

Intracardiac Echocardiography-Guided Left Atrial Appendage Occlusion Procedures: Initial Experience, Workflow, and Other Considerations
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2024;24(7):12-15.
Sanjaya Gupta, MD, MBA, and Chetan Huded, MD, MSc, Saint Luke’s Mid-America Heart Institute, Kansas City, Missouri
Left atrial appendage occlusion (LAAO) has been performed since 2002 in clinical trials and was approved in 2015 by the United States Food and Drug Administration. Patients have predominantly undergone LAAO with the Watchman (Boston Scientific) and Amplatzer Amulet (Abbott) devices, but several other investigational LAAO devices are being evaluated in clinical trials, and the annual number of LAAO procedures has steadily increased in recent years. Throughout this time, the main imaging modality for LAAO has been transesophageal echocardiography (TEE), which usually requires both general anesthesia with endotracheal intubation as well as a second physician to perform TEE.
Interest in using intracardiac echocardiography (ICE) as an alternative to TEE originally emerged out of necessity when a TEE probe could not be passed down a patient’s esophagus due to stricture or anatomic anomaly. Other centers electively adopted ICE-guided LAAO to obviate the need for a second physician to perform TEE.1 An additional benefit is the ability to perform LAAO procedures under conscious sedation to facilitate faster patient recovery for elderly patients who may have a difficult time with general anesthesia. Several studies have validated the safety and efficacy of LAAO with ICE guidance compared to standard TEE and have found comparable results.2-4 Some studies demonstrated a reduction in procedural time and in-room time.5 The recently completed SURPASS registry compared 39,759 LAAO procedures with TEE vs ICE guidance. There was a high success rate of LAAO with both TEE and ICE guidance with no significant difference in rate of successful device placement or rate of incomplete seal between the ICE and TEE. While most adverse event rates were similar between TEE and ICE guidance, there was a slightly higher rate of pericardial effusion with ICE guidance compared to TEE.6
With the advent of live 3-dimensional (3D) ICE (also known as 4D ICE) imaging, it is thought that this may provide a sufficient level of imaging quality that may facilitate broader adoption of ICE as an alternative to TEE for LAAO procedures. Standard 2-dimensional (2D) ICE consisted of a phased array ultrasound transducer on the tip of a catheter capable of a single-plane live image. A live 3D (or 4D) ICE consists of a matrix of phased array transducers that facilitate multiplanar reconstruction (MPR) of multiple different angles to generate a live 3D image. Available ICE catheters fundamentally operate on this same principle. In this article, we discuss our initial experience in developing a workflow for ICE-guided LAAO procedures.
Choosing a Catheter
Currently commercially available 3D/4D ICE catheters include the VeriSight Pro (Philips), NUVISION (Biosense Webster, Inc, a Johnson & Johnson company), and ACUSON AcuNav Volume 4D ICE (Siemens Healthineers).
The decision about which catheter to pursue should be based on several factors, including catheter maneuverability, image resolution, support by clinical staff, and cost. Another consideration is the type of imaging platform used at the institution, and if a new imaging console will need to be purchased to accommodate a compatible catheter.
When considering which catheter to acquire and whether to integrate 3D ICE into the LAAO workflow, it is recommended to conduct an evaluation in conjunction with the imager who performs TEE. Set aside a day with a manageable volume of relatively straightforward cases. Attend a hands-on demonstration or spend time with an ICE simulator prior to the first case. During the procedure, try to perform as much of the procedure as possible with 3D ICE and use TEE to verify the position of the transseptal puncture and the final measurements of the LAAO device.
Our Initial Experience
We began performing ICE-guided LAAO procedures several years ago using 2D ICE catheters. These procedures were primarily for patients in whom TEE could not be performed. Having gained that initial experience with the procedural workflow, we were excited to integrate 3D ICE over the past year as the technology has become more accessible. Since June 2023, we have performed approximately 20-25 cases of 3D ICE-guided LAAO procedures. We have trialed each of the 3 commercially available 3D ICE catheters listed here, and each of the catheters can provide high-quality images to guide LAAO. The specific catheter that a program ultimately chooses may vary based on local factors.
During our early experience with 3D ICE-guided LAAO, we utilized both TEE and ICE concomitantly for several reasons. First, incorporating both TEE and ICE is helpful to engage the cardiac imaging team in the process. Rather than using 3D ICE to remove the imager from the procedure, we have aimed to include our imaging colleagues in the process and rely on their expertise when incorporating this new technology. A skilled imager adds immense value to a 3D ICE-guided case by optimizing the image acquisition and 3D multiplanar reconstructions. Second, concomitant use of TEE and 3D ICE allows for a stepwise transition to ICE-only cases. For example, as we became more comfortable with 3D ICE, we would perform the entire procedure under ICE and use TEE only as a final check before device release.
There are numerous imaging objectives during an LAAO procedure: evaluation of baseline cardiac anatomy, guidance of transseptal puncture, evaluation for baseline LAA thrombus, guidance of the delivery sheath into the LAA, positioning of the device in the LAA, evaluation of release criteria such as PASS or CLOSE criteria for Watchman and Amulet, respectively, and assessing for pericardial effusion. Once we were comfortable with performing each of these objectives with 3D ICE, we began performing 3D ICE only procedures for selected patients.
Programs may have different visions for the optimal use of 3D ICE in LAAO. While some programs are seeking to adopt ICE as the default imaging modality for LAAO, we view 3D ICE and TEE both as valuable approaches to guide LAAO. While 3D ICE-guided LAAO is a great option for patients with straightforward LAAO anatomy and reasons to forego general anesthesia, TEE-guided closure remains a safe and effective procedure for many patients, especially those with complex anatomy. Our goal is to be facile with both modalities so that we can offer each patient the best procedure for them.
Workflow for ICE-Guided LAAO Procedures
There are several workflow considerations for ICE-guided LAAO procedures. First, prior to the procedure, it is helpful to get a CT angiogram of the LAA to confirm there is no thrombus and to allow visualization of the anatomy and orientation, facilitating preprocedural planning. When developing workflow for ICE-guided procedures, preplanning will help in selecting appropriate cases using ICE for guidance. The ICE catheter requires a dedicated sheath, typically a 9 French (F) to 13F size sheath depending upon the catheter. To minimize complications, venous access for both the LAAO access sheath and ICE catheter sheath should be obtained under ultrasound guidance and/or utilizing a micropuncture venous access kit. If a suture-mediated closure device is planned, it may be beneficial to deploy that device after access and before the vessel is dilated with a large-bore sheath. Some operators prefer to have both access in the same groin to facilitate easier manipulation of both the LAAO sheath and ICE catheter by a single operator. Other operators may want to have an assistant help with the ICE catheter, and therefore, may obtain access in bilateral femoral veins and place the sheath for the ICE catheter in the left femoral vein.
Typically, the ICE catheter is advanced initially through the venous system into the right atrium (RA) without fluoroscopy by always visualizing an echo-lucent space in front of the ICE catheter. Once the catheter is in the RA, the home view is obtained with the RA, right ventricle, tricuspid valve, and aorta visualized (Figure 1, Video 1). It is recommended to initially deflect the catheter across the tricuspid valve and then rotate the catheter clockwise to visualize the left ventricle. This is done to establish a baseline for pericardial effusion at the beginning of the case that can be repeated at the end of the case or if there is an unexpected change in blood pressure during the procedure (Figure 2, Video 2). From the right ventricle, if the ICE catheter is rotated clockwise as it is withdrawn, the pulmonary artery becomes visible. If the ICE catheter is gently advanced into the pulmonary artery to the level of the pulmonic valve and then rotated slightly, the LAA is visible. This can be useful to ensure the LAA is clear of thrombus before transseptal catheterization is performed. The ICE catheter is then returned to the home view in the RA and rotated clockwise until the LA and interatrial septum are visualized. The LAAO sheath is advanced to the superior vena cava over a guidewire. Preparations are then made to perform transseptal catheterization. One of the advantages of the 4D ICE catheters is the ability to obtain contralateral views (ie, x-plane) to visualize the interatrial septum in short and long axis, as can be done with TEE. This facilitates precisely positioning the transseptal system in the superior-inferior axis as well as in the anterior-posterior axis at the same time (Figure 3, Video 3). Once transseptal catheterization is performed and the LAAO sheath is advanced into the LA, it is recommended to withdraw the LAAO sheath over the wire back to the RA to facilitate placement of the 4D ICE catheter in the LA. This is done by deflecting the ICE catheter toward the interatrial septum and rotating the catheter to keep the guidewire in view. Once the ICE catheter tip is confirmed to be at the interatrial septum and immediately adjacent to the guidewire, the ICE catheter can be gently advanced across the interatrial septum into the LA. Finally, the LAAO sheath can be advanced into the LA again over the guidewire.
Once the 4D ICE catheter is in the LA, there are several positions where the ICE catheter can be placed to visualize the LAA. The most common initial position is in the mid LA with a slight retroflexion and counterclockwise rotation to properly visualize the LAA. This view is similar to the 90° TEE view and facilitates baseline measurements of the ostial diameter and depth of the appendage (Figure 4, Video 4). This view is also useful to confirm the LAA is free of thrombus, if this had not been done prior to transseptal catheterization. Additional views include placing the ICE catheter in the left superior pulmonary vein and along the lateral mitral annulus, which correspond to the 45° and 135° views, respectively.
Of note, since the LAAO sheath and ICE catheter are in the same chamber, care must be taken when manipulating the ICE catheter to always keep a safe distance from the LAAO sheath and device. In addition, it is important to always see an echo-lucent space in front of the ICE catheter at all times to prevent traumatizing any cardiac structures. The presence of the ICE catheter in the LA does not change the existing recommendations for target ACT range for heparin anticoagulation.
The initial positioning of the LAAO sheath in the appendage (Figure 5, Video 5), the deployment of the LAAO device, the tug test (Figure 6, Video
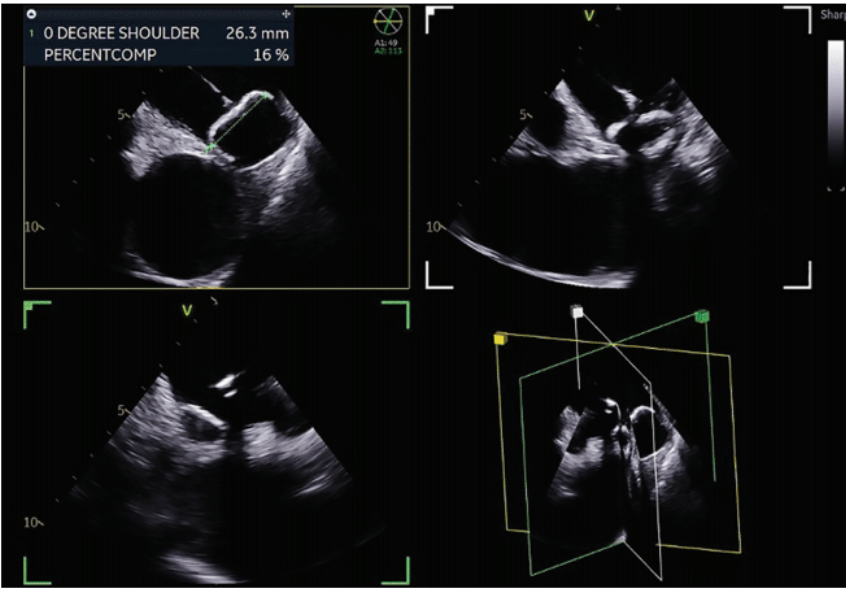
6), the measurements for compression (Figure 7), and the assessment for possible flow around the device (Figure 8, Video 7) can all be done in the 2D ICE views in a similar manner as TEE. All the available 4D ICE catheters allow for MPR to create a live 3D image that may be helpful in navigating a challenging anatomy or to provide additional perspective on the size and shape of the LAAO device in the appendage (Figure 9, Video 8). Once the device is deployed and both the LAAO sheath and ICE catheter are returned to the RA, the final step is to return the ICE catheter to the right ventricle and confirm the absence of any significant pericardial effusion. Once catheters are removed from the body, use of a closure device or a subcutaneous figure-of-8 suture is recommended to facilitate faster patient recovery.
Other Considerations
It is important to also note the disadvantages of utilizing 4D ICE for LAAO. It requires a second large-bore venous access, which has its own inherent risks. The operator is responsible for both acquiring images and performing the procedure unless staff can be trained to acquire images or a second operator is used.
While the image quality is excellent for available ICE catheters, it cannot exceed the resolution of TEE. The cost of 4D ICE catheters can be significant and the catheters are not capable of being reprocessed at the present time.
These disadvantages may be outweighed by the potential for greater procedural efficiency and reduced need for a second physician to perform TEE by performing LAAO with 4D ICE. This may allow for cases to be performed under moderate sedation instead of general anesthesia, which may facilitate faster recovery, shorter overall procedural time, and reduced cost per case. These projected cost savings and potential increase in procedural volume may offset costs as compared to TEE. If the opportunities created by freeing up an anesthesiologist and structural echocardiographer to perform additional procedures are also considered, then there may be significant benefit to the institution to perform LAAO with 4D ICE.
Conclusion
The use of 4D ICE catheters for LAAO procedures holds tremendous promise for improved efficiency and decreased overall resource utilization that may justify the expense of the catheter. The process of acclimating to a 4D ICE workflow will occur at a different pace for each operator and it is important to be patient and work with imaging staff to become familiar with this workflow and ensure best patient outcomes.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest, and report no conflicts of interest regarding the content herein. Dr Gupta consulting fees from Medtronic and Boston Scientific, and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Medtronic, Boston Scientific, and ZOLL Respicardia. Dr Huded reports consulting fees from Medtronic and Boston Scientific.
References
1. Alkhouli M, Chaker Z, Alqahtani F, Raslan S, Raybuck B. Outcomes of routine intracardiac echocardiography to guide left atrial appendage occlusion. JACC Clin Electrophysiol. 2020;6(4):393-400. doi:10.1016/j.jacep.2019.11.014
2. Berti S, Pastormerlo LE, Santoro G, et al. Intracardiac versus transesophageal echocardiographic guidance for left atrial appendage occlusion: the LAAO Italian multicenter registry. JACC Cardiovasc Interv. 2018;11(11):1086-1092. doi:10.1016/j.jcin.2018.05.008
3. Gianni C, Horton RP, Della Rocca DG, et al. Intracardiac echocardiography- versus transesophageal echocardiography-guided left atrial appendage occlusion with Watchman FLX. J Cardiovasc Electrophysiol. 2021;32(10):2781-2784. doi:10.1111/jce.15220
4. Turagam MK, Neuzil P, Hala P, et al. Intracardiac echocardiography-guided left atrial appendage closure with a novel foam-based conformable device: safety and 1-year outcomes. JACC Clin Electrophysiol. 2022;8(2):197-207. doi:10.1016/j.jacep.2021.10.001
5. Diaz JC, Bastidas O, Duque M, et al. Impact of intracardiac echocardiography versus transesophageal echocardiography guidance on left atrial appendage occlusion procedures: a meta-analysis. J Cardiovasc Electrophysiol. 2024;35(1):44-57. doi:10.1111/jce.16118
6. Ferro EG, Alkhouli M, Nair DG, et al. Intracardiac vs transesophageal echocardiography for left atrial appendage occlusion with Watchman FLX in the US. JACC Clin Electrophysiol. 2023;9(12):2587-2599. doi:10.1016/j.jacep.2023.08.004
Figure 1/Video 1.
Home view on ICE with VeriSight Pro (Philips). RA = right atrium; RV = right ventricle; Ao = Aorta.
Figure 2/Video 2.
View of left ventricle from right ventricle with trace pericardial effusion visible, using NUVISION catheter (Biosense Webster, Inc, a Johnson & Johnson company).
Figure 3/Video 3.
X-plane view of long axis of fossa ovalis (left pane) with the superior aspect of the interatrial septum on the right side of the image and inferior aspect on the left side, using the NUVISION catheter (Biosense Webster, Inc, a Johnson & Johnson company). The short axis of the fossa is shown on the right pane with the aorta and anterior aspect shown on the right side of the image and posterior aspect shown on the left side of the image.
Figure 4/Video 4.
View from mid LA with slight retroflexion, similar to 135° TEE view, using VeriSight Pro (Philips). The mitral valve is on the left side of the screen.
Figure 5/Video 5.
Initial positioning of the LAAO sheath in the LAA in a multiplanar view, using NUVISION catheter (Biosense Webster, Inc, a Johnson & Johnson company).
Figure 6/Video 6.
Using VeriSight Pro (Philips), tug test showing Watchman FLX (Boston Scientific) elongating and returning to original shape without moving.
Related Content





