

Atrial Fibrillation in Emergency Department Patients With COVID-19: Review of Literature
Though traditionally thought of as a pulmonary illness, SARS-CoV-2 infection has been shown to have significant impact on the cardiovascular system and has been linked to cardiac arrhythmias, myocardial ischemia, myocarditis, venous thromboembolism, and heart failure.1-3 In many cases, these risks persist for up to 1 year after illness.4 Patients with preexisting cardiovascular disease have significantly higher mortality rates from SARS-CoV-2 and are more likely to experience an acute cardiac event during their illness.5 There is an increased prevalence of multiple cardiac arrhythmias during infection, with studies suggesting an incidence of 17% in hospitalized patients.6
Atrial fibrillation (AF) is defined by an irregular heart rhythm caused by atria that beat out of coordination with the ventricles.7 AF has been shown to be a complication of an acute SARS-CoV-2 infection, with a recent meta-analysis showing a prevalence of 11% during illness in contrast to a prevalence of between 2.3%-3.4% in the general population.8,9 Patients with more severe infection were more likely to have AF compared with patients with milder cases. While the exact mechanism of this relationship has not been elucidated, there are several suspected theories.10
AF is associated with increased levels of angiotensin-converting enzyme 2 (ACE-2), an enzyme on the surface of cardiac cells.11 ACE-2 is associated with atria remodeling and predisposes individuals to enter AF. In SARS-CoV-2 infection, ACE-2 also acts as a receptor for the virus, allowing viral entry. Individuals with a higher number of these receptors are more prone to higher viral loads. The dysregulation of ACE-2 receptors also allows for a decreased production rate of angiotensin II over angiotensin-I (1-7), which ultimately increases the release of reactive oxygen species and increases vascular permeability.3 This cascade generates more inflammation. An underlying inflammatory state is thought to contribute to the development of both worse SARS-CoV-2 infection and predisposes cardiac tissue to AF.10 Furthermore, SARS-CoV-2 has been shown to cause respiratory thromboembolic disease, which if it becomes chronic, can lead to pulmonary hypertension (PH).12 PH is an independent risk factor for the development of AF and may be a mechanism by which these 2 conditions are linked.
Studies of floor and intensive care unit patients have shown an increased mortality in SARS-CoV-2 infections when patients have concurrent AF.13 Patients with AF ultimately have a higher chance of all-cause mortality during infection.14 This was true for existing AF (odds ratio [OR], 2.98; 95% CI, 1.91-4.66) as well as new-onset AF (OR, 2.32; 95% CI, 1.60-3.37).8,15 While this has been established in studies evaluating hospitalized patients, to date, there are very few studies on emergency department (ED) presentations of AF during the pandemic period. This articles explores the current knowledge about the impact of COVID-19 on AF presentations to the ED.
Literature Review Process
We reviewed data from 3 separate retrospective studies. A 2021 study by Bilaszewski et al analyzed 497 charts for patients that presented to 2 EDs in Poland.16 The study compared the quantity and quality of AF episodes prepandemic vs during the pandemic, as well as differences in therapeutic approaches.16
The second study retrospectively examined cases of AF and electrical cardioversion at an ED in Austria.17 A total of 2310 bouts of AF and 511 sessions of electrical cardioversion were included in the study.17 From January 1, 2020, through May 31, 2020, an ED in Vienna evaluated documented cases of AF and associated electrical cardioversion episodes. AF incidence for the years 2017, 2018, and 2019 were used as controls and the investigators conducted inter- and intra-year analyses.17
The last study was a retrospective observational investigation performed in Italy by D’Ascenzi et al in March 2021.18 During the first 4 months of 2020, investigators evaluated patients who called the emergency medical system (EMS) or presented with cardiac complaints to one of the study’s 39 ED locations in Tuscany. The data was compared to the same period in 2018-2019.18
Summary of Literature
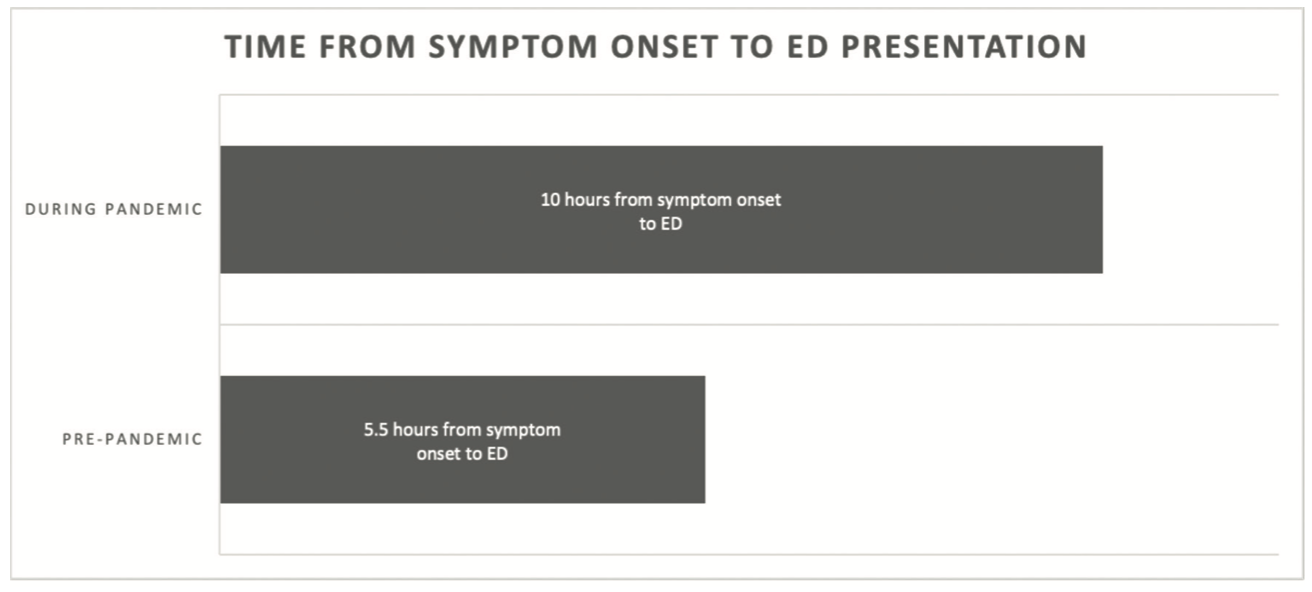
A retrospective comparison of ED visits for AF periods before (July-December 2019) and during (July-December 2020) the pandemic showed a significant decrease in patients with AF as their principal complaint (Figure 1).16 Patients were found to present later with new-onset AF during the pandemic period (symptoms beginning 10 hours prior vs 5 hours prepandemic). The total number of AF episodes treated in the ED was lower during the pandemic compared to prepandemic (Figure 2). The authors also found that prepandemic, there were more frequent successful cardioversions in the prepandemic group. Although there were slight differences between the 2 hospital locations in patient demographics and treatment patterns, the trends in AF presentation were consistent across both sites.
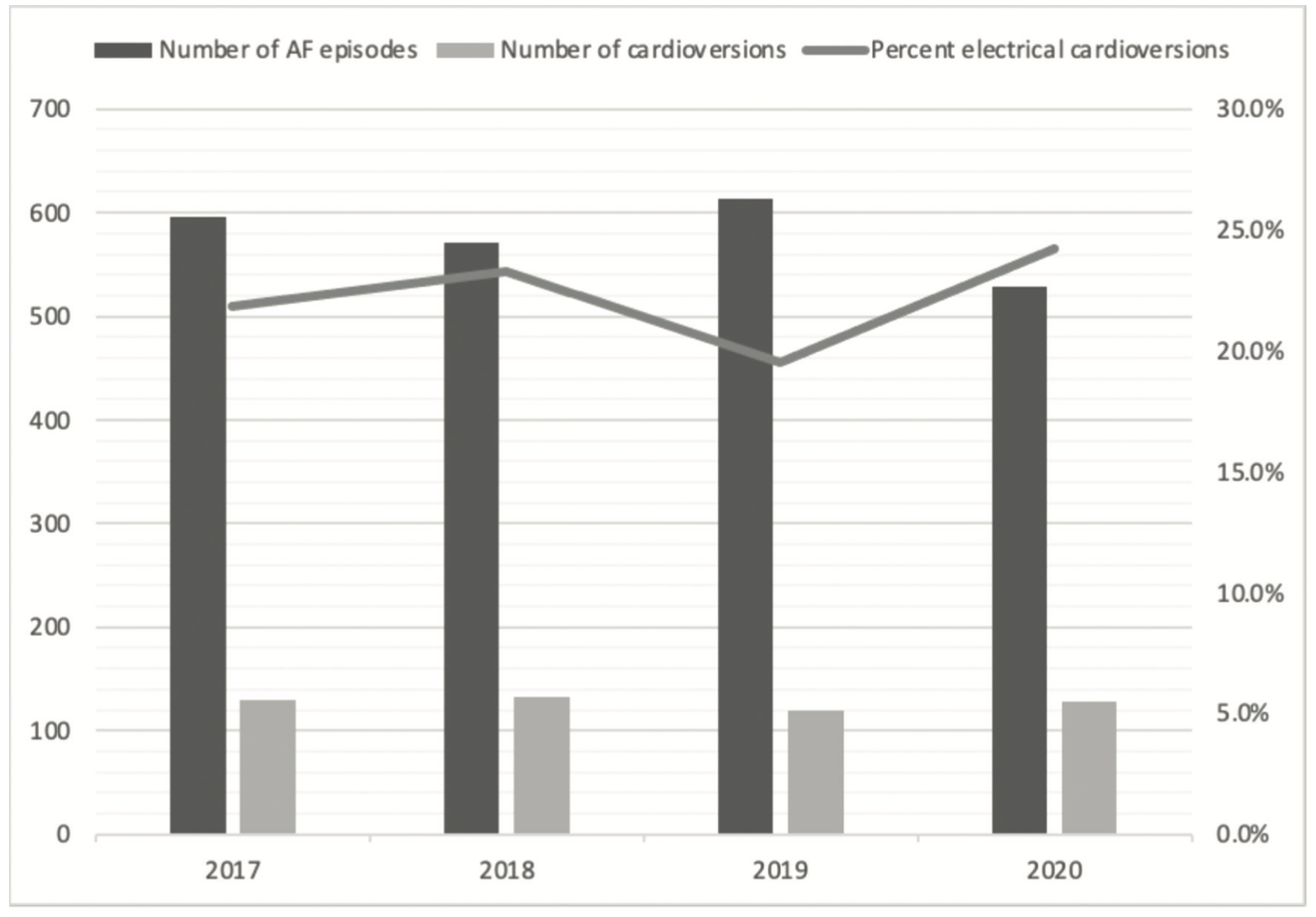
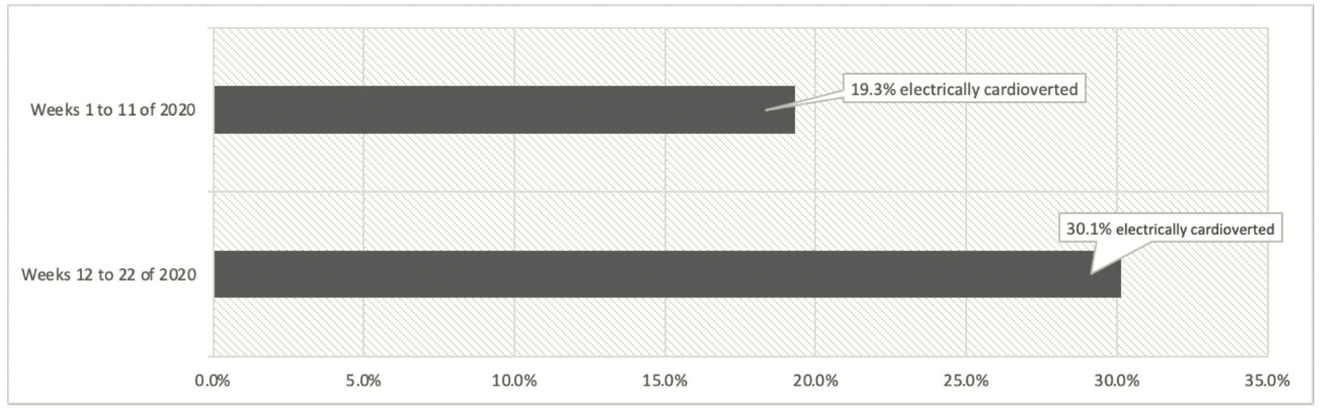
In the second study, the intra-year analysis from 2020 showed a trend toward decreased incidence of AF and increased electrical cardioversions (Figure 3). This could be due to the contribution of several factors. An increased threshold to seek clinical care may cause the in-hospital population to be a selective group of more refractory cases. There also was likely an increased shift of patients from specialist centers to the ED, especially early in the pandemic period. Patients often presented later after AF onset, which may make it harder to terminate the arrhythmia. It has also been hypothesized that increased stress levels over the pandemic period may result in more refractory cases, though this relationship has not been definitively established.17,19
In the third study, investigators found that a diagnosis of AF in the EDs was significantly higher in February 2018 and 2019, compared to February 2020 at the start of the COVID-19 pandemic (P<.05).18 The authors suggest that fear of contagion at the hospital likely played a role in why patients avoided contacting EMS or going to the ED during the initial wave of the COVID-19 pandemic.
Discussion
There is a significant impact of the ongoing SARS-CoV-2 pandemic on AF presentations to the ED, including trends in the number of admissions for a primary diagnosis of AF as well as new trends in delayed treatment for AF.16,17,19 These findings are consistent with studies evaluating AF in SARS-CoV-2 on the inpatient side.11 However, these studies are all focused on 1 or 2 centers.16,17 While they report findings in keeping with anecdotal international trends, a multicenter evaluation or meta-analysis will need to be done to confirm these studied populations are not unique. Additionally, as compared to inpatient studies, there is still a relatively limited number of ED-based research on AF presentations during the COVID-19 pandemic. Ongoing future research and meta-analysis is needed to better understand how SARS-CoV-2 has impacted the incidence and presentation of AF.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. They have no conflicts of interest to report regarding the content herein.
References
1. Corrales-Medina VF, Musher DM, Shachkina S, Chirinos JA. Acute pneumonia and the cardiovascular system. Lancet. 2013;381(9865):496-505. doi:10.1016/S0140-6736(12)61266-5
2. Guo T, Fan Y, Chen M, et al. Cardiovascular implications of fatal outcomes of patients with coronavirus disease 2019 (COVID-19). JAMA Cardiol. 2020;5(7):811-818. doi:10.1001/jamacardio.2020.1017
3. Driggin E, Madhavan MV, Bikdeli B, et al. Cardiovascular considerations for patients, health care workers, and health systems during the COVID-19 pandemic. J Am Coll Cardiol. 2020;75(18):2352-2371. doi:10.1016/j.jacc.2020.03.031
4. Xie Y, Xu E, Bowe B, Al-Aly Z. Long-term cardiovascular outcomes of COVID-19. Nat Med. 2022;28(3):583-590. doi:10.1038/s41591-022-01689-3
5. Bae SA, Kim SR, Kim MN, Shim WJ, Park SM. Impact of cardiovascular disease and risk factors on fatal outcomes in patients with COVID-19 according to age: a systematic review and meta-analysis. Heart. 2021;107(5):373-380. doi:10.1136/heartjnl-2020-317901
6. Bhatla A, Mayer MM, Adusumalli S, et al. COVID-19 and cardiac arrhythmias. Heart Rhythm. 2020;17(9):1439-1444. doi:10.1016/j.hrthm.2020.06.016
7. Nattel S, Burstein B, Dobrev D. Atrial remodeling and atrial fibrillation: mechanisms and implications. Circ Arrhythm Electrophysiol. 2008;1(1):62-73. doi:10.1161/CIRCEP.107.754564
8. Li Z, Shao W, Zhang J, et al. Prevalence of atrial fibrillation and associated mortality among hospitalized patients with COVID-19: a systematic review and meta-analysis. Front Cardiovasc Med. 2021;8:1314. doi:10.3389/fcvm.2021.720129
9. Ball J, Carrington MJ, McMurray JJV, Stewart S. Atrial fibrillation: profile and burden of an evolving epidemic in the 21st century. Int J Cardiol. 2013;167(5):1807-1824. doi:10.1016/j.ijcard.2012.12.093
10. Uribarri A, Núñez-Gil IJ, Aparisi Á, et al. Atrial fibrillation in patients with COVID-19. Usefulness of the CHA2DS2-VASc score: an analysis of the international HOPE COVID-19 registry. Rev Esp Cardiol (Engl Ed). 2021;74(7):608-615. doi:10.1016/j.rec.2020.12.009
11. Szarpak L, Filipiak KJ, Skwarek A, et al. Outcomes and mortality associated with atrial arrhythmias among patients hospitalized with COVID-19: a systematic review and meta-analysis. Cardiol J. 2022;29(1):33-43. doi:10.5603/CJ.a2021.0167
12. Wanamaker B, Cascino T, McLaughlin V, Oral H, Latchamsetty R, Siontis KC. Atrial arrhythmias in pulmonary hypertension: pathogenesis, prognosis and management. Arrhythm Electrophysiol Rev. 2018;7(1):43-48. doi:10.15420/aer.2018.3.2
13. Ip RJ, Ali A, Baloch ZQ, et al. Atrial fibrillation as a predictor of mortality in high risk COVID-19 patients: a multicentre study of 171 patients. Heart Lung Circ. 2021;30(8):1151-1156. doi:10.1016/j.hlc.2021.02.010
14. Sanz AP, Tahoces LS, Pérez RO, et al. New-onset atrial fibrillation during COVID-19 infection predicts poor prognosis. Cardiol J. 2021;28(1):34-40. doi:10.5603/CJ.a2020.0145
15. Mountantonakis SE, Saleh M, Fishbein J, et al. Atrial fibrillation is an independent predictor for in-hospital mortality in patients admitted with SARS-CoV-2 infection. Heart Rhythm. 2021;18(4):501-507. doi:10.1016/j.hrthm.2021.01.018
16. Bilaszewski Ł, Timler W, Budrewicz K, et al. The impact of COVID-19 on admissions and management of patients with atrial fibrillation episodes in the emergency department. Int J Environ Res Public Health. 2021;18(11):6048. doi:10.3390/ijerph18116048
17. Schnaubelt S, Domanovits H, Niederdoeckl J, et al. The impact of the COVID-19 pandemic on incidences of atrial fibrillation and electrical cardioversion at a tertiary care emergency department: an inter- and intra-year analysis. Front Med (Lausanne). 2020;7:595881. doi:10.3389/fmed.2020.595881
18. D’Ascenzi F, Cameli M, Forni S, et al. Reduction of emergency calls and hospitalizations for cardiac causes: effects of COVID-19 pandemic and lockdown in Tuscany region. Front Cardiovasc Med. 2021;8:625569. doi:10.3389/fcvm.2021.625569
19. Gawałko M, Kapłon-Cieślicka A, Hohl M, Dobrev D, Linz D. COVID-19 associated atrial fibrillation: incidence, putative mechanisms and potential clinical implications. Int J Cardiol Heart Vasc. 2020;30:100631. doi:10.1016/j.ijcha.2020.100631

