias: a 5-year experience. Pacing Clin Electrophysiol. 2017;40(4):425-433. doi:10.1111/pace.13038
8. Razminia M, Zei PC. Fluoroscopic Reduction Techniques for Catheter Ablation of Cardiac Arrhythmias. Minneapolis, MN: Cardiotext; 2019.
9. Canpolat U, Faggioni M, Rocca DGG, et al. State of fluoroless procedures in cardiac electrophysiology practice. J Innov Card Rhythm Manag. 2020;11(3):4018-4029. doi:10.19102/icrm.2020.110305
10. Razminia M, Zei P. Fluoroless catheter ablation of cardiac arrhythmias: change is inevitable. J Innov Card Rhythm Manag. 2020;11(4):4076-4078. doi:10.19102/icrm.2020.110406
11. Alyesh D, Venkataraman G, Stucky A, et al. Acute safety and efficacy of fluoroless cryoballoon ablation for atrial fibrillation. J Innov Card Rhythm Manag. 2021;12(2):4413-4420. doi:10.19102/icrm.2021.120205
12. Doshi RN. Atrial fibrillation ablation without fluoroscopy: because we can. J Innov Card Rhythm Manag. 2018;9(11):3391-3394. doi:10.19102/icrm.2018.091103
13. Verma A, Haines DE, Boersma LV, et al. Pulsed field ablation for the treatment of atrial fibrillation: PULSED AF pivotal trial. Circulation. 2023;147(19):1422-1432. doi:10.1161/CIRCULATIONAHA.123.063988
Related Content