

Current and Future Perspectives on Left Atrial Appendage Occlusion
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2023;23(7):13-16.
Atrial fibrillation (AF) remains a major cause of stroke and disability. The management of stroke prevention using anticoagulation with warfarin, the previous hallmark of therapy, proved to be difficult to control. Direct oral anticoagulants (DOACs) then surpassed warfarin as the primary first-line option to prevent thrombus formation in the left atrial appendage (LAA). However, DOACs also have bleeding complications and a significant cohort of patients are ineligible for anticoagulation. This led to the evolution to left atrial appendage occlusion (LAAO). The advent of LAA closure started with surgical ligation, transitioned to attempts at epicardial closure, and has since expanded to endocardial LAAO. In this review, we focus on endocardial LAAO, approach and decision-making, current advances, and future perspectives.
Shared Decision-Making
There are 2 FDA-approved LAAOs in the United States. The Watchman device (Boston Scientific) was approved in 2015, and the Amplatzer Amulet LAAO (Abbott) was approved in 2021. Both devices are used to close off the LAA from the systemic circulation. The Watchman device seals off the distal body of the LAA, while the Amulet device lobe is placed within the LAA, and the disc seals the orifice.
Patient selection for LAAO depends on a CHADS2 score of 2 or CHA2DS2-VASc score of 3 or higher as well as those who are at high risk of bleeding. The decision to implant a LAAO device starts in the cardiology clinic. The Centers for Medicare & Medicaid Services (CMS) requires a nonimplanting physician to document a shared decision-making interaction using an evidence-based decision tool.1 Patient decision aids (PDA) are available through the American College of Cardiology at CardioSmart.org.2 While there is significant data on the benefits of shared decision-making, cardiologists are often not formally trained. For example, when queried on shared decision-making practices, cardiologists did not perceive a benefit of using PDAs.3
It is worth revisiting what a shared decision-making encounter should encompass. This encounter is a meeting between the physician, who can present the risks and benefits of different options, and the patient, who can express their interests and values. There are 4 necessary characteristics in a shared decision-making encounter:
1. Both the physician and patient are present and involved in the decision.
2. Both the physician and patient share information with each other.
3. Both the physician and patient take steps to express treatment preferences.
4. A treatment decision is made, and both the physician and patient agree on the treatment to implement.4
It is vital that the patient is not pressured to accept device implantation and has the opportunity to express their values and wishes.5
Current guidelines allow for patient preference on long-term anticoagulation vs a short course of anticoagulation to pursue LAAO.6 If after documenting preferences and risks, the patient’s decision is to pursue LAAO, they are sent for transesophageal echocardiography (TEE).7
Preimaging
Both structural and electrophysiology (EP) implanting physicians are used at our institution. A TEE or cardiac tomography (CT) is performed prior to implant to assess LAA thrombus, stasis of blood, and morphology and size of the LAA. Anticoagulation is generally held for 2 days prior to the procedure to prevent bleeding, unless there is dense stasis, in which case anticoagulation may be continued up until the day prior to procedure.
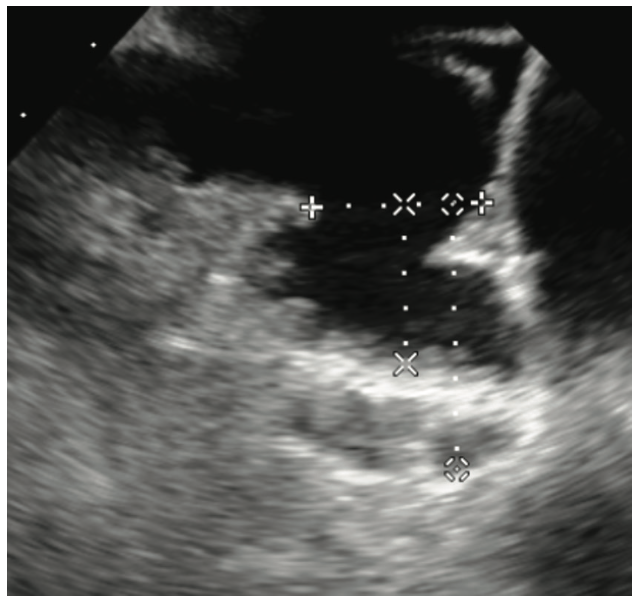
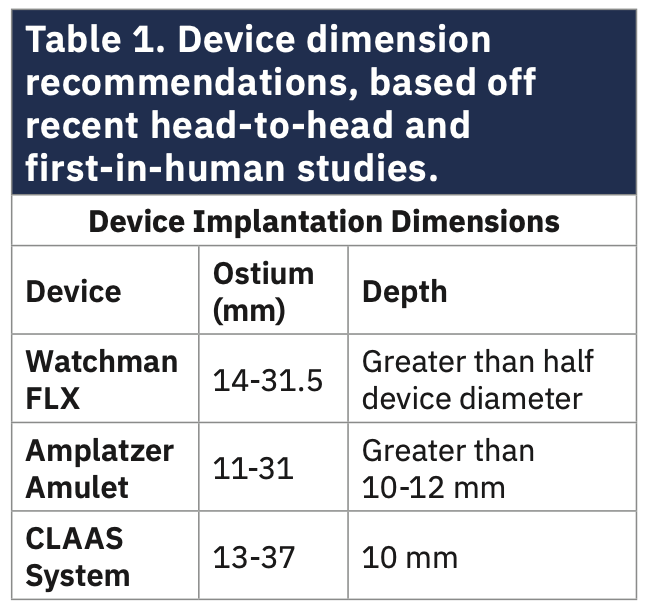
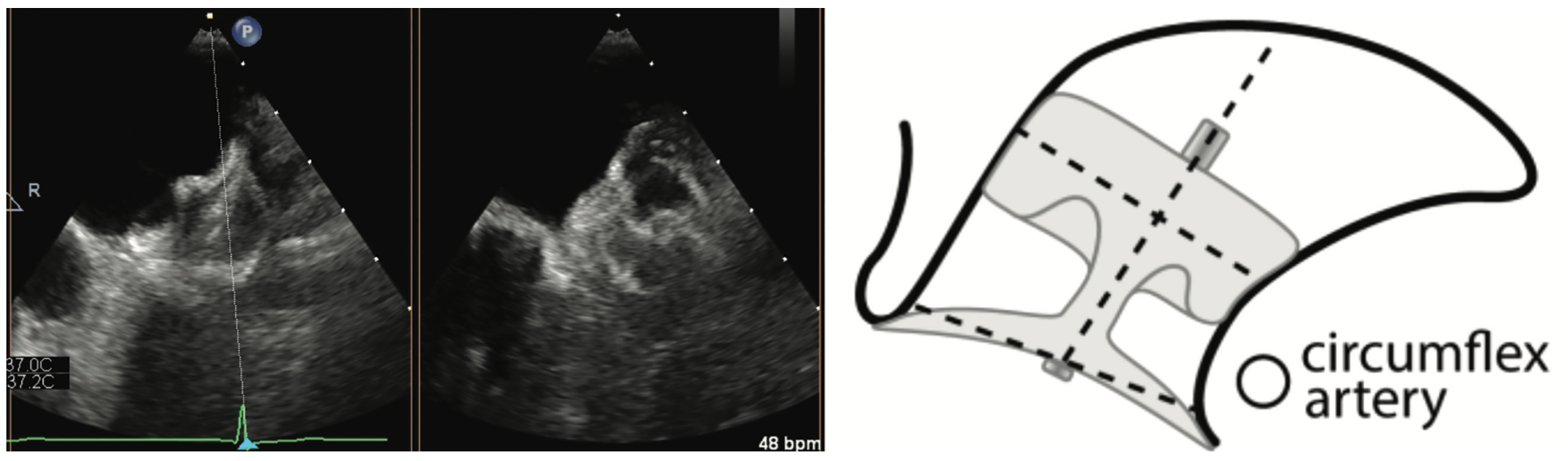
Aside from routine TEE imaging, the preimplantation examination focuses on the LAA dimensions using standardized views derived from the CHAMPION-AF trial.8 In addition to standard views at 0, 45, 90, and 135, each of these views is bisected with a cutting plane. It is also important to document the working depth of the LAA rather than the absolute depth (Figure 1). Measuring both the os and depth of the LAA helps to determine which devices can be offered to the patient. Our institution offers the Amulet, CLAAS System (Conformal Medical), and Watchman FLX device (Table 1). The implanting physician then reviews the images and determines the most appropriate device option.
Procedure
On the day of implantation, the patient is brought to the short-stay unit, where they will reside until discharge later that day or the following day, depending on if there are procedural complications.9 These procedures are required by CMS to be performed at sites with a structural heart or EP program. Implanting physicians must be trained on each device and have continued to implant at least 12 devices over a 2-year period.1
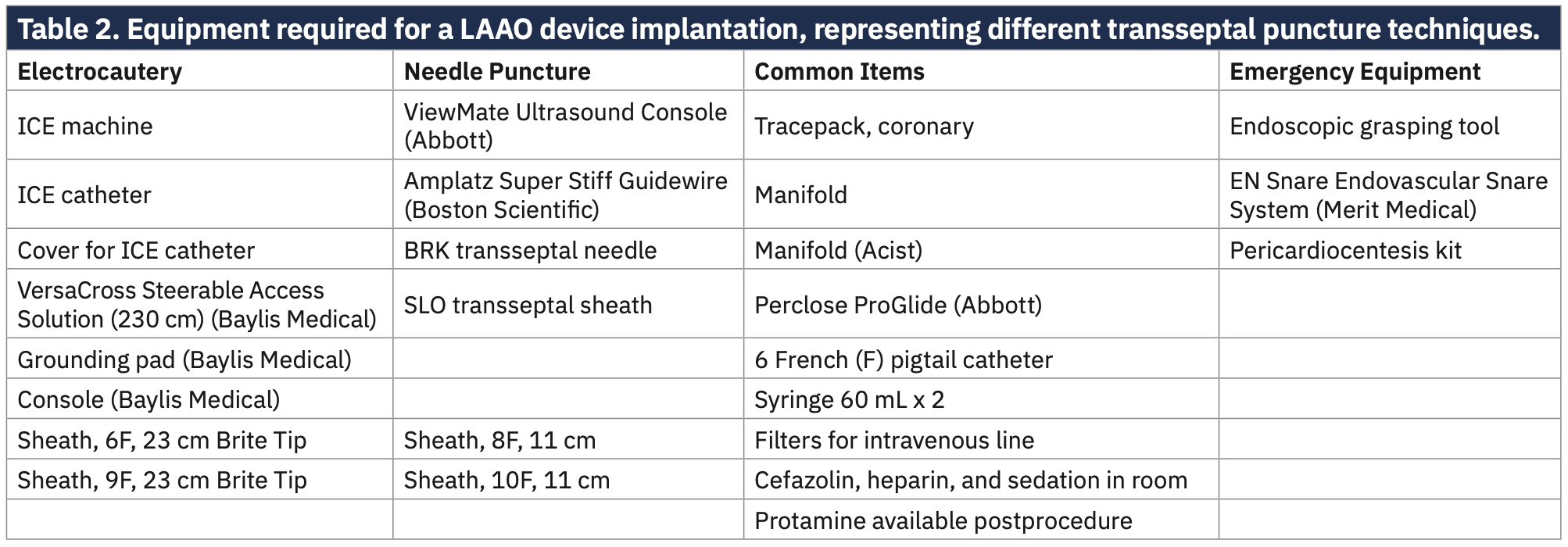
In prepping the laboratory, consideration must be made for imaging modalities, sedation, and the device. If conscious sedation is used, intracardiac echocardiography (ICE) is useful for visualizing the transseptal puncture. If general anesthesia is used, a TEE probe offers visualization of the septum. If a physician is still training on a device, both can be useful in a general anesthesia case to better visualize the septum and LA. At our institution, the septum is crossed with a needle puncture or electrocautery. The tools required for the case are dependent on the device, sedation, and mechanism of transseptal puncture. Table 2 includes equipment lists for staff for the 2 most common methods of transseptal puncture.
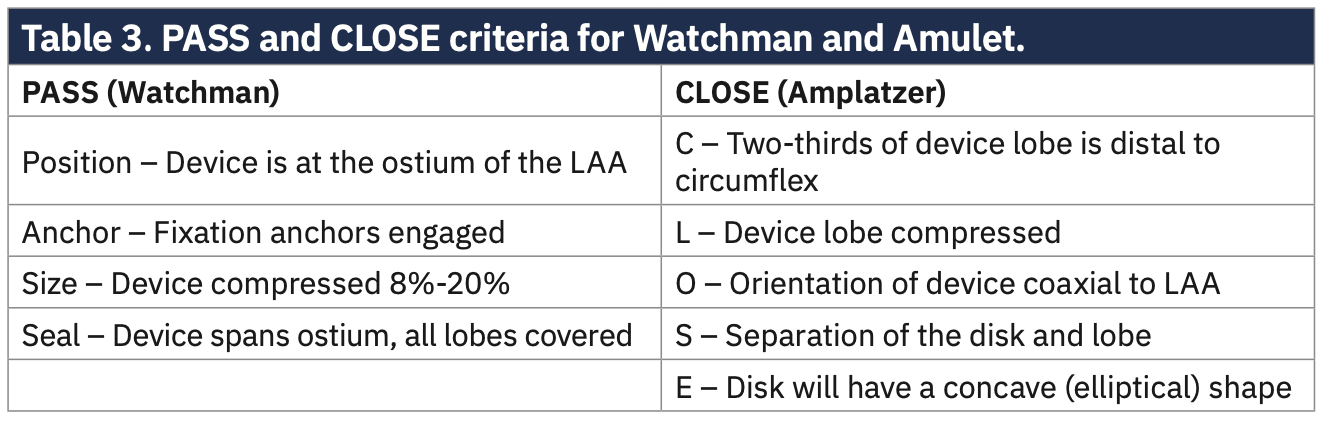
Once the procedure has started, imaging confirms the status of any pericardial fluid, and an image is saved as a reference. Fluids are administered, usually about 500 mL of crystalloid to increase the LA pressure. The transseptal puncture is visualized under the imaging modality for that case. Direct pressure measurement of the LA can be made at this point, and fluid can be administered if the left atrial pressure (LAP) is not sufficient (our preference is to give fluid for LAP <10 mm Hg). After measurements of the LAA have been confirmed during the procedure and there is no clot in the appendage, the device is implanted. A Brockenbrough needle with SLO is used for transseptal access and exchanged using an Amplatz Super Stiff Guidewire (Boston Scientific). The Watchman delivery sheath comes in anterior and double curve, and the double curve sheath is most commonly used. A right anterior oblique (RAO) caudal projection is used to deliver the Watchman, and a RAO cranial image is used for the Amulet. LAA measurements are taken again to ensure appropriate sizing of the Watchman. The sizing is determined by maximum LAA diameter and depth in all angles. After review with the anesthesiologist or cardiologist, a Watchman device is chosen and flushed with care on the back table to ensure there is no air in the device. The device is then placed in the Watchman access sheath and locked into place. Under breath hold with anesthesia, the device is deployed. However, prior to release, PASS (Position, Anchor, Size, and Seal) criteria should be reviewed. Position determines that the device is at the ostium of the LAA. Anchor is determined by evaluating if the fixation anchors are engaged and the device is stable by using a tug test on the deployment knob. Size ensures the device is compressed at 8%-20% of the original size. Seal ensures the device covers all the ostium and all the lobes are covered. If all 4 of these device criteria are met, the Watchman can be released.
The Amulet device has 3 delivery sheaths, and the TorqVue is most commonly used. An oversizing of 2-4 mm is performed for the Amulet. TEE measurements at both short axis and long axis of the landing zone and the orifice are used for LAA measurement. Intraprocedural imaging is most commonly used with TEE. ICE is also used for lower risk cases, but in more experienced hands. Safety checks involve PASS criteria for Watchman and CLOSE criteria for Amulet (Table 3).
After a tug test, which lasts between 30-45 seconds, the device can be untethered. If there is any issue with device deployment or stability during the procedure, the device can be retrieved with either a snare or endoscopic grasping tool (Raptor, Steris). One of the most common complications from LAAO is pericardial tamponade. Therefore, after the procedure is completed, the pericardium is reevaluated to confirm the absence of pericardial effusion. Upon successful completion, the catheters are removed and the venotomies are closed with a closure device or figure-of-8 stitch. Patients are typically discharged the same day.
Postoperative Implant
The postimplantation anticoagulation regimen used in the landmark trials for the Watchman device was aspirin (ASA) and warfarin with an international normalized ratio of 2-3 initiated the day of the procedure. A TEE was performed 45 days later to assess for any leaks >5 mm around the device or device-related thrombosis (DRT).10,11 If no significant leak of >5 mm or DRT were present, warfarin was dropped in favor of clopidogrel and ASA for 6 months, and then ASA indefinitely.11 Other studies were conducted to ensure safety of postimplantation anticoagulation regimens with dual antiplatelet therapy (DAPT)12 or DOAC and ASA.13,14 Retrospective studies have shown both DAPT and DOAC strategies to be noninferior to warfarin. Both the Amulet and WATCHMAN FLX now have FDA approval for DAPT alone after LAAO.
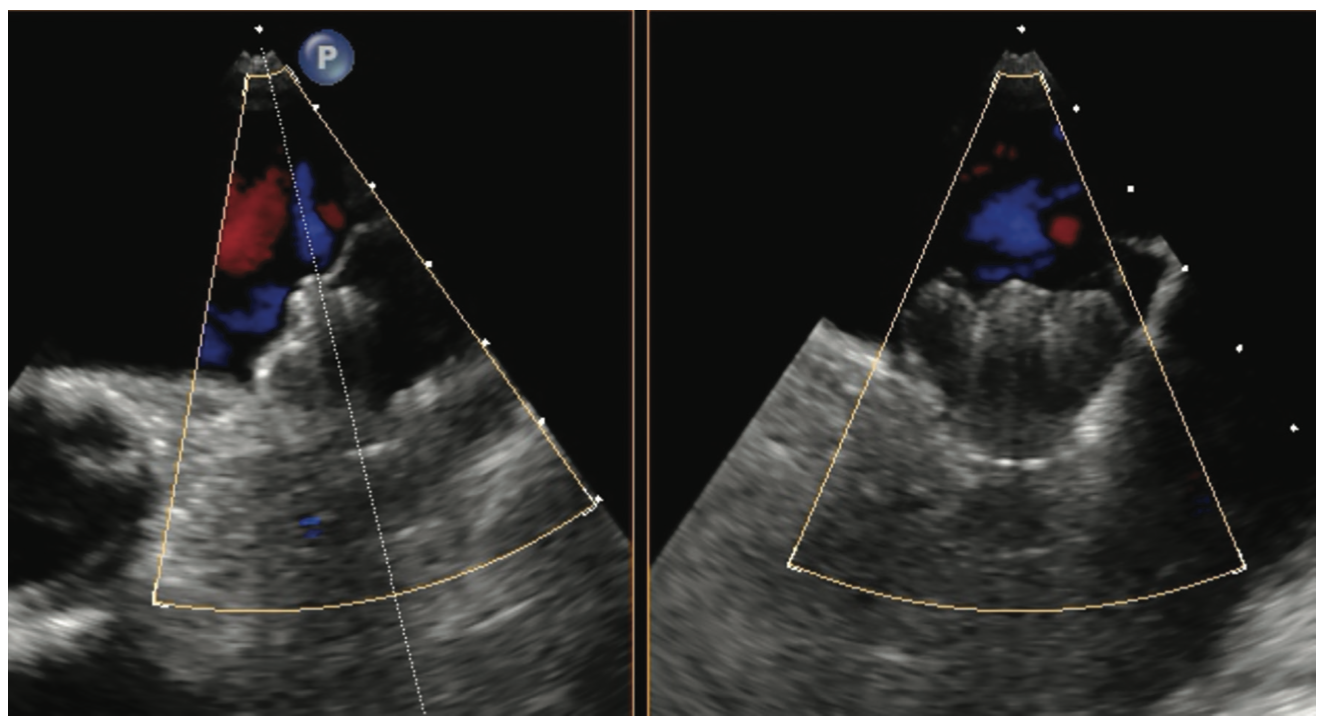
Using TEE 45 days after implantation, we use the same practices, specific angles for evaluation, and x-plane as in the preimplantation TEE (Figures 2 and 3). We also use a reduced viewing angle to only look at one-half of the device at a time, thus increasing the frame rate. Nyquist limits are reduced to be more sensitive to the lower pressures generated in the LA. The study is read immediately and relayed to the implanting physician. Patients are usually seen in the clinic that afternoon and their anticoagulation regimen is adjusted as needed. Video 1 demonstrates a well-seated Watchman FLX device, and Video 2 shows a well-seated Amulet device.
There are also epicardial solutions for LAAO. The Lariat procedure (SentreHeart, Inc) bridges the endocardial and epicardial approach; however, it has a more complex risk profile.15 During the workup for LAAO, if additional pathology such as severe valve disease, reduced ejection fraction, or ischemic symptoms are discovered, cardiothoracic surgery is involved. Guidelines recommend a heart team approach for any patients with a valvular disorder.16,17 During an open procedure, the AtriClip (AtriCure, Inc) can be used. Patients with persistent or long-standing persistent AF may benefit from a convergent procedure.18 The first phase of this procedure involves a pericardial window from the transdiaphragmatic or subxiphoid approach for epicardial ablation, during which an AtriClip can be deployed (Video 3).
There are also new devices on the horizon that aim to improve the success of the procedure, including the CLAAS System. It comes in 2 sizes, 27 mm and 35 mm, with a landing zone of 10 mm. The sheath has a single or double curve. Both the CHAMPION-AF and CATALYST trials are comparing LAAO to DOACs with the hypothesis of equal efficacy but greater safety. The OPTION trial is investigating oral anticoagulation vs LAAO after ablation of AF. These trials will only increase the utilization of LAAO as a primary treatment modality if they show benefit. Given the increase of the procedure, we see a shifting role toward less general anesthesia.
Summary
EPs have a litany of options for the treatment of stroke prophylaxis in patients with AF. As more devices come to market with different properties, we will be able to incorporate patient preference. Just as surgical aortic valve replacement and transcatheter aortic valve replacement are best managed with a heart team approach to determine the most appropriate therapy, we will see the management of AF move to this model.19 The number of implanting physicians will continue to increase as both structural cardiologists and EPs are trained to place a LAAO device. These procedure times will likely continue to decrease and may eventually be routinely incorporated as part of an ablation.20 Pharmacologic management of stroke prophylaxis will likely occupy a smaller portion of the AF population, and warfarin will continue to decline outside of situations where clinicians are obligated to use a vitamin K antagonist.
AF is a complex atrial conduction disease marked by its striking risk for cardioembolic strokes. While the treatment of the underlying pathology continues to evolve, we need to protect patients from the devastating effects of stroke. How we prevent this sequela has evolved from a minimally effective anticoagulant to multiple medications and mechanical devices. EPs will continue to evolve with the changing modalities and engage with patients regarding their preferences.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. They report no conflicts of interest regarding the content herein. Outside the work, Dr Manyam reports consulting fees from Abbott, Boston Scientific, Janssen, and Philips; support for attending meetings and/or travel from Philips; and participation on a data safety monitoring board or advisory board from ZOLL Medical.
References
1. Jensen TS, Chin J, Ashby L, Long K, Schafer J, Hakim R. Percutaneous left atrial appendage closure (LAA) closure therapy. CMS.gov. Published February 8, 2016. Accessed January 25, 2023. https://www.cms.gov/medicare-coverage-database/view/ncacal-decision-memo.aspx?proposed=N&NCAId=281
2. Atrial fibrillation. CardioSmart. Published August 25, 2021. Accessed January 25, 2023. https://www.cardiosmart.org/topics/atrial-fibrillation
3. Coylewright M, O’Neill E, Sherman A, et al. The learning curve for shared decision-making in symptomatic aortic stenosis. JAMA Cardiol. 2020;5(4):442-448. doi:10.1001/jamacardio.2019.5719
4. Charles C, Gafni A, Whelan T. Decision-making in the physician-patient encounter: revisiting the shared treatment decision-making model. Soc Sci Med. 1999;49(5):651-661. doi:10.1016/s0277-9536(99)00145-8
5. Seaburg L, Hess EP, Coylewright M, Ting HH, McLeod CJ, Montori VM. Shared decision making in atrial fibrillation: where we are and where we should be going. Circulation. 2014;129(6):704-710. doi:10.1161/CIRCULATIONAHA.113.004498
6. January CT, Wann LS, Calkins H, et al. 2019 AHA/ACC/HRS Focused Update of the 2014 AHA/ACC/HRS guideline for the management of patients with atrial fibrillation: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines and the Heart Rhythm Society in collaboration with the Society of Thoracic Surgeons. Circulation. 2019;140(2):e125-e151. doi:10.1161/CIR.0000000000000665
7. Moussa Pacha H, Al-Khadra Y, Soud M, Darmoch F, Moussa Pacha A, Alraies MC. Percutaneous devices for left atrial appendage occlusion: a contemporary review. World J Cardiol. 2019;11(2):57-70. doi:10.4330/wjc.v11.i2.57
8. CHAMPION-AF clinical trial. Clinicaltrials.gov. Accessed January 25, 2023. https://clinicaltrials.gov/ct2/show/NCT04394546
9. Kleinecke C, Allakkis W, Buffle E, et al. Impact of conscious sedation and general anesthesia on periprocedural outcomes in Watchman left atrial appendage closure. Cardiol J. 2021;28(4):519-527. doi:10.5603/CJ.a2020.0184
10. Holmes DR, Reddy VY, Turi ZG, et al. Percutaneous closure of the left atrial appendage versus warfarin therapy for prevention of stroke in patients with atrial fibrillation: a randomised non-inferiority trial. Lancet. 2009;374(9689):534-542. doi:10.1016/S0140-6736(09)61343-X
11. Holmes DR Jr, Kar S, Price MJ, et al. Prospective randomized evaluation of the Watchman left atrial appendage closure device in patients with atrial fibrillation versus long-term warfarin therapy: the PREVAIL trial. J Am Coll Cardiol. 2014;64(1):1-12. doi:10.1016/j.jacc.2014.04.029
12. Reddy VY, Möbius-Winkler S, Miller MA, et al. Left atrial appendage closure with the Watchman device in patients with a contraindication for oral anticoagulation: the ASAP study (ASA Plavix feasibility study with Watchman left atrial appendage closure technology). J Am Coll Cardiol. 2013;61(25):2551-2556. doi:10.1016/j.jacc.2013.03.035
13. Cohen JA, Heist EK, Galvin J, et al. A comparison of postprocedural anticoagulation in high-risk patients undergoing WATCHMAN device implantation. Pacing Clin Electrophysiol. 2019;42(10):1304-1309. doi:10.1111/pace.13796
14. Holmes DR Jr, Reddy VY, Gordon NT, et al. Long-term safety and efficacy in continued access left atrial appendage closure registries. J Am Coll Cardiol. 2019;74(23):2878-2889. doi:10.1016/j.jacc.2019.09.064
15. O’Neill WW. The Lariat device: R.I.P. or buried alive. J Am Coll Cardiol. 2018;72(12):1354-1356. doi:10.1016/j.jacc.2018.07.019
16. Khanji MY, Ricci F, Galusko V, et al. Management of aortic stenosis: a systematic review of clinical practice guidelines and recommendations. Eur Heart J Qual Care Clin Outcomes. 2021;7(4):340-353. doi:10.1093/ehjqcco/qcab016
17. Otto CM, Nishimura RA, Bonow RO, et al. 2020 ACC/AHA guideline for the management of patients with valvular heart disease: executive summary: a report of the American College of Cardiology/American Heart Association Joint Committee on Clinical Practice Guidelines. Circulation. 2021;143(5):e35-e71. doi:10.1161/CIR.0000000000000932
18. DeLurgio DB, Crossen KJ, Gill J, et al. Hybrid convergent procedure for the treatment of persistent and long-standing persistent atrial fibrillation: results of CONVERGE clinical trial. Circ Arrhythm Electrophysiol. 2020;13(12):e009288. doi:10.1161/CIRCEP.120.009288
19. Nishimura RA, Otto CM, Bonow RO, et al. 2017 AHA/ACC Focused Update of the 2014 AHA/ACC guideline for the management of patients with valvular heart disease: a report of the American College of Cardiology/American Heart Association Task Force on Clinical Practice Guidelines. J Am Coll Cardiol. 2017;70(2):252-289. doi:10.1016/j.jacc.2017.03.011
20. Domain G, Dognin N, O’Hara G, et al. Experience of combined procedure during percutaneous LAA closure. J Clin Med. 2022;11(12). doi:10.3390/jcm11123280
Related Content





