

Incorporating Advanced Intracardiac Signal Information Into the Clinical Workflow: Interview With G. Joseph Gallinghouse, MD
 In this feature interview, EP Lab Digest speaks with Dr. Gallinghouse to discuss his use of and thoughts on the PURE EP™ System (BioSig Technologies, Inc.), including workflow integration, improved signal technology, and recent study results at Texas Cardiac Arrhythmia Institute (TCAI) at St. David’s Medical Center in Austin, Texas.
In this feature interview, EP Lab Digest speaks with Dr. Gallinghouse to discuss his use of and thoughts on the PURE EP™ System (BioSig Technologies, Inc.), including workflow integration, improved signal technology, and recent study results at Texas Cardiac Arrhythmia Institute (TCAI) at St. David’s Medical Center in Austin, Texas.
Please tell us a little about your practice.
In 1997, I completed my EP fellowship training at the University of California San Francisco, under the direction of Dr. Mel Scheinman. I have been practicing at TCAI in Austin for the past 20 years. As TCAI has grown and evolved over the years, several of our physicians have developed subspecialty areas of interest. For me, that has been complex atrial arrhythmia management. The majority of my time in the lab these days involves ablation of atrial fibrillation (AF), atrial flutters, and the various varieties of supraventricular tachycardias (SVT). I feel so fortunate to have been in clinical practice just as we were developing a better understanding of the AF substrate. Since Michel Haïssaguerre’s landmark study first published in 1998 demonstrated the importance of the pulmonary veins in AF, many of us from that era have been on a mission to eradicate the drivers, and a lot of us jokingly refer to the early days as “learning by burning.” It has really been amazing to witness the technological advancements in the field since the late 1990s, with 3D mapping systems, intracardiac ultrasound, and irrigated force-sensing catheters. But not much attention has been given to the most basic component of any invasive electrophysiology study: the accurate recording and display of the intracardiac electrogram. That is where PURE EP™ has filled a major gap for us.
Results from the PURE EP 2.0 study, in which you were an investigator, were recently published in the Journal of Cardiovascular Electrophysiology.1 Can you recap the key study findings?
This was a multicenter, prospective study of a new signal processing platform. Intracardiac signal data of clinical interest were collected at the same timestamps from 51 patients who underwent ablation procedures with PURE EP™, the conventional recording system, and the 3D mapping system. Those samples were randomized and subjected to a blinded evaluation by three independent electrophysiologists to determine the clinical utility and quality of PURE signals when compared to conventional sources of intracardiac signals. Each reviewer assessed the same signal sets and responded to questions using a 10-point rating scale. If two or more of the reviewers rated the PURE EP™ signal higher than the control, it was judged as superior.
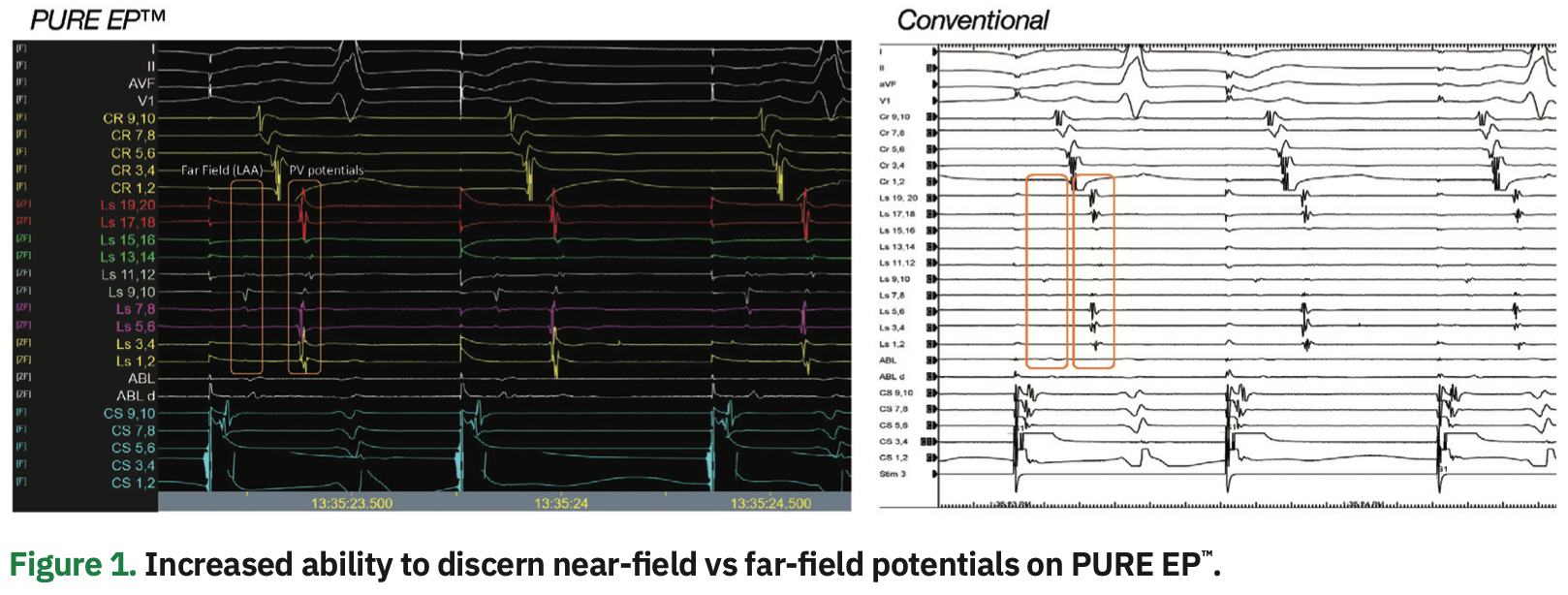
The main takeaway was that the study validated the clinical relevance and quality of the PURE EP™ signals over conventional signal sources. There was a 93% consensus in responses from the blinded EP reviewers. They deemed signals from the PURE EP™ System as having a cumulative 75% superiority in signal quality and physician confidence. There was an 83% improved confidence in interpreting near-field versus far-field signal components, and a 73% improvement in visualization of small, fractionated signals of clinical importance.
What is your perspective of these findings in your personal EP practice?
The study results show that PURE EP™ provides the most accurate physiologic signal information available for use during our ablation procedures. We get higher fidelity visualization of the intracardiac signals without issues associated with signal saturation and noise, which is so common in the EP lab. In addition, with PURE EP™, we don’t see the usual problematic artifact such as ringing, which is caused by over-filtering in conventional systems and can be misleading.
Now that you’ve been using the PURE EP™ technology for about two years, how do you incorporate the improved signal information into your clinical workflow?
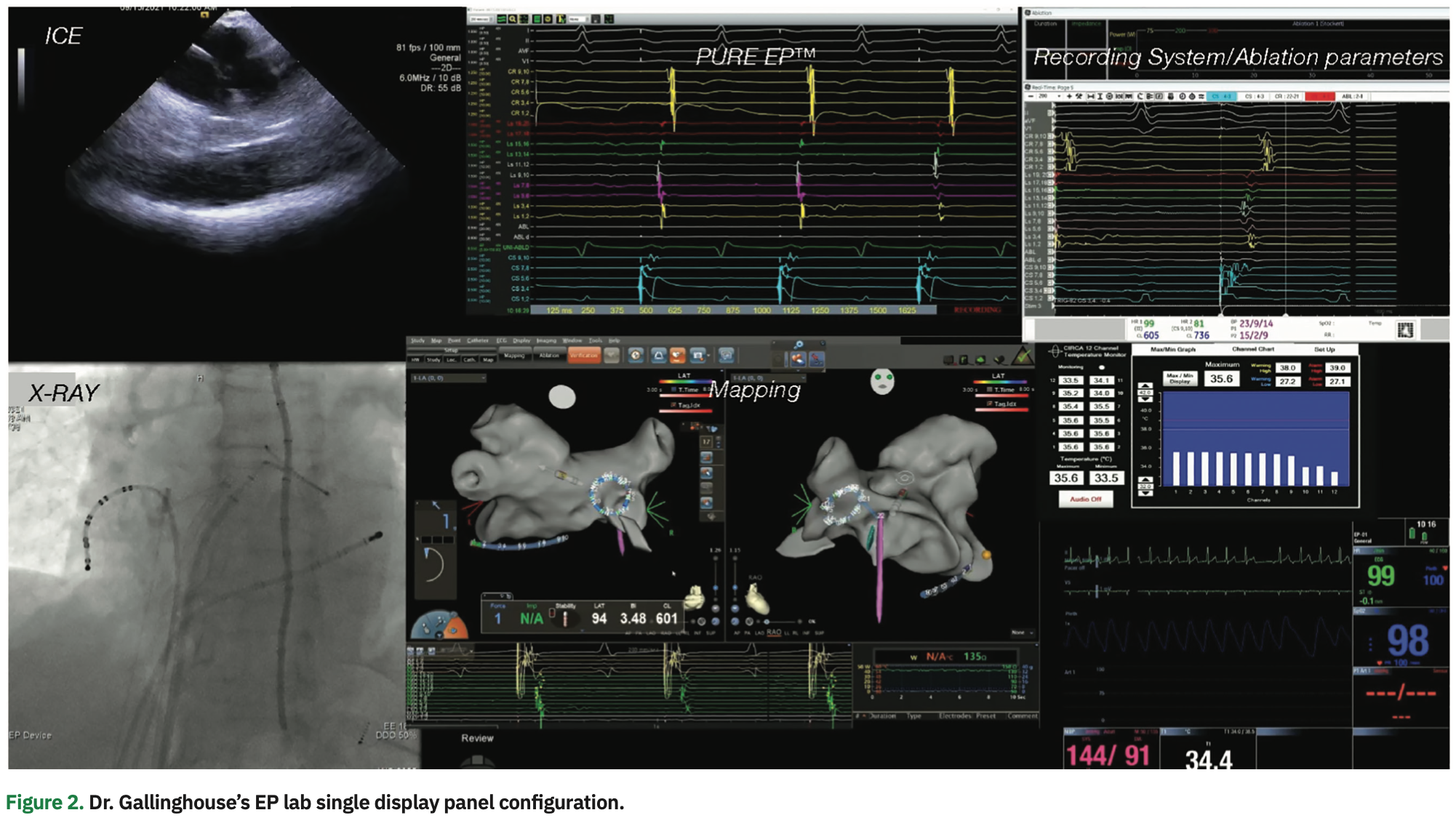
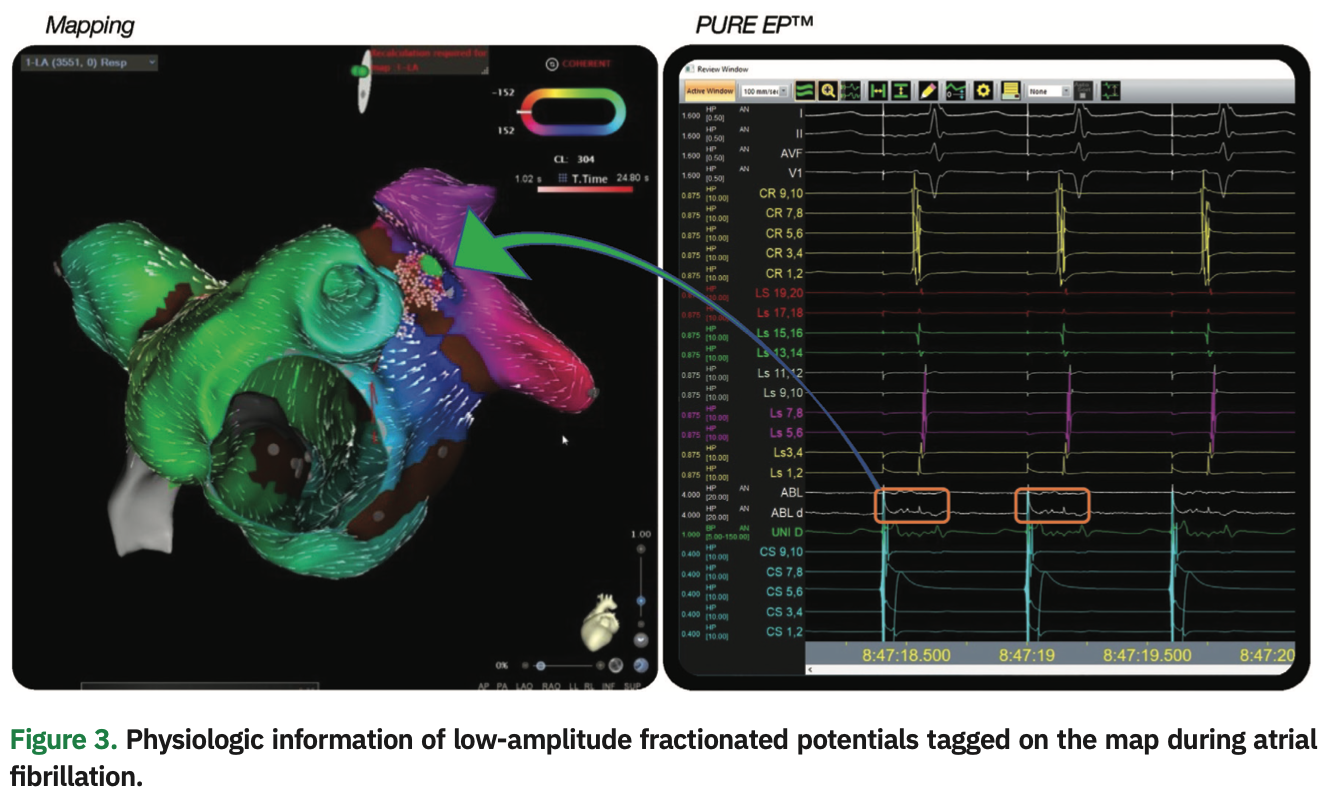
We’ve made PURE EP™ signals central to our workflow, and it has become the primary source of physiologic signal information. For our setup, we have visualization of two screens: the PURE EP Live window and the 3D mapping window. Since it is essential to clearly discern small, fractionated signal potentials to effectively treat complex arrhythmia substrates, the focus is on the PURE EP window. We enhance the 3D map by tagging small, fractionated signals seen on PURE EP™, which we consider critical to the case. Overall, PURE EP™ enhances our interpretation of the 3D map and allows more precise treatment of ablation targets.
What do better signals mean for physicians and the patients they treat?
I’m very excited that we finally have what I consider to be a major technological enhancement in one of the most important areas of interventional cardiac electrophysiology. High-quality signal acquisition is central to any ablation procedure, and absolutely mission critical for many of our cases. Over the past several years, other technological advances such as improved mapping systems, force-sensing ablation catheters, and intracardiac echo, have allowed us to successfully tackle more challenging arrhythmia substrates. But as we’ve discussed, the most complex arrhythmias often have important small, high-frequency, low-amplitude potentials that are difficult to discern with current mapping and recording systems. Those signals, when they’re tagged and incorporated into the 3D electroanatomical map, help us better understand the circuit or arrhythmia focus, and identify areas that require ablation therapy.
What is your opinion of the potential impact of the PURE EP™ technology on ablation procedure outcomes and efficiency?
The ability to accurately identify these high-frequency, low-amplitude signals has definitely made my procedures more efficient. With PURE EP™, I can quickly identify important areas to target for more accurate ablation. It hasn’t yet been evaluated in a formal clinical trial, but I suspect PURE EP™ can lead to shorter procedure times and improved ablation efficacy, particularly for the most complex arrhythmia substrates. The bottom line is that electrophysiologists always want cleaner and more accurate signal recordings, and I’m frankly amazed that more effort hasn’t been made to achieve this over the years. Hopefully, moving forward, we’ll find ways to automatically incorporate PURE EP™ signals into the 3D anatomical mapping systems. I think that would be a major next step.
This article is published with support from BioSig Technologies, Inc.
Disclosures: Dr. Gallinghouse reports consulting fees from BioSig Technologies, Inc., and Biosense Webster.
Reference
1. Al-Ahmad A, Knight B, Tzou W, et al. Evaluation of a novel cardiac signal processing system for electrophysiology procedures: the PURE EP 2.0 study. J Cardiovasc Electrophysiol. 2021;32(11):2915-2922. Epub 2021 Oct 1. doi: 10.1111/jce.15250

