

The Promise of Pulsed Field Ablation: An Update
Introduction
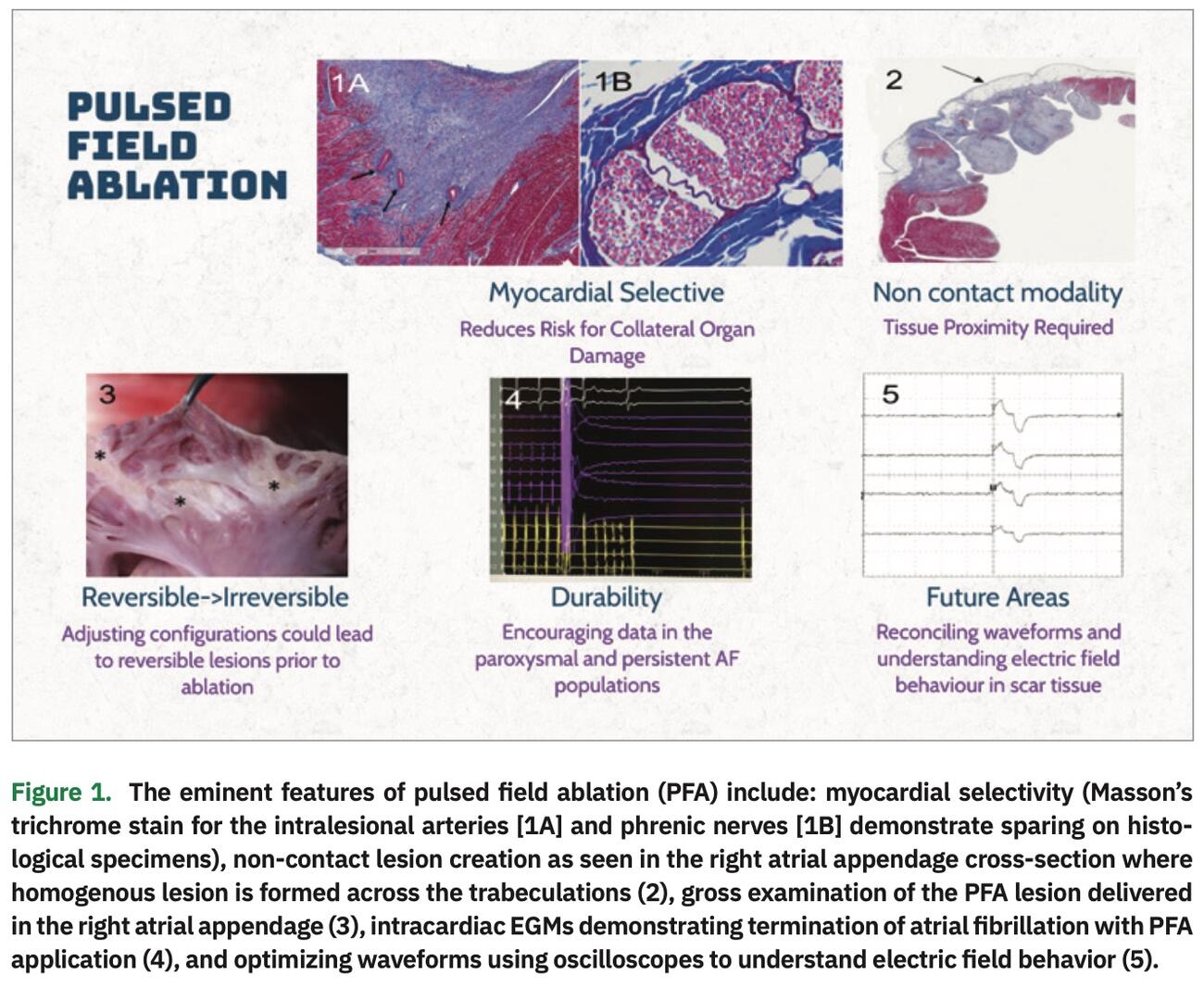
With atrial fibrillation (AF) being the most common arrhythmia requiring treatment, ablation modalities are now emerging as front-line management options. In an ideal setting, the ablation modality should be able to create transmural lesions to the targeted tissue and yet avoid attendant collateral injury. However, safety and efficacy are a zero-sum game. Higher efficacy generally translates to more aggressive ablation, which can threaten the safety of the procedure. Pulsed field ablation (PFA) appears to rise to this challenge, but with some important caveats as highlighted during the 2021 Great Debates and Updates in Electrophysiology (ep.greatdebatesandupdates.com) conference. This article serves as an update to the advances in PFA since our last article in 2019 (summarized in Figure 1), and we aim to revisit the important questions regarding PFA that remain to be answered.1
Broadly, the mechanism of PFA is the creation of aqueous pores in the cell membrane via high-voltage electric field application. The pores increase cell permeability, and with lower voltages, can reseal without permanent cell damage.
This is known as reversible electroporation. This property has been historically used for delivery of cytotoxic drugs via induced pores in tumor cells and cellular gene transfection.2 However, with higher voltage electric fields, this dielectric breakdown of the sarcolemmal membrane is irreversible and results in irreversible electroporation (IRE).3 The cardiac applications of IRE have evolved into the development of PFA technology for the treatment of atrial fibrillation.
Pathophysiology of PFA Lesions
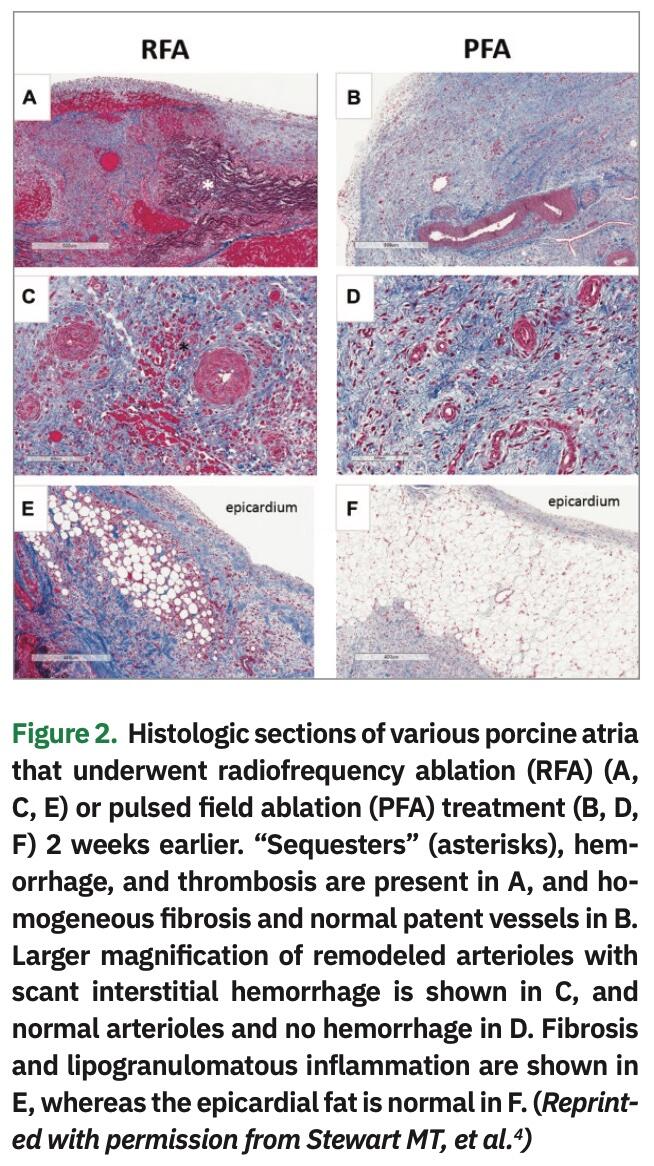
PFA lesions are characterized by homogeneity compared to radiofrequency ablation (RFA) lesions, which show inhomogeneity with many islands of sequestered viable myocytes. Compared to RFA, PFA deliveries do not cause epicardial fat tissue inflammation in the treated area or noteworthy arteriolar remodeling (Figure 2).4 IRE lesions show homogenous organized fibrotic replacement of the myocytes without the inflammatory signatures that accompany other ablation modalities. IRE is associated with extracellular matrix preservation,5 unlike RFA, which shows significant denaturation of collagen.6 One can speculate that an unperturbed extracellular matrix could possibly lead to lower left atrial (LA) stiffness and lower risk of stiff LA syndrome, as is seen after some cases of extensive RFA.6 However, this needs to be investigated. Early reports show transient impact on the conduction system with recovery. This property, in conjunction with reversible electroporation, could lend additional utility as a modality for mapping prior to ablation of the target area, akin to cryomapping.7 Most of the PFA research has focused on ablation of the atrial substrate in experimental animals with normal hearts. Understanding the electric field behavior across scar tissue will be of value, especially as we extend applications into the persistent AF substrate and ventricular arrhythmias.
Effectiveness Across Different Atrial Thicknesses and Structures
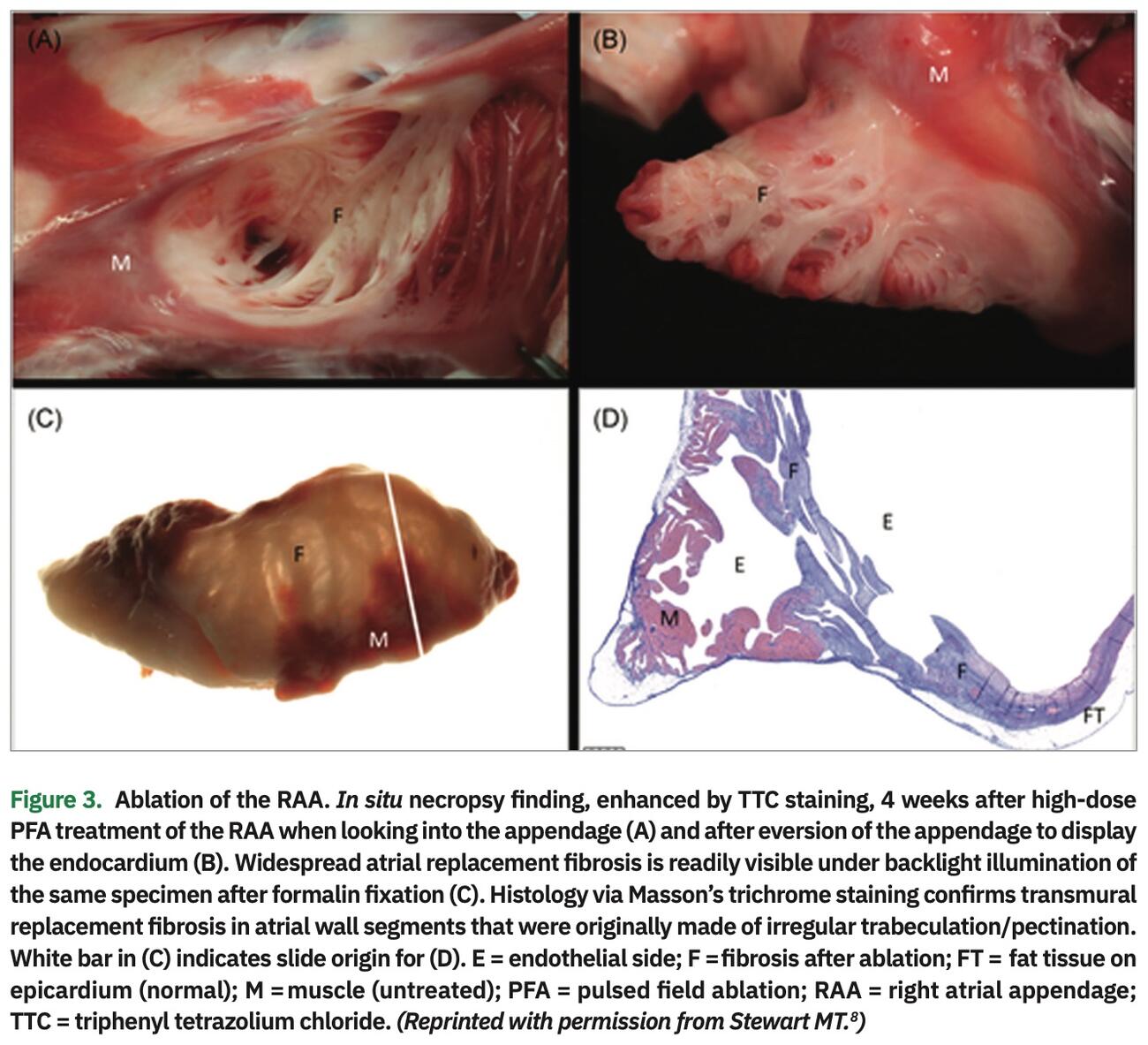
Owing to electric field behavior, PFA is not reliant on contact as long as there is tissue proximity. This leads to increased effectiveness across different cardiac structures. The preclinical application of overlapping PFA application on sites with smooth and trabeculated surfaces of the heart including the superior vena cava, right atrial appendage, and right superior pulmonary vein have been shown to produce transmural, contiguous, and circumferential lesions, as seen in Figure 3. In addition, this porcine study demonstrated acute and chronic safety data at 4 weeks.8
Non-Thermal Nature Could Prove to be Less Thrombogenic and Reduce Pulmonary Vein Stenosis
Overall PFA is a non-thermal modality, as the cells die due to membrane permeabilization and not from a local increase in tissue temperature. The absence of meaningful tissue heating is based on the ultra-rapid delivery of electric pulses (nano to micro seconds in duration) coupled with convective cooling of circulating blood. In a report of PFA in a swine model, there was minimal increase in temperature (0.7°C with 700V applications and up to 5°C with 1500V application) with this delivery system, confirming the relative non-thermal nature of this modality.8 Theoretically, this may reduce the risk of endothelial thrombus and possible strokes following AF ablation. In this study, there was a 5% pulmonary vein narrowing with PFA compared to 46% narrowing with RF. This demonstrates the absence of significant heating. The pulmonary veins suffer thermal injury at 60°C or higher because of collagen degradation, resulting in scar and stenosis. The decrease in thermal delivery with PFA is a significant safety feature.
Higher Discriminative Potential With Mitigation of Collateral Injury
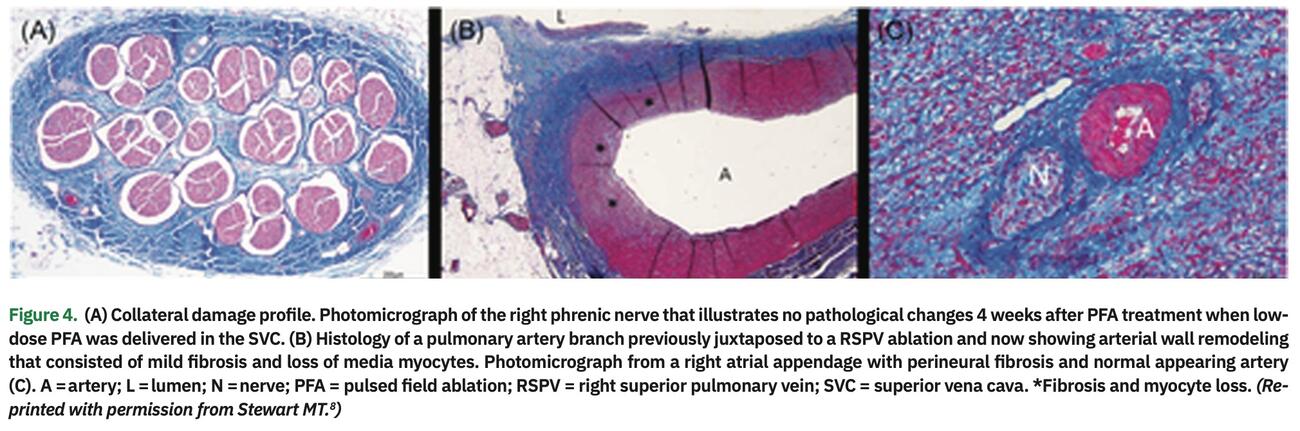
The unique promise of PFA lies in cardiac tissue selectivity, and several studies have confirmed this observation. While this mechanism is not well understood, striated muscle is thought to have lower threshold for IRE (400v/cm).8 There has been no evidence of epicardial adipose inflammation, vascular thrombus, phrenic nerve injury, or evidence of Wallerian degeneration/perineural fibrosis noted with PFA application (Figure 4). Interestingly, in a swine study, there was evidence of mild neointimal remodeling and non-myelinated autonomic nerve injury. The latter could be of benefit in ablating the autonomic plexi postulated to play a role in AF initiation and maintenance.8 The Varipulse directional circular lasso catheter (Biosense Webster, Inc., a Johnson & Johnson company) is coupled to an IRE ablation system using bipolar monophasic ablation with a relatively long pulse duration (250 ms). This was tested in swine, and 11/12 achieved pulmonary vein entrance block with a lesion width up to 14 mm. Chronic lesion stability was observed in this 30-day survival study. There was no evidence of phrenic or esophageal damage despite ablation overlaying these organs.9 The Pulmonary Vein Ablation Catheter (PVAC GOLD, Medtronic) was similarly tested in 8 swine and compared to RF. There was no evidence of pulmonary, esophageal, or vagal injury with PFA.10
This distinctive feature of cardiac selectivity allows electrophysiologists in clinical trials to deliver multiple rapidly delivered therapies around each pulmonary vein ostium without fear of collateral damage. The LA dwell time for the PFA catheter was 34 minutes in the PFA trial in paroxysmal AF patients, much shorter than the FIRE and ICE trial (92 and 109 minutes for cryoablation and radiofrequency ablation, respectively).11 Whether the myocardial selectivity is secondary to the lower electric field threshold affecting myocytes alone, or whether there are differences in electric field in different tissue, requires further investigation.
Gas Bubble Formation
PFA delivery systems have been shown to generate bubbles noted on intracardiac echocardiography due to electrolysis.11 Whether this translates to higher cerebral embolic events is of concern. However, a recent MRI study argued against this.12 In 9 canines, PFA in the ascending aorta did not lead to embolic cerebral lesions detected on MRI performed 1 and 5 days following ablation.12 This may differ from other ablation modalities where subclinical cerebral embolic events can be noted in up to 50% cases.12,13 In contrast, investigators studied ablation with a combination of both RFA and PFA using a novel delivery catheter, and reported a 15% prevalence of cerebral lesions in those patients who underwent routine cerebral MRI post procedure.14 Whether these lesions were complications of the transseptal catheterization, a result of PFA ablation or a result of combining PFA with RFA remains unclear. While the jury is out on the clinical significance of gas bubble formation,
Clinical Results: Atrial Fibrillation Results are Promising in the Paroxysmal, Persistent, and Longstanding Persistent Populations
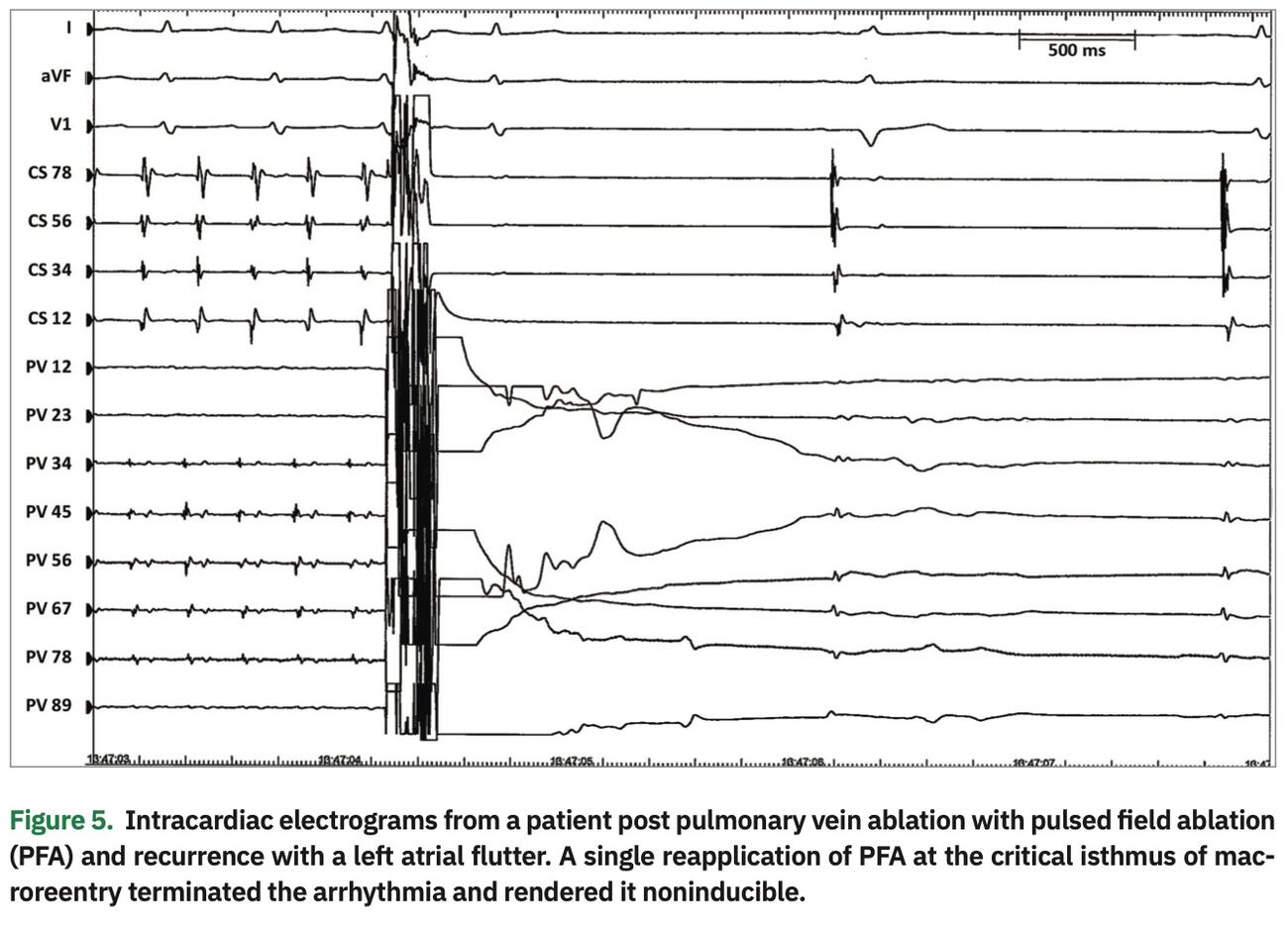
The IMPULSE and PEFCAT trials analyzed the outcomes of PFA in the symptomatic paroxysmal AF population with left ventricular ejection fraction of >40% and LA dimension <5 cm.11 This was an interesting study in which the sponsor iterated and optimized the ablation system using patients as the test subjects. Monophasic and biphasic waveforms from 900-2000V were optimized during the course of the trial. The success with remapping increased from 18 to 100% with successive waveform refinements. Echoing prior clinical reports, our experience suggests effective termination of atrial fibrillation and flutter with PFA delivery. (Figure 1 and 5)
In the recently published remapping group, in which 20 of the initial 45 patients with complete data sets were analyzed, the lesion set was durable if a threshold of <0.5 mV was selected to define scar. If this was reduced to 0.2-0.45 mV, there was slight regression of the scar formed compared to initial procedure.15
To date, pulmonary vein isolation (PVI), posterior wall isolation (LAPW), mitral isthmus ablation, and cavotricuspid isthmus (CTI) ablation with PFA have been clinically studied. Interestingly, LA mechanics have not been impaired contrasting to other ablation modalities. In 30 patients, cardiac MRI imaging was done before, within 3 hours, and 3 months post ablation in patients with paroxysmal AF undergoing PFA (16) or radiofrequency ablation.16 The authors reported that although the maximum strain decreased in both pulmonary veins with PFA and RFA, the PFA group demonstrated complete recovery in 3 months. The initial decline could be from myocardial edema, but at 3 months, the compliance of myocardial tissue was unaffected by PFA.16 Whether this could reduce incidence of stiff LA syndrome with extensive lesion sets needs to be studied further.17
A pilot trial testing PFA of the pulmonary veins and left atrial posterior wall with a pentaspline catheter and the CTI with a focal catheter at 1600-2000V biphasic bipolar application was performed in 25 patients. Conscious sedation was used in 80% of these cases. Investigators showed 96% durable PVI and 100% posterior wall isolation with remapping at 3-month follow-up in 25 patients. LA dwell time was 22 minutes. Thirteen patients underwent CTI ablation with 100% durability at the acute and remapping time point. One patient had inadvertent left atrial appendage isolation, which recovered during the remapping procedure. There was no evidence of esophageal damage on post-procedure EGD studies. There was localized scar regression in 3 patients, but this was not associated with recurrence. Further follow-up of this population showed high arrhythmia-free survival (23 of 25 patients at 1 year) with posterior wall and pulmonary vein isolation based on transtelephonic monitoring and Holter analysis. Only one patient remained on amiodarone at follow-up.18,19
Transition Zones Appear to be Narrow and Stable Without Significant Regression
In the swine model using the proprietary PulseSelect Pulsed Field Ablation System (Medtronic), Masson’s trichrome staining showed abrupt pathological transition from transmural replacement fibrosis to normal non-treated superior vena cava muscle. However, this was observed on pathological exam and did not assess functional electrical block.8 In the PEFCAT study population, voltage mapping of 20 patients, followed at a median of 84 days post PFA procedure, revealed no significant difference between the isolated antral regions of pulmonary veins compared to non-ablated posterior wall. In addition, the low-voltage area distance between the left and right pulmonary veins was also similar, suggesting no significant regression in lesion size.15 Despite these observations, early reports from investigators participating in clinical trials of PFA have noted some AF recurrence among patients with acutely successful PVI, indicating some propensity for lesion reversibility (Figure 1).
Prescriptive Doses, Delivery Systems, and Adjunct Modalities
Although over 7 manufacturers have introduced cardiac PFA equipment in the cardiac arena, the proprietary specifications are not publicly available. This makes comparison of these systems challenging. Understanding the biophysical parameters, which govern the lesion size, is important.20 Unlike radiofrequency modalities, where power duration and irrigation platforms can be compared, the PFA systems are more complex and simple comparisons are not easily possible. There are several variables in generating the electric field waveforms: unipolar/bipolar, monophasic/biphasic, AC/DC, voltage settings, inter and intrapulse duration, and number of pulse trains.1 In addition, there are different catheter configurations: adaptable (linear to basket to petal shaped) vs fixed. Additional advances include radiofrequency and PFA delivery systems combined in one to enhance versatility.
Pacemaker Interactions
In theory, pacemakers in the vicinity of the PFA field could perturb the electric field behavior and lead to pacemaker malfunction. This could be from the metal casing or electrode contact. The pacemaker could act as a large ground electrode and draw current from the PFA delivery. In a series of in vitro and numerical modeling experiments, the presence of a pacemaker and leads led to a higher electric field and up to 5°C increased heating with 1000V and 3000V at 100-µs duration. The interference dropped with increasing distance and was deemed to be safe with distances beyond 3 cm. No pacemaker malfunction was noted, and thermal damage from the pacemaker was less likely on numerical stimulations.21
Territories to be Explored and Next Frontiers
Given the singular advantage of cardiac selectivity, left ventricular summit arrhythmias and extensive substrate modifications could now be within reach. With titration of parameters, deeper lesions are now possible but will require understanding of how the myocyte orientation and presence of intramural fibrosis and scar could alter the electric field. Furthermore, reconciling different parameters from the major PFA contenders will pose another challenge, as it is likely that one size will not fit all.
References
1. Haines DE, Bradley CJ. The promise of pulsed field ablation. EP Lab Digest. 2019;19:1-3.
2. Gehl J. Electroporation: theory and methods, perspectives for drug delivery, gene therapy and research. Acta Physiol Scand. 2003;177:437-447.
3. Aycock KN, Zhao Y, Lorenzo MF, Davalos RV. A theoretical argument for extended interpulse delays in therapeutic high-frequency irreversible electroporation treatments. IEEE Trans Biomed Eng. 2021;68:1999-2010.
4. Stewart MT, Haines DE, Verma A, et al. Intracardiac pulsed field ablation: proof of feasibility in a chronic porcine model. Heart Rhythm. 2019;16:754-764. doi: 10.1016/j.hrthm.2018.10.030
5. Zager Y, Kain D, Landa N, Leor J, Maor E. Optimization of irreversible electroporation protocols for in-vivo myocardial decellularization. PLoS One. 2016;11:e0165475.
6. Packer M. Effect of catheter ablation on pre-existing abnormalities of left atrial systolic, diastolic, and neurohormonal functions in patients with chronic heart failure and atrial fibrillation. Eur Heart J. 2019;40:1873-1879.
7. van Zyl M, Ladejobi AO, Tri JA, et al. Reversible atrioventricular conduction impairment following bipolar nanosecond electroporation of the interventricular septum. JACC Clin Electrophysiol. 2021;7:255-257.
8. Stewart MT, Haines DE, Miklavcic D, et al. Safety and chronic lesion characterization of pulsed field ablation in a porcine model. J Cardiovasc Electrophysiol. 2021;32:958-969.
9. Yavin H, Brem E, Zilberman I, et al. Circular multielectrode pulsed field ablation catheter lasso pulsed field ablation: lesion characteristics, durability, and effect on neighboring structures. Circ Arrhythm Electrophysiol. 2021;14:e009229.
10. Howard B, Haines DE, Verma A, et al. Reduction in pulmonary vein stenosis and collateral damage with pulsed field ablation compared with radiofrequency ablation in a canine model. Circ Arrhythm Electrophysiol. 2020;13:e008337.
11. Reddy VY, Neuzil P, Koruth JS, et al. Pulsed field ablation for pulmonary vein isolation in atrial fibrillation. J Am Coll Cardiol. 2019;74:315-326.
12. Neven K, Futing A, Byrd I, et al. Absence of (sub-)acute cerebral events or lesions after electroporation ablation in the left-sided canine heart. Heart Rhythm. 2021;18:1004-1011.
13. Siklody CH, Deneke T, Hocini M, et al. Incidence of asymptomatic intracranial embolic events after pulmonary vein isolation: comparison of different atrial fibrillation ablation technologies in a multicenter study. J Am Coll Cardiol. 2011;58:681-688.
14. Reddy VY, Anter E, Rackauskas G, et al. Lattice-tip focal ablation catheter that toggles between radiofrequency and pulsed field energy to treat atrial fibrillation: a first-in-human trial. Circ Arrhythm Electrophysiol. 2020;13:e008718.
15. Kawamura I, Neuzil P, Shrivamurthy P, et al. Does pulsed field ablation regress over time? A quantitative temporal analysis of pulmonary vein isolation. Heart Rhythm. 2021;18:878-884.
16. Nakatani Y, Cheniti G, Sridi S, et al. Pulsed field ablation preserves atrial mechanics after catheter ablation for atrial fibrillation. Heart Rhythm. 2020;D-AB24-01.
17. Ramirez FD, Reddy VY, Viswanathan R, Hocini M, Jais P. Emerging technologies for pulmonary vein isolation. Circ Res. 2020;127:170-183.
18. Reddy VY, Anic A, Koruth J, et al. Pulsed field ablation in patients with persistent atrial fibrillation. J Am Coll Cardiol. 2020;76:1068-1080.
19. Reddy VY, Neuzil P, Anic A. Reply: pulsed field ablation for persistent atrial fibrillation: do electrophysiological endpoints predict clinical benefit? J Am Coll Cardiol. 2020;76:3065-3066.
20. Anic A, Breskovic T, Sikiric I. Pulsed field ablation: a promise that came true. Curr Opin Cardiol. 2021;36:5-9.
21. Jarm T, Krmac T, Magjarevic R, Kos B, Cindric H, Miklavcic D. Investigation of safety for electrochemotherapy and irreversible electroporation ablation therapies in patients with cardiac pacemakers. Biomed Eng Online. 2020;19:85.

