

Clinical Decision to Electrophysiology Procedure: A Standardized Approach
In 2020, more than 360,000 catheter ablation procedures took place in the United States.1 Implantation of cardiac implantable electronic devices has also continued to increase significantly in recent years.2 As electrophysiology (EP) procedures such as these become more prevalent, clinical efficiency within the procedural area is crucial. Herein, we describe our standardized procedure request form to achieve improved outcomes in administrative and clinical efficiency.
Background
Variability of communication among providers in our clinic setting was recently identified as inefficient and inconsistent, with missing information required to schedule procedures. This gap between current and preferred practice was identified as an opportunity for quality improvement (QI) to streamline efficiency, accuracy, and communication, and provide better care to this population of patients. It has been demonstrated that a lack of standardization of scheduling orders can lead to errors, inefficient use of workforce, overuse, and waste.3 Missing information within the procedure order also diminishes the preparedness of the procedural area, leading to delays in preparation of the area for patient-centered delivery of care. A review of the literature reveals that through standardization of communication and orders, the cardiovascular procedural area can be more efficient and prevent delays.3,4
A gap analysis between current and desired best practice demonstrated the need to incorporate technology into the practice. Standardization of the scheduling process in a similar setting such as the cardiac catheterization lab can be successfully implemented and has been demonstrated to improve overall productivity.5-7 A description of the standardization of this process may assist with implementation at other practice sites to improve process efficiency.
Methods
Tools
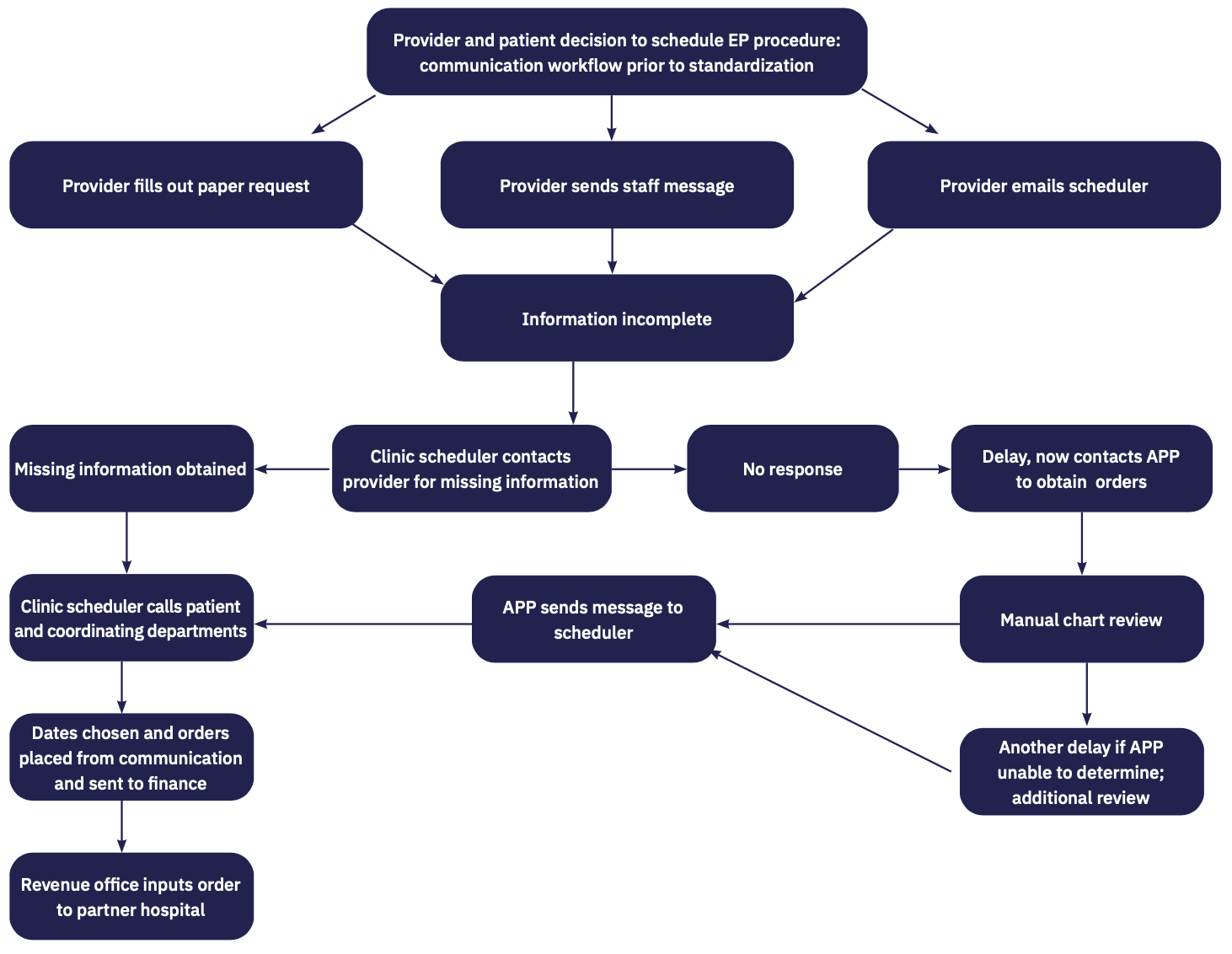
Flowcharts and process mapping were used throughout this process to visually depict the directional mapping of communication and the steps necessary in the clinical scheduling process. In health care, this method has become popular for process improvement.8-10 As we identified common gaps in communication and ordering details in the flowcharts, evidence of the need for change was realized. Gaps were identified as missing or incomplete information as well as multiple communication attempts or steps to obtain a response for unanswered questions in order to complete the order. This missing or omitted information as well as a delay in response repeatedly led to delays in the completion of procedural scheduling, requiring the end user to complete additional steps in order to schedule the procedure. A visualization of these additional steps and work is shown in Figure 1. With the variable process, the clinic schedulers received incomplete or partial orders without the necessary details. This variable process among providers caused delays in patient access to procedures as well as increased work hours for staff due to more time spent acquiring the necessary information to schedule procedures. This increased work and time is avoidable with standardization of the workflow.
As a result of this analysis, our goals in this process were to improve communication by preventing omission of necessary information, and positively impact delivery of care by decreasing the time needed to arrange the procedural day and time with the patient. In addition, our aim was to achieve improved efficiency as evidenced by an increased number of scheduled procedures in the work day as compared to prior variable processes.
Framework, Model, and Design
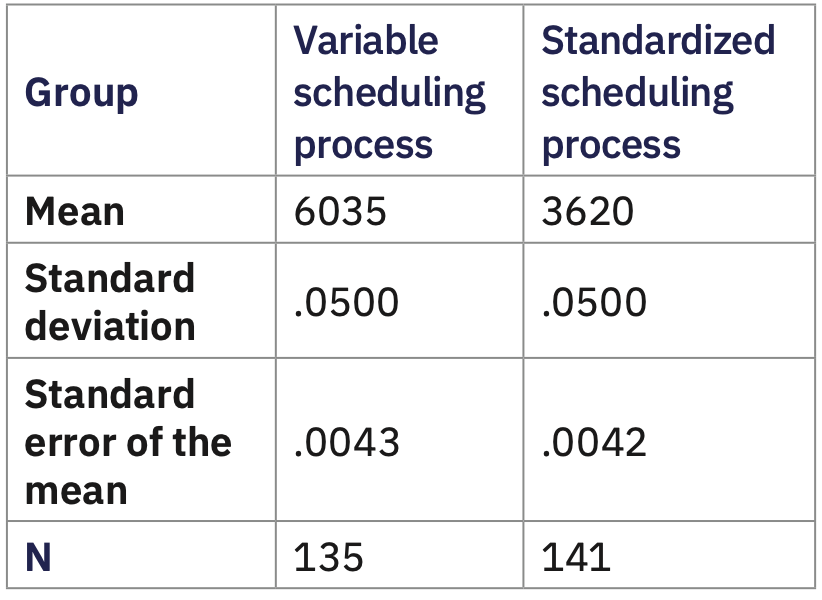
The QI model from the DMAIC process8 was used to Define the current variable process, Measure baseline information, Analyze the current workflow, Identify improvement in the process, and Control the new process once implemented. We analyzed 2 samples: a retrospective, consecutive sample utilizing the current variable process, and a consecutive convenience sample after implementation of the standardized scheduling process. The QI study description and protocol were submitted to the Institutional Review Board and approved for study. Consecutive patients classified as outpatients scheduled to undergo an EP procedure performed by an EP provider in the partner hospital procedural area met inclusion criteria. Collected data was analyzed by the amount of steps and time to accurately schedule the patient in need of an EP procedure. The 2 samples were coded numerically. Consecutively selected sampling based on inclusion criteria prevented sample bias. Patients who changed their decision to proceed with procedure, were not classified as outpatients, and patients who were unable to be reached after more than 2 weeks of attempts (therefore, falling outside of the parameters of this process evaluation) were excluded. The medical record number was associated with a numerical value without further identifying information, and the data was saved on a password-protected database. The time and steps required from decision to schedule the procedure was mapped with flowcharts. The time of clinical decision to schedule the procedure was recorded and the time was recorded upon completion of the scheduling by the clinic schedulers. The retrospective analysis time was recorded at clinic time of decision to proceed and the time was recorded upon completion of the scheduling by the clinic schedulers. Based on criteria, the retrospective sample included 135 patients, and the prospective analysis included 141 patients. The components of the clinic scheduling task included reviewing the block schedule availability, provider availability, patient availability, coordinating necessary departments, COVID-19 testing appointment, and insurance authorization, if necessary. These components were fixed within the 2 samples. After implementation of the standardized process, a statistical difference measured by independent t test was realized. This difference demonstrated improved efficiency measured in time and quantity.
In addition to the DMAIC model, the Change Theory of Nursing provided a structural framework for process improvement.11 Application of this theory has shown to be effective when adopting a new practice, even in well-entrenched processes.11,12
Process Implementation
The provider or delegate first enters the prepopulated order set with “hard stops” defined by required necessary procedural information during the patient encounter in the electronic health record (EHR) to the scheduler work queue. The inclusion of all necessary information prevents an unnecessary delay in scheduling, and therefore, a delay in procedure. The required information must be entered to transmit directly to the work queue. Upon receipt of order, available time and dates in block scheduling and provider availability are coordinated with other necessary services or departments, and financial approval is obtained. This process is performed in the shared EHR between the clinic and partner hospital. The implementation of a standardized process is paramount for patient safety; it eliminates duplication of information gathering and ensures accurate and crucial information is included.4 Communication through text, email, or paper was eliminated.
As with any change process, there were challenges to progress. Internal threats included fear of change, disruption of familiar practice patterns, awareness of new processes, and variability of providers and staff, as well as lack of awareness of this change. Reinforcement was necessary to prevent staff from reverting to a variable process. Initial concerns with time constraints and perception of additional work within the visit were voiced prior to implementation. Additional constraints to implementation included a national pandemic and ongoing demands for advanced technology assistance. There was also an initial delay of implementation, as our information technology (IT) department did not originally have the resources to implement this project due to prioritization of other projects. Strategic collaboration with IT, process engineering, stakeholders, operations across both organizations, and the chief of operations, was necessary to implement this process change.
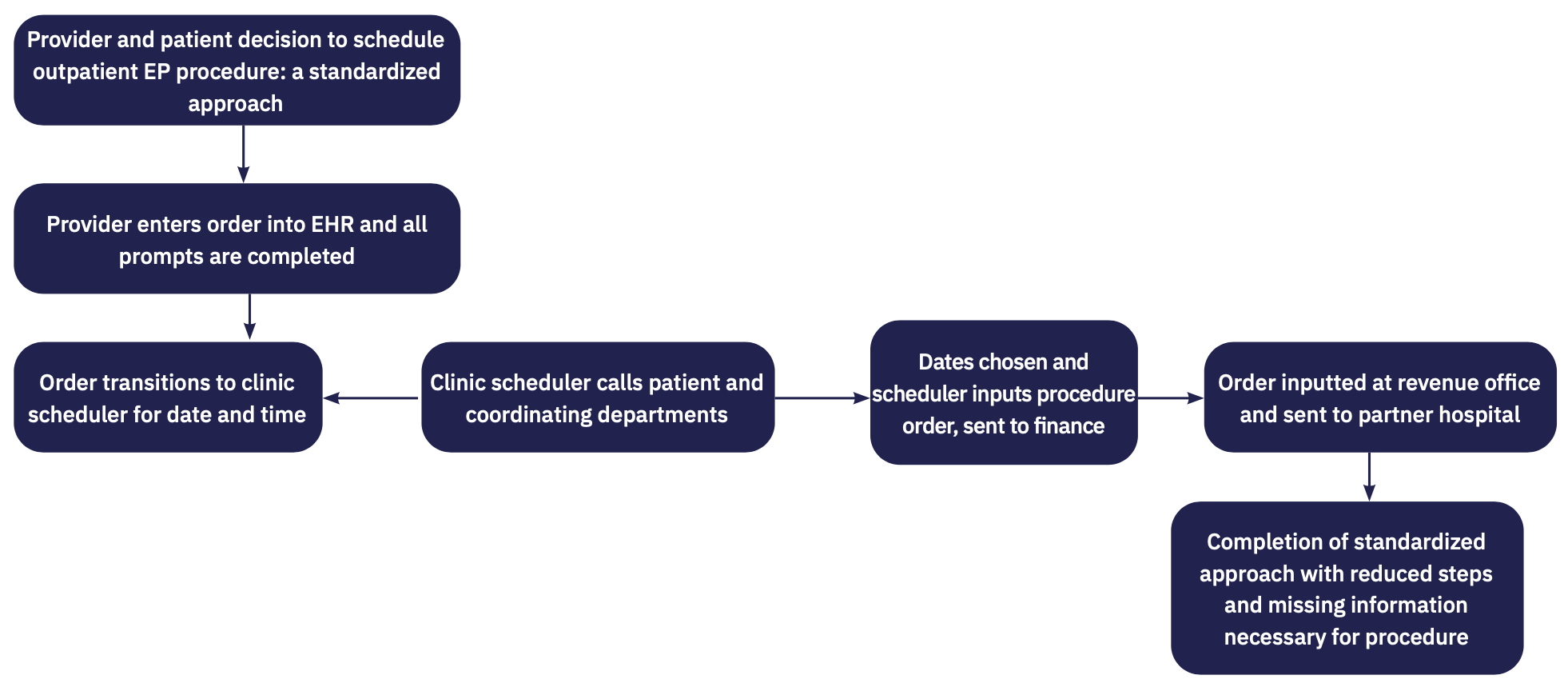
This process change utilized the existing, updated inpatient order sets for scheduling of EP procedures and extended access to the clinic setting. As discussed, a standardized approach can benefit patient care, enhance communication with providers, and improve clinical operations through reduced work time and decreased cost. Through implementation of this new approach, the staff, equipment, and patient environment are now safely prepared. This process streamlined the timely delivery of specialized procedural setup, which is now patient centered and ensures effective preparedness of the patient, staff, and procedural area with regard to equipment availability (Figure 2).
Historically, missing information needed by schedulers to complete the procedure order for this patient population would delay the scheduling of approximately 3-6 patients per week. Improved communication and more precise information allows for the optimization of staff, environment, and provider utilization by identifying the patient needs for each procedure.5 Timely and accurate communication ensures the team, equipment, and environment are safely and effectively prepared in advance of the patient arrival.
Results
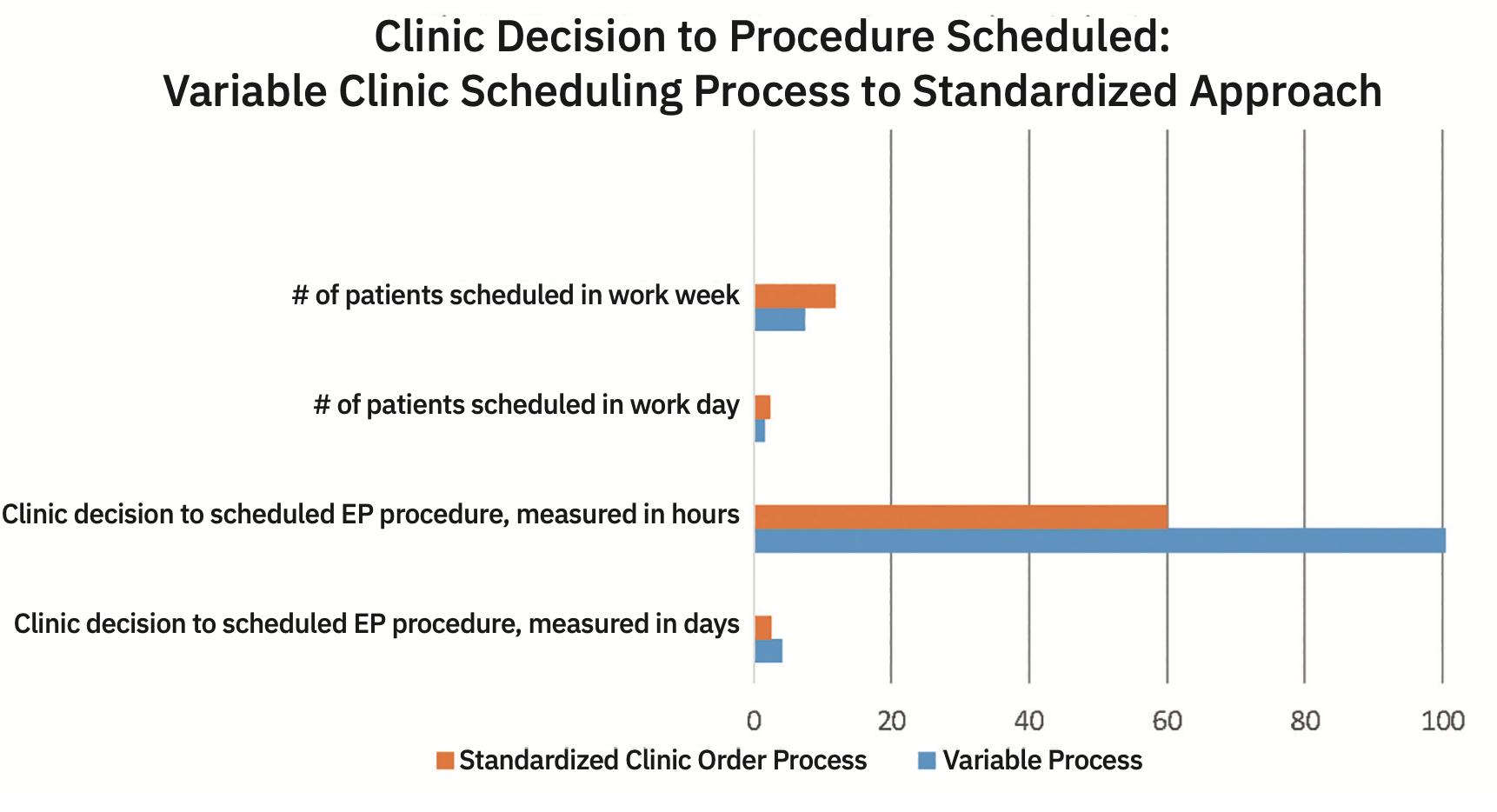
A total of 276 reviewed procedures met criteria for inclusion. This included 135 retrospective and 141 prospective procedures. We found by using this standardized process, clinic schedulers were able to decrease the time needed to complete planned procedures by almost 40%. This outcome exceeded our expected reduction of 20%. The minimum time to schedule patient procedures at clinic decision decreased from 92 minutes to 32 minutes. The average time to complete the scheduling process decreased from 6035 minutes to 3620 minutes. The maximum time decreased from 66201 minutes to 23147 minutes. P value is significant at less than .0001. Procedure quantity scheduled in 11 weeks increased to 141 procedures compared to 101, a difference of 40 procedures during the same number of weeks. Prior to standardization, 5 or more procedures in a day were scheduled during 1.5% of workdays. After implementation of the standardized process, 5 or more procedures were scheduled during 11.9% of the workdays. The process change realized almost a tenfold difference (Figure 3).
Significance and Implications
The two-tailed P value is statistically significant at <.0001.The CI is 95% from 2414.9882 to 2415.0118, t=400352.6793. The standard error of difference is .006.
Discussion
Implementation of a standardized order set incorporated into the EHR resulted in a 40% reduction in time from clinical decision to scheduling of procedure. Our schedulers were surveyed after implementation and reported improved overall workflow secondary to improved communication and completeness of information. This was appreciated by a decreased time to complete the scheduling process, allowing the ability to schedule more patients in a day. It should also be noted that during the standardized process, additional responsibilities were added to the clinic scheduler’s job description requiring time outside of scheduling that may have diminished the impact, although quite significant.
Conclusion
In this article, we shared our approach to standardizing the procedure request form to help achieve improved outcomes in administrative and clinical efficiency. A standardized approach can be beneficial for the patient, organization, and partner hospital. Through elimination of omitted information, a standardized process with increased efficiency and improved productivity was realized, resulting in a 40% decrease in time from clinical decision to scheduling of procedure.
Acknowledgements. We would like to thank Guilherme Oliviera, MD, MBA, executive director of the Tampa General Hospital (TGH) Heart & Vascular Institute and professor and chief of division of Cardiovascular Sciences at the University of South Florida (USF) Health Morsani College of Medicine; Bengt Herweg, MD, medical director of the TGH Electrophysiology Center of Excellence as well as professor and cardiologist at the USF Health Morsani College of Medicine. We would also like to thank Nicholas Kotch, DO; David Wilson, MD; schedulers Yvette Cartagena and Diane Randolph for their keen awareness and assistance in identifying areas for improvement; Nishit Patel, MD, FAAD, chief medical information officer; and system analysts Danielle Litowchak and Danielle Lanier for their assistance in implementing the much-needed technology to successfully complete this quality improvement project initiative. We also want to thank the faculty at USF for their input and mentorship, including Tracey Taylor, DNP, ACNP-BC, RN, and Christina Cardy, DNP, AGACNP-BC.
Disclosures: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Ms Wicks and Ms Taylor have no conflicts of interest to report regarding the content herein.
References
1. U.S. EP labs losing $500 million each year due to underutilized reprocessing programs. Innovative Health. Published June 10, 2020. Accessed March 1, 2022. https://www.hmpgloballearningnetwork.com/site/eplab/us-ep-labs-losing-500-million-each-year-due-underutilized-reprocessing-programs
2. Greenspon AJ, Patel JD, Lau E, et al. 16-year trends in the infection burden for pacemakers and implantable cardioverter-defibrillators in the United States 1993 to 2008. J Am Coll Cardiol. 2011;58(10):1001-1006. doi:10.1016/j.jacc.2011.04.033
3. Thieret D, Clark E, Carbaugh DL. Electronic forms trump paper for surgical scheduling. Nursing. 2015;45(10):16-18. doi: 10.1097/01.NURSE.0000471424.57377.52
4. Kitz-Torpey D, Murphy M, Skipitaris N. Process for improving efficiency: experience from the EP team at Lenox Hill Hospital. EP Lab Digest. 2016;16(12):1,6-8.
5. Rodriguez Martinez C, Gonzalez Aleu F, Granda EMA, Nadeem SP. Quality improvement projects in catheterization laboratories: a systematic literature review. Proceedings of the International Conference on Industrial Engineering and Operations Management. Published online March 10, 2020. http://www.ieomsociety.org/ieom2020/papers/224.pdf
6. Reed GW, Hantz S, Cunningham R, et al. Operational efficiency and productivity improvement initiatives in a large cardiac catheterization laboratory. JACC Cardiovasc Interv. 2018;11(4):329-338. doi:10.1016/j.jcin.2017.09.025
7. Agarwal S, Gallo JJ, Parashar A, et al. Impact of lean six sigma process improvement methodology on cardiac catheterization laboratory efficiency. Cardiovasc Revasc Med. 2016;17(2):95-101. doi:10.1016/j.carrev.2015.12.011
8. The define, measure, analyze, improve, control DMAIC Process. American Society for Quality (ASQ). ASQ.org. Accessed March 1, 2022. https://asq.org/quality-resources/dmaic
9. Quality improvement essentials toolkit. Institute for Healthcare Improvement (IHI). Published 2017. Accessed March 1, 2022. http://www.ihi.org/resources/Pages/Tools/Quality-Improvement-Essentials-Toolkit.aspx
10. Anderson-Dean C. The benefits of lean six sigma for nursing informatics. The Free Online Library. Published December 22, 2012. Accessed March 1, 2022. https://www.thefreelibrary.com/The+benefits+of+Lean+Six+Sigma+for+nursing+informatics.-a0339637788
11. Lewin’s change theory. Nursing Theory. Published 2016. Accessed March 1, 2022. https://nursing-theory.org/theories-and-models/lewin-change-theory.php
12. Hussain ST, Lei S, Akram T, et al. Kurt Lewin’s change model: a critical review of the role of leadership and employee involvement in organizational change. J Innovation & Knowledge. 2018;3(3):123-127. doi:10.1016/j.jik.2016.07.002

