

‘Wear’ Are We? Digital Health Tools in the Detection and Management of Atrial Fibrillation
EP Lab Digest. 2023;23(1):1,11-13.
Deepti Ranganathan, MBChB, and Christopher C Cheung, MD, MPH, Sunnybrook Health Sciences Centre, University of Toronto, Toronto, Ontario, Canada
The incidence of atrial fibrillation (AF) is increasing, with an expected prevalence of 12.1 million people in the United States by 2050 and 17.9 million people in Europe by 2060.1 Early diagnosis of AF facilitates risk factor modification, early rhythm control, and anticoagulation initiation for stroke prevention.2 Untreated AF accounts for approximately 15%-20% of all strokes and is an independent risk factor for heart failure, cognitive decline, and increased mortality.3
Screening for AF
Given that one-third of patients with AF are asymptomatic, screening remains crucial.4 Various guidelines have recommended opportunistic electrocardiogram (ECG) screening in older patients, although the yield is variable, ranging from 1%-7%.5,6 AF screening studies have evaluated a combination of methods, ranging from point-of-care ECGs and ambulatory ECG monitoring to implantable cardiac monitors (ICM).7
The STROKESTOP trial demonstrated the benefits of systematic screening in an older population (aged 75 years or older). Intermittent ECG recording over a 2-week period detected AF in 3% of the study population and led to a small reduction in adverse outcomes (stroke or systemic embolism, bleeding, all-cause death) compared to those who did not undergo screening for AF.8 Similarly, the SCREEN-AF trial enrolled individuals aged 75 years or older with hypertension and detected new AF in 5.3% of patients with a 14-day patch monitor worn at baseline and 3 months.9 In the REVEAL-AF study, 385 patients with AF risk factors underwent ICM insertion and had an AF detection rate (defined as ≥6 minutes) of 40% at 30 months.10
Wearable Devices for AF Screening
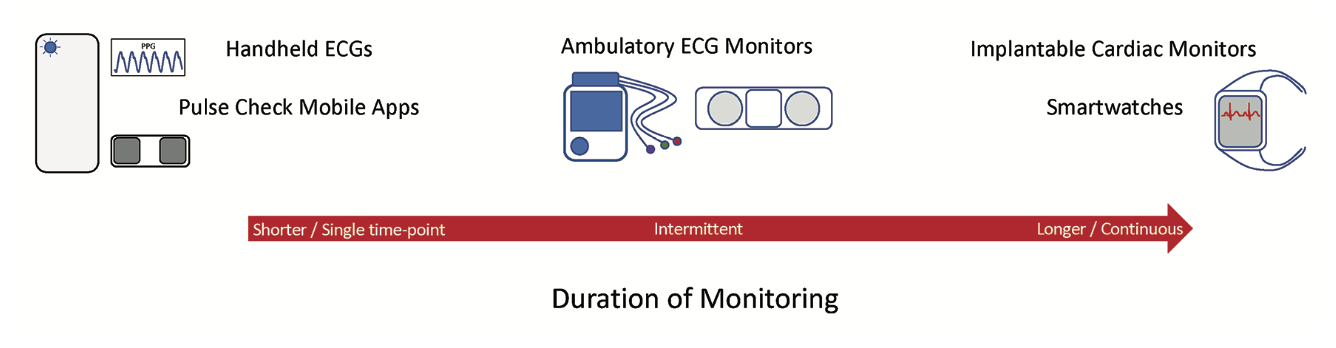
Simultaneous with the growth of patch monitors and ICMs for AF detection is the development of handheld ECG devices for AF screening (Figure 1). A recent European Heart Rhythm Association survey reported increased use of wearable devices among physicians.11 By recording a single-lead ECG, handheld devices can achieve high accuracy in detecting AF and are increasingly used for point-of-care ECG screening. In a Canadian study of 334 primary care practices and 16,817 patients, AF was detected using a single-lead ECG in 7% of patients.12
There has also been a proliferation of smartwatches and consumer-facing devices with added functionality for AF screening. The number of smartwatch users worldwide was estimated to be more than 200 million users in 2022.13 With increased global access to technology, these mobile health tools can support positive lifestyle modification, enhance health literacy and awareness, and potentially enable earlier arrhythmia detection.14
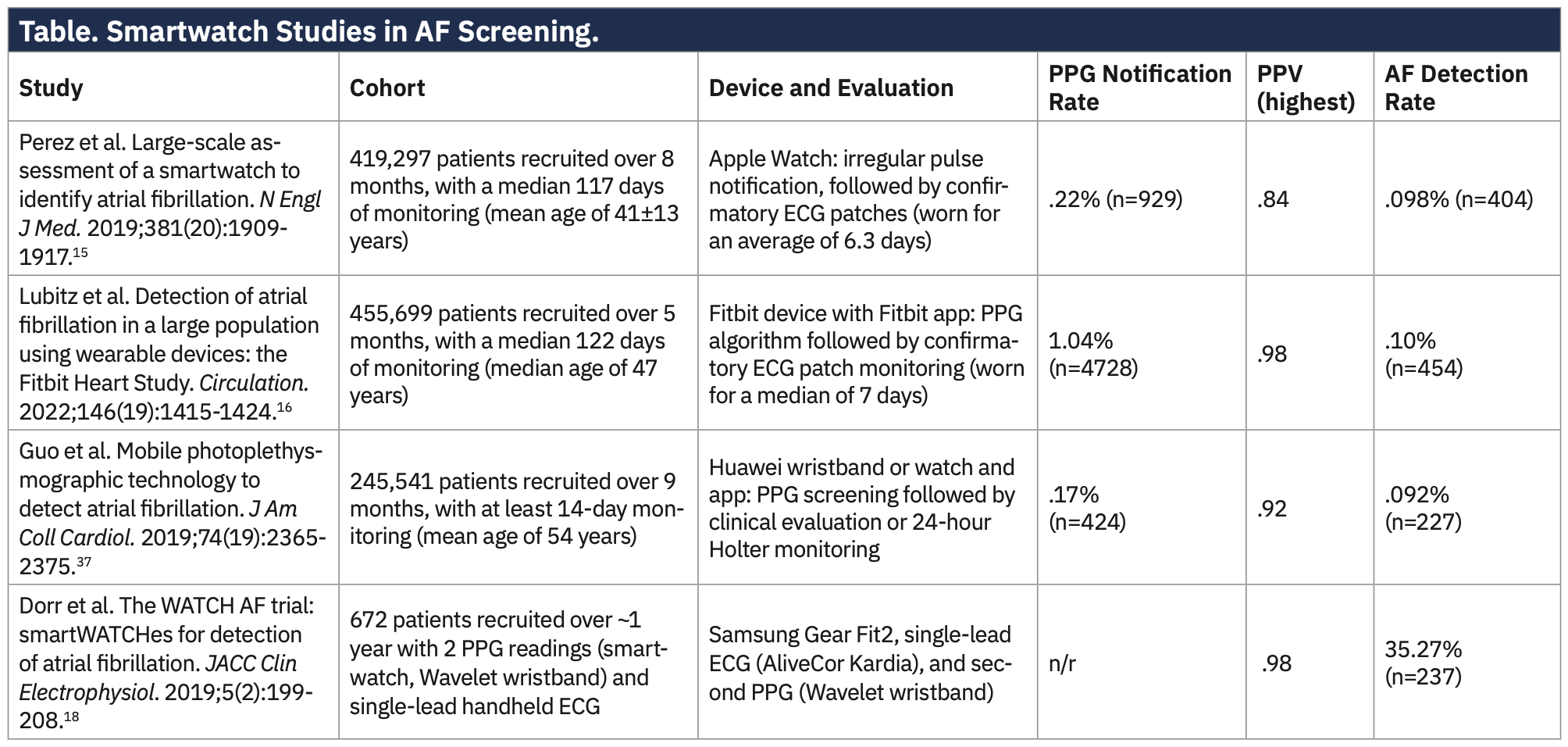
Population screening using smartwatches has been employed in several large studies. The Apple Heart Study enrolled 419,297 participants, with participants receiving an irregular rhythm notification and subsequently proceeding to confirmatory ECG patch monitoring. New AF was diagnosed in a subset of participants with a positive predictive value (PPV) of 84% for the irregular rhythm notification.15 The Fitbit Heart Study enrolled 455,699 participants and reported high PPVs (97.0%-98.2% depending on age).16 In a systematic review, smartwatches demonstrated a high diagnostic accuracy with a sensitivity and specificity of 94% and 93%, respectively.17 Four prominent smartwatch studies are summarized in the Table.
Limitations of Wearable Devices for AF Screening
Wearable technologies also have their limitations. Even small reductions in diagnostic accuracy, when applied on a population level, can result in a substantial increase in false-positive results in low-risk populations. False-positives can lead to over-investigation and unnecessary patient anxiety. Furthermore, the high diagnostic accuracies reported in healthy population studies may not necessarily be generalizable to higher risk populations. For example, in the WATCH-AF trial, 21.8% of smartwatch recordings among hospitalized patients were deemed not suitable for analysis.18
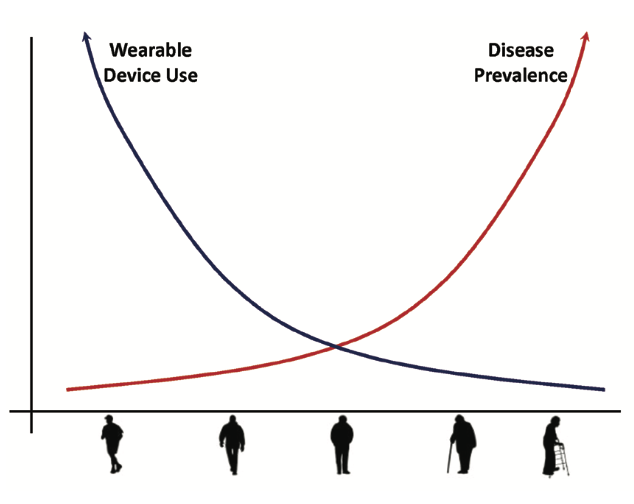
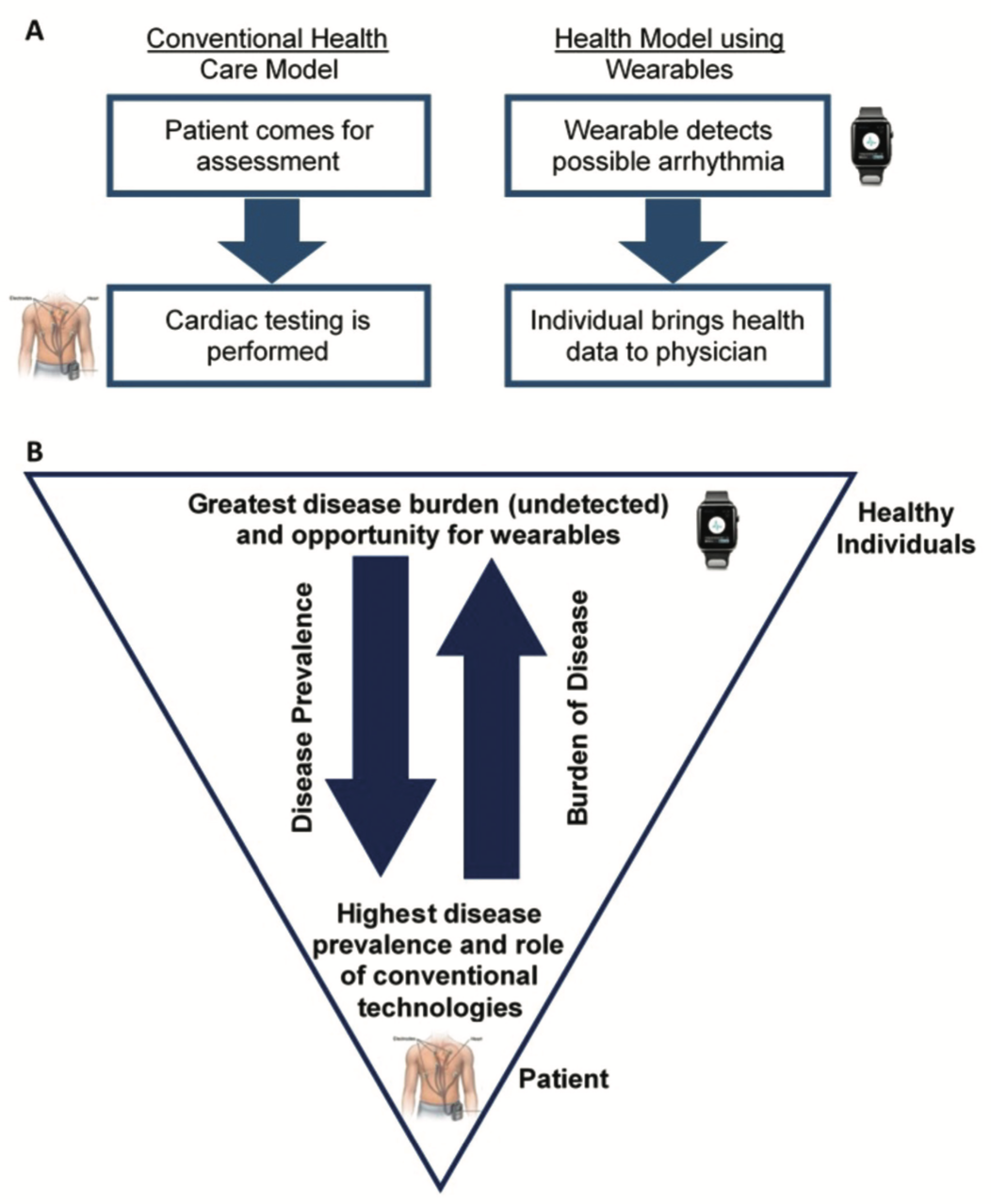
There is also a concern that older patients have barriers to adopting novel technology, thereby limiting the effectiveness of wearables in population screening studies. For example, in the Apple Heart Study, the majority of participants were young (mean age = 41 years) and only 5.9% of patients aged 65 or older were included in the study.15 With only 4.6% of smartwatch users older than 65 years with an age-adjusted prevalence of 5%, the PPV was 33%.19 This reflects an inherent paradox between smartwatch users and AF prevalence (Figure 2). Fortunately, other studies have suggested that this discordance can be mitigated. The eBRAVE-AF study recruited older patients with smartphones, with patients performing 2 photoplethysmogram (PPG) recordings per day over 14 days. In addition to a higher AF detection rate (1.33% vs .63%), older patients also performed more PPG recordings compared to younger patients.20
Management of subclinical AF in patients with implantable cardiac devices, and by extension, wearable-detected AF, remains an area of therapeutic uncertainty.19 For example, the threshold AF duration and interplay of CHA2DS2-VASc risk factors for determining anticoagulation initiation in subclinical AF is still debated.21 While longer episodes of subclinical AF (>24 hours) may benefit from anticoagulation,22 shorter episodes (<24 hours) are currently subject to ongoing trials.23 In patients with AF detected using a single-lead device, physicians are also more hesitant to prescribe anticoagulation in these individuals without confirmatory testing.11 Whether wearable-detected AF itself may represent a further layer of complexity in this risk calculation remains unknown.
Digital Health Tools for Managing AF
Digital health tools are poised to dramatically change our management of AF. Emerging methods in artificial intelligence have been shown to predict AF using ECGs recorded in normal sinus rhythm.24 These tools will allow physicians to identify high-risk patients, predict the future development of AF, and allow for prioritization of AF screening and targeted therapy accordingly.
Decentralized clinical studies will also substantially change our management of AF. Patients are increasingly comfortable both having their health care delivered and participating in clinical studies virtually. With smartwatch studies enrolling more than 400,000 participants in less than 12 months, future decentralized studies can leverage virtual platforms to answer clinical questions. MyHeart Counts25 and Health eHeart26 are examples of decentralized population studies that enrolled more than 50,000 and 66,000 participants, respectively. By digitizing aspects of the study such as enrollment, data collection, study visits, and outcomes, there is a great opportunity for broader patient inclusion and patient-reported outcomes with significant cost savings. This becomes crucial in ensuring minority representation and diversity in the validation of these digital tools.26
Emerging Opportunities and Future Directions for Wearable Devices
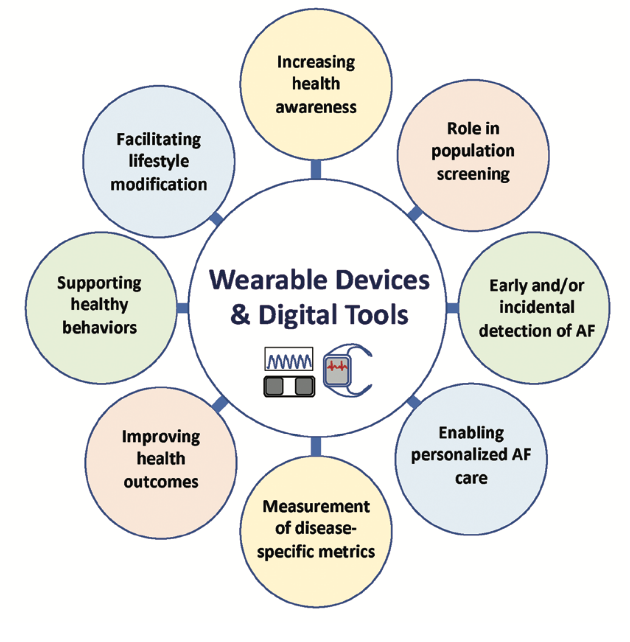
Patients and physicians are increasingly employing wearable devices to facilitate health care delivery (Figure 3). Examples such as the TeleCheck-AF project have demonstrated the effective use of an app-based, on-demand rhythm and rate monitoring infrastructure that provided teleconsultation for patients during the COVID-19 pandemic.27 Screening for AF using a handheld device has been shown to be cost-effective28-31 compared to conventional screening for AF. Adaptations in our existing health care infrastructure are necessary to integrate wearable devices into the health care system, with the goal of improving population outcomes and identifying cost savings (Figure 4).32
Continuous monitoring through wearable devices also provides exciting opportunities for AF screening and management. Intermittent AF episodes, previously detected by ICM, may be increasingly detected by wearable devices with important implications for management. New developments in smartwatches allow for the measurement of AF burden (a metric traditionally recorded by conventional cardiac monitors) and will add a new facet to AF management, particularly in patients undergoing rhythm control or considering catheter ablation.
Finally, timely AF detection will provide unique opportunities for personalized AF management. Guided by smartwatch AF detection, the REACT-AF trial will evaluate the safety and effectiveness of a pill-in-the-pocket approach to anticoagulation.33,34 Ongoing studies in subclinical AF will contribute to our understanding of when to initiate anticoagulation in these patients.
Conclusion
Digital health tools have the potential to improve the health of our patients with AF, from supporting positive lifestyle modification to disease prevention and early detection.35 In particular, wearable devices (ie, smartwatches and handheld ECGs) can be reliable and accurate when employed in specific circumstances. When integrated into our health care infrastructure and supported by telemedicine, these tools can empower patients and facilitate personalized AF care.36 While more studies are required to better understand how to best use and integrate these devices, there is much optimism about the future of wearables and digital health tools in the management of AF.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. They have no conflicts of interest to report regarding the content herein.
References
1. Dai H, Zhang Q, Much AA, et al. Global, regional, and national prevalence, incidence, mortality, and risk factors for atrial fibrillation, 1990-2017: results from the Global Burden of Disease Study 2017. Eur Heart J Qual Care Clin Outcomes. 2021;7(6):574-582. doi:10.1093/ehjqcco/qcaa061
2. Ruff CT, Giugliano RP, Braunwald E, et al. Comparison of the efficacy and safety of new oral anticoagulants with warfarin in patients with atrial fibrillation: a meta-analysis of randomised trials. Lancet. 2014;383(9921):955-962. doi:10.1016/S0140-6736(13)62343-0
3. Kotalczyk A, Lip GY, Calkins H. The 2020 ESC guidelines on the diagnosis and management of atrial fibrillation. Arrhythm Electrophysiol Rev. 2021;10(2):65-67. doi:10.15420/aer.2021.07
4. Dilaveris PE, Kennedy HL. Silent atrial fibrillation: epidemiology, diagnosis, and clinical impact. Clin Cardiol. 2017;40(6):413-418. doi:10.1002/clc.22667
5. Kaasenbrood F, Hollander M, de Bruijn SH, et al. Opportunistic screening versus usual care for diagnosing atrial fibrillation in general practice: a cluster randomised controlled trial. Br J Gen Pract. 2020;70(695):e427-e433. doi:10.3399/bjgp20X708161
6. Lubitz SA, Atlas SJ, Ashburner JM, et al. Screening for atrial fibrillation in older adults at primary care visits: VITAL-AF randomized controlled trial. Circulation. 2022;145(13):946-954. doi:10.1161/CIRCULATIONAHA.121.057014
7. Raja JM, Elsakr C, Roman S, et al. Apple Watch, wearables, and heart rhythm: where do we stand? Ann Transl Med. 2019;7(17):417. doi:10.21037/atm.2019.06.79
8. Svennberg E, Friberg L, Frykman V, Al-Khalili F, Engdahl J, Rosenqvist M. Clinical outcomes in systematic screening for atrial fibrillation (STROKESTOP): a multicentre, parallel group, unmasked, randomised controlled trial. Lancet. 2021;398(10310):1498-1506. doi:10.1016/S0140-6736(21)01637-8
9. Gladstone DJ, Wachter R, Schmalstieg-Bahr K, et al. Screening for atrial fibrillation in the older population: a randomized clinical trial. JAMA Cardiol. 2021;6(5):558-567. doi:10.1001/jamacardio.2021.0038
10. Conti S, Reiffel JA, Gersh BJ, et al. Baseline demographics, safety, and patient acceptance of an insertable cardiac monitor for atrial fibrillation screening: the REVEAL-AF study. J Atr Fibrillation. 2017;9(5):1551. doi:10.4022/jafib.1551
11. Manninger M, Zweiker D, Svennberg E, et al. Current perspectives on wearable rhythm recordings for clinical decision-making: the wEHRAbles 2 survey. Europace. 2021;23(7):1106-1113. doi:10.1093/europace/euab064
12. Andrade JG, Godin R, Nault I. Large-scale implementation of a pragmatic atrial fibrillation screening program in Canadian community practice. Pacing Clin Electrophysiol. 2020;43(7):768-769. doi:10.1111/pace.13966
13. Number of smartwatch users worldwide from 2017 to 2026. Statista. Published June 15, 2022. Accessed December 13, 2022. https://www.statista.com/forecasts/1314339/worldwide-users-of-smartwatches
14. Lopez Perales CR, Van Spall HGC, Maeda S, et al. Mobile health applications for the detection of atrial fibrillation: a systematic review. Europace. 2021;23(1):11-28. doi:10.1093/europace/euaa139
15. Perez MV, Mahaffey KW, Hedlin H, et al. Large-scale assessment of a smartwatch to identify atrial fibrillation. N Engl J Med. 2019;381(20):1909-1917. doi:10.1056/NEJMoa1901183
16. Lubitz SA, Faranesh AZ, Selvaggi C, et al. Detection of atrial fibrillation in a large population using wearable devices: the Fitbit Heart Study. Circulation. 2022;146(19):1415-1424. doi:10.1161/CIRCULATIONAHA.122.060291
17. Prasitlumkum N, Cheungpasitporn W, Chokesuwattanaskul A, et al. Diagnostic accuracy of smart gadgets/wearable devices in detecting atrial fibrillation: a systematic review and meta-analysis. Arch Cardiovasc Dis. 2021;114(1):4-16. doi:10.1016/j.acvd.2020.05.015
18. Dorr M, Nohturfft V, Brasier N, et al. The WATCH AF trial: smartWATCHes for detection of atrial fibrillation. JACC Clin Electrophysiol. 2019;5(2):199-208. doi: 10.1016/j.jacep.2018.10.006
19. Cheung CC, Gin KG, Andrade JG. Watch out: the many limitations in smartwatch-driven af detection. JACC Clin Electrophysiol. 2019;5(4):525-526. doi:10.1016/j.jacep.2018.10.006
20. Freyer L, von Stülpnagel L, Spielbichler P, et al. Rationale and design of a digital trial using smartphones to detect subclinical atrial fibrillation in a population at risk: the eHealth-based Bavarian alternative detection of atrial fibrillation (eBRAVE-AF) trial. Am Heart J. 2021;241:26-34. doi:10.1016/j.ahj.2021.06.008
21. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS focused update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in Collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125-e151. doi:10.1161/CIR.0000000000000665
22. Brambatti M, Connolly SJ, Gold MR, et al. Temporal relationship between subclinical atrial fibrillation and embolic events. Circulation. 2014;129(21):2094-2099. doi:10.1161/CIRCULATIONAHA.113.007825
23. Lopes RD, Alings M, Connolly SJ, et al. Rationale and design of the apixaban for the reduction of thrombo-embolism in atients with device-detected sub-clinical atrial fibrillation (ARTESiA) trial. Am Heart J. 2017;189:137-145. doi:10.1016/j.ahj.2017.04.008
24. Attia ZI, Noseworthy PA, Lopez-Jimenez F, et al. An artificial intelligence-enabled ECG algorithm for the identification of patients with atrial fibrillation during sinus rhythm: a retrospective analysis of outcome prediction. Lancet. 2019;394(10201):861-867. doi:10.1016/S0140-6736(19)31721-0
25. Hershman SG, Bot BM, Shcherbina A, et al. Physical activity, sleep and cardiovascular health data for 50,000 individuals from the MyHeart Counts study. Sci Data. 2019;6(1):24. doi:10.1038/s41597-019-0016-7
26. Avram R, Tison GH, Aschbacher K, et al. Real-world heart rate norms in the Health eHeart study. NPJ Digit Med. 2019;2:58. doi:10.1038/s41746-019-0134-9
27. Pluymaekers N, Hermans ANL, van der Velden RMJ, et al. On-demand app-based rate and rhythm monitoring to manage atrial fibrillation through teleconsultations during COVID-19. Int J Cardiol Heart Vasc. 2020;28:100533. doi:10.1016/j.ijcha.2020.100533
28. Jacobs MS, Kaasenbrood F, Postma MJ, van Hulst M, Tieleman RG. Cost-effectiveness of screening for atrial fibrillation in primary care with a handheld, single-lead electrocardiogram device in the Netherlands. Europace. 2018;20(1):12-18. doi:10.1093/europace/euw285
29. Aronsson M, Svennberg E, Rosenqvist M, et al. Cost-effectiveness of mass screening for untreated atrial fibrillation using intermittent ECG recording. Europace. 2015;17(7):1023-1029. doi:10.1093/europace/euv083
30. Chen W, Khurshid S, Singer DE, et al. Cost-effectiveness of screening for atrial fibrillation using wearable devices. JAMA Health Forum. 2022;3(8):e222419. doi:10.1001/jamahealthforum.2022.2419
31. Levin LA, Husberg M, Sobocinski PD, et al. A cost-effectiveness analysis of screening for silent atrial fibrillation after ischaemic stroke. Europace. 2015;17(2):207-214. doi:10.1093/europace/euu213
32. Boriani G, Svennberg E, Guerra F, et al. Reimbursement practices for use of digital devices in atrial fibrillation and other arrhythmias: a European Heart Rhythm Association survey. Europace. 2022;24(11):1834-1843. doi:10.1093/europace/euac142
33. Passman R, Leong-Sit P, Andrei AC, et al. Targeted anticoagulation for atrial fibrillation guided by continuous rhythm assessment with an insertable cardiac monitor: the Rhythm Evaluation for Anticoagulation with Continuous monitoring (REACT.COM) pilot study. J Cardiovasc Electrophysiol. 2016;27(3):264-270. doi:10.1111/jce.12864
34. Passman R. “Pill-in-pocket” anticoagulation for atrial fibrillation: fiction, fact, or foolish? Circulation. 2021;143(23):2211-2213. doi:10.1161/CIRCULATIONAHA.121.053170
35. Tarakji KG, Silva J, Chen LY, et al. Digital health and the care of the patient with arrhythmia: what every electrophysiologist needs to know. Circ Arrhythm Electrophysiol. 2020;13(11):e007953. doi:10.1161/CIRCEP.120.007953
36. Hills MT. Patient perspective: digital tools give afib patients more control. Cardiovasc Digit Health J. 2021;2(3):192-194. doi:10.1016/j.cvdhj.2021.05.001
37. Guo Y, Wang H, Zhang H, et al. Mobile photoplethysmographic technology to detect atrial fibrillation. J Am Coll Cardiol. 2019;74(19):2365-2375. doi:10.1016/j.jacc.2019.08.019
38. Cheung CC, Krahn AD, Andrade JG. The emerging role of wearable technologies in detection of arrhythmia. Can J Cardiol. 2018;34(8):1083-1087. doi:10.1016/j.cjca.2018.05.003
Related Content





