

Pacing Type Versus Ventricular Synchrony: Which is More Important?
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2023;23(12):1,10-12.
Karol Curila, MD, MSc, PhD,1 and Pavel Jurak, MSc, PhD2
1Cardiocenter, Third Faculty of Medicine, Charles University and University Hospital Kralovske Vinohrady, Prague, Czech Republic; 2Institute of Scientific Instruments, the Czech Academy of Sciences, Brno, Czech Republic
The main impetus for developing conduction system pacing (CSP) methods was to minimize dyssynchronous ventricular activation associated with right ventricular (RV) myocardial pacing in patients with bradycardia or heart failure and bundle branch block.1,2 His bundle pacing (HBP), left ventricular septal pacing (LVSP), and left bundle branch pacing (LBBP) result in synchronous biventricular or at least left ventricular (LV) activation and, in the recent past, have shaped the clinical approach.
Theoretically, CSP is the optimal treatment method to minimize ventricular dyssynchrony in patients with bradycardia with anticipated high ventricular pacing burden. However, CSP methods are more complex, time-consuming, and costly than RV myocardial pacing, which is well-tolerated in many patients. Therefore, it would be most reasonable to offer CSP to patients at highest risk of pacing-induced heart failure.
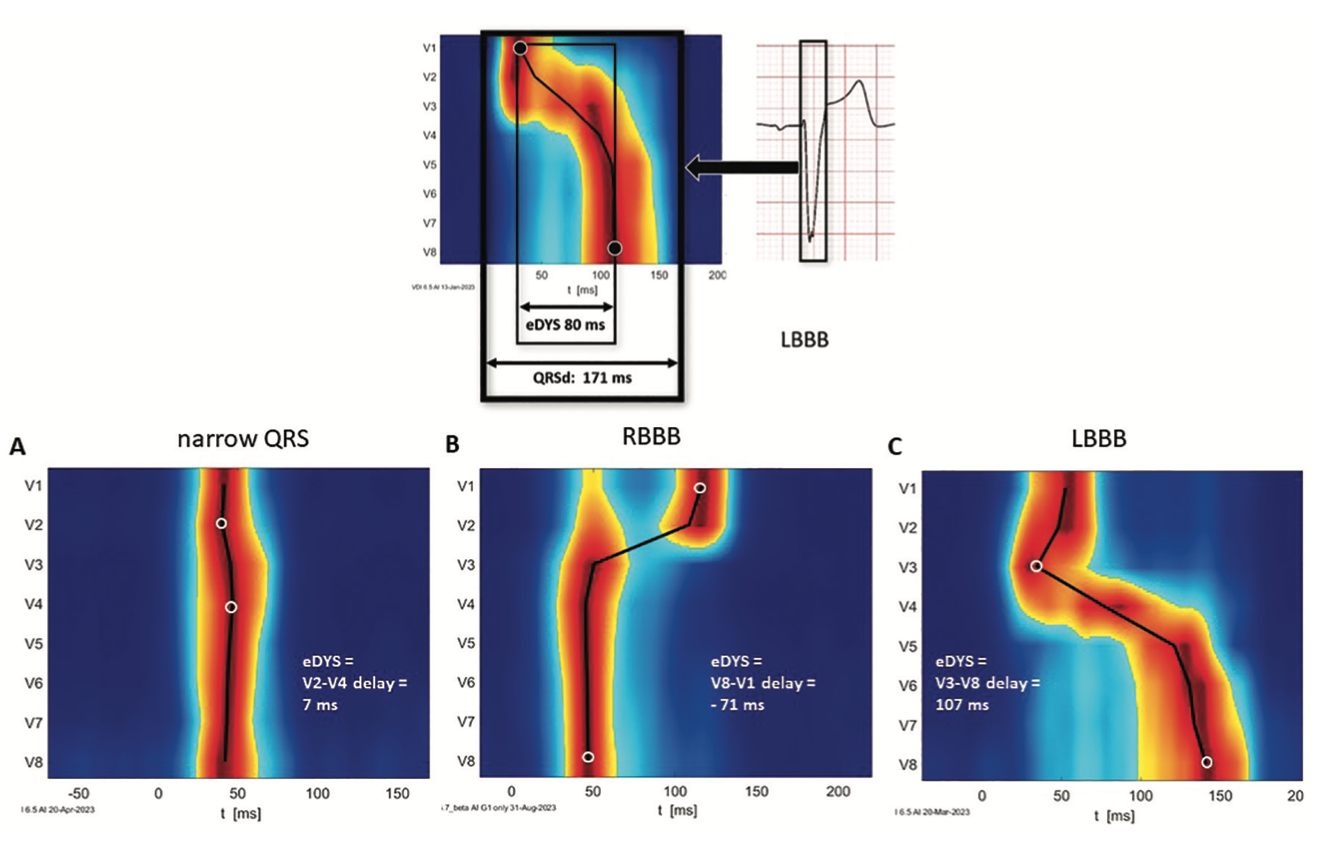
The question is how to identify them when risk factors, such as QRSd, gender, and coronary artery disease, have been shown to have low predictive value3 and when visualization of ventricular dyssynchrony was not routinely feasible during implant procedures. A new technology based on ultra-high-frequency electrocardiography (UHF-ECG) has recently received intensive study.4 It allows real-time ventricular dyssynchrony assessment by processing 100-1000 Hz ECG signals. In almost all patients, detailed information about timing differences between activations of ventricular segments below standard precordial leads is available in less than 5 minutes (Figure 1).
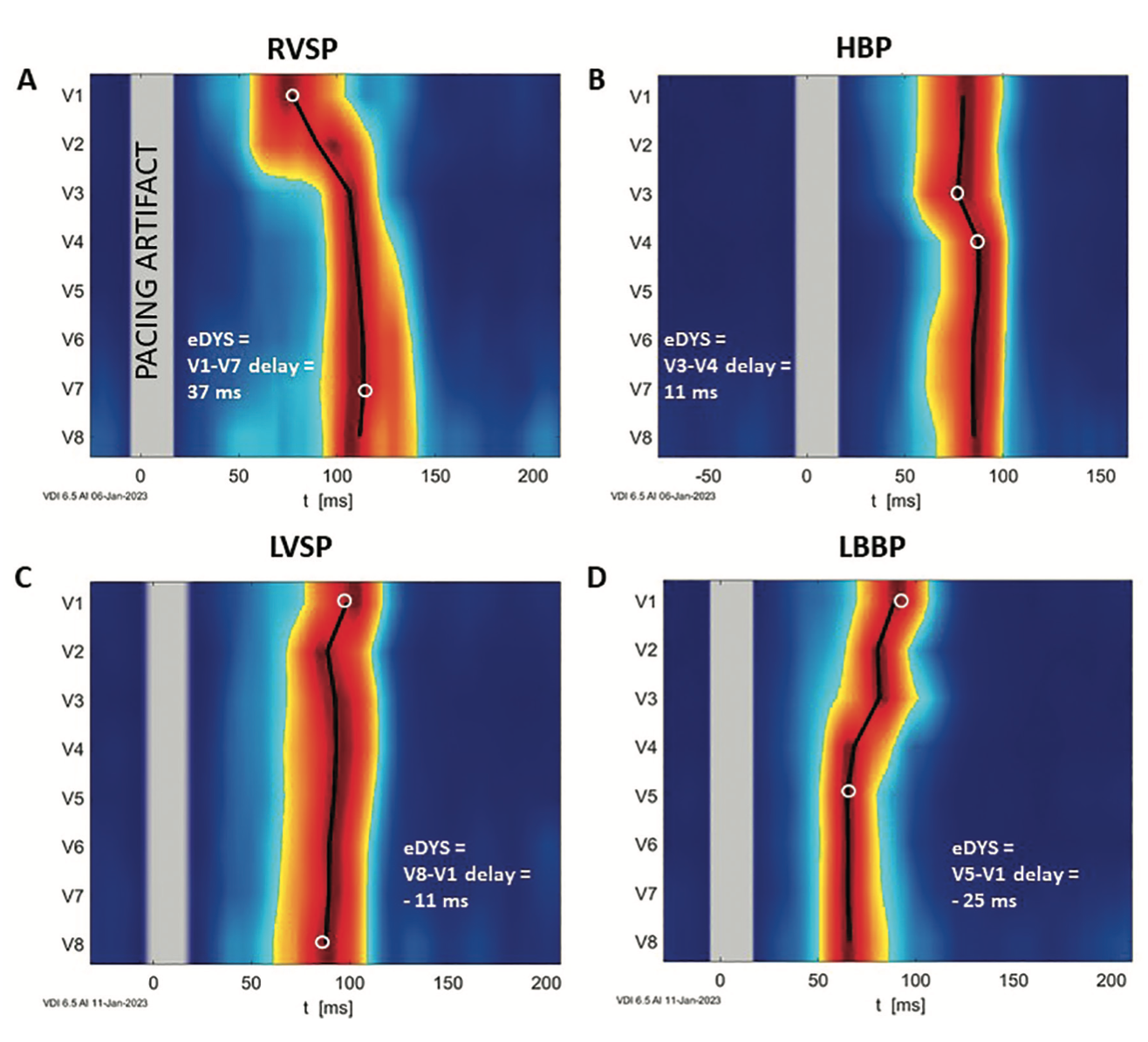
UHF-ECG studies in patients with bradycardia have shown that all CSP methods provide more physiological ventricular activation than any RV pacing method with myocardial capture.5-9 Ventricular dyssynchrony during HBP, LBBP, and LVSP is much smaller than RV septal pacing (RVSP), which is believed to be the best RV myocardial pacing location (Figure 2).
HBP provides the best ventricular synchrony of all CSP methods,6,9 but its utilization is declining because of several shortcomings.10 LBBP and LVSP are less physiological than HBP6 but are increasingly gaining popularity due to lead stability, sensing values, and pacing thresholds, which are typically better than during HBP. We hypothesize that LBBP and LVSP will provide similar clinical outcomes in bradycardia patients, and studying ventricular dyssynchrony during RV myocardial pacing, LBBP, and LVSP might provide some important insights.
In one study, the average ventricular dyssynchrony during RVSP was 37 milliseconds (a representative example of RVSP with an electrical dyssynchrony (eDYS) of 37 milliseconds is shown in Figure 2, Panel A). All CSP (HBP, LBBP, and LVSP) led to less dyssynchronous ventricular activation than RVSP, with an eDYS of 10 milliseconds during HBP, -12 milliseconds during LVSP, and -24 milliseconds during LBBP. Moreover, the delays in LV lateral wall activations (V5-V8), which may be more associated with LV hemodynamics and clinical outcomes than eDYS, are much shorter during HBP, LVSP, and LBBP compared to RVSP (Figure 2).
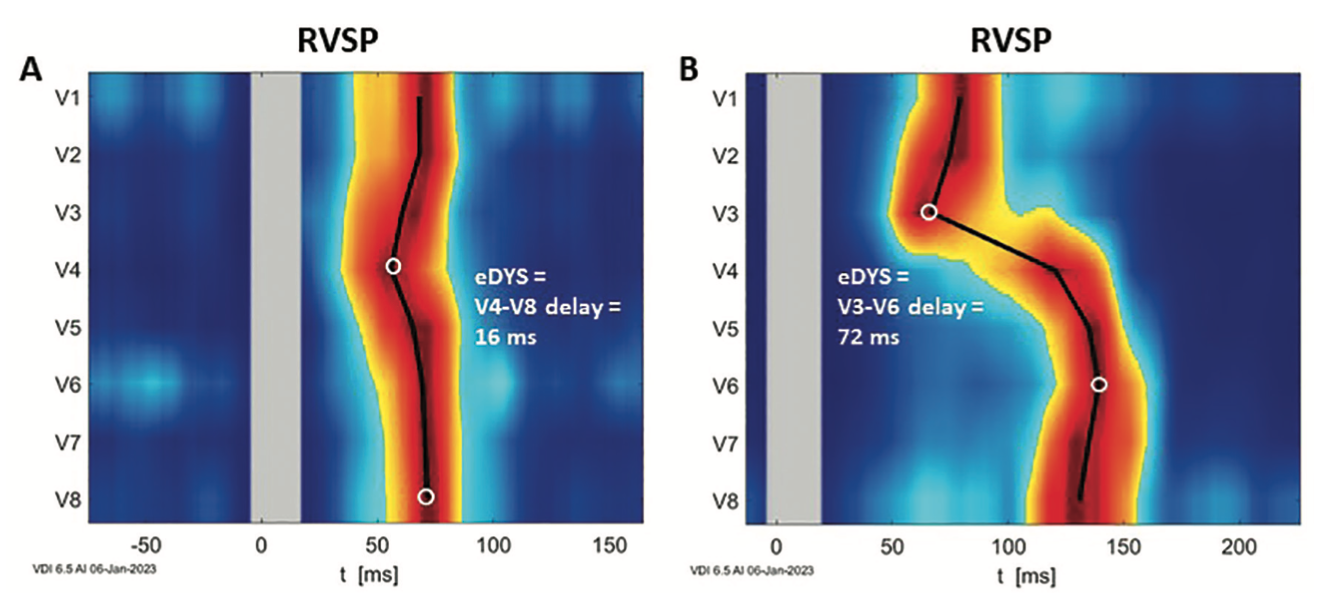
Interestingly, a substantial interindividual heterogeneity among patients receiving RVSP was observed. Many had eDYS values below 30 milliseconds (Figure 3A), while others had significant ventricular dyssynchrony during RVSP (Figure 3B).
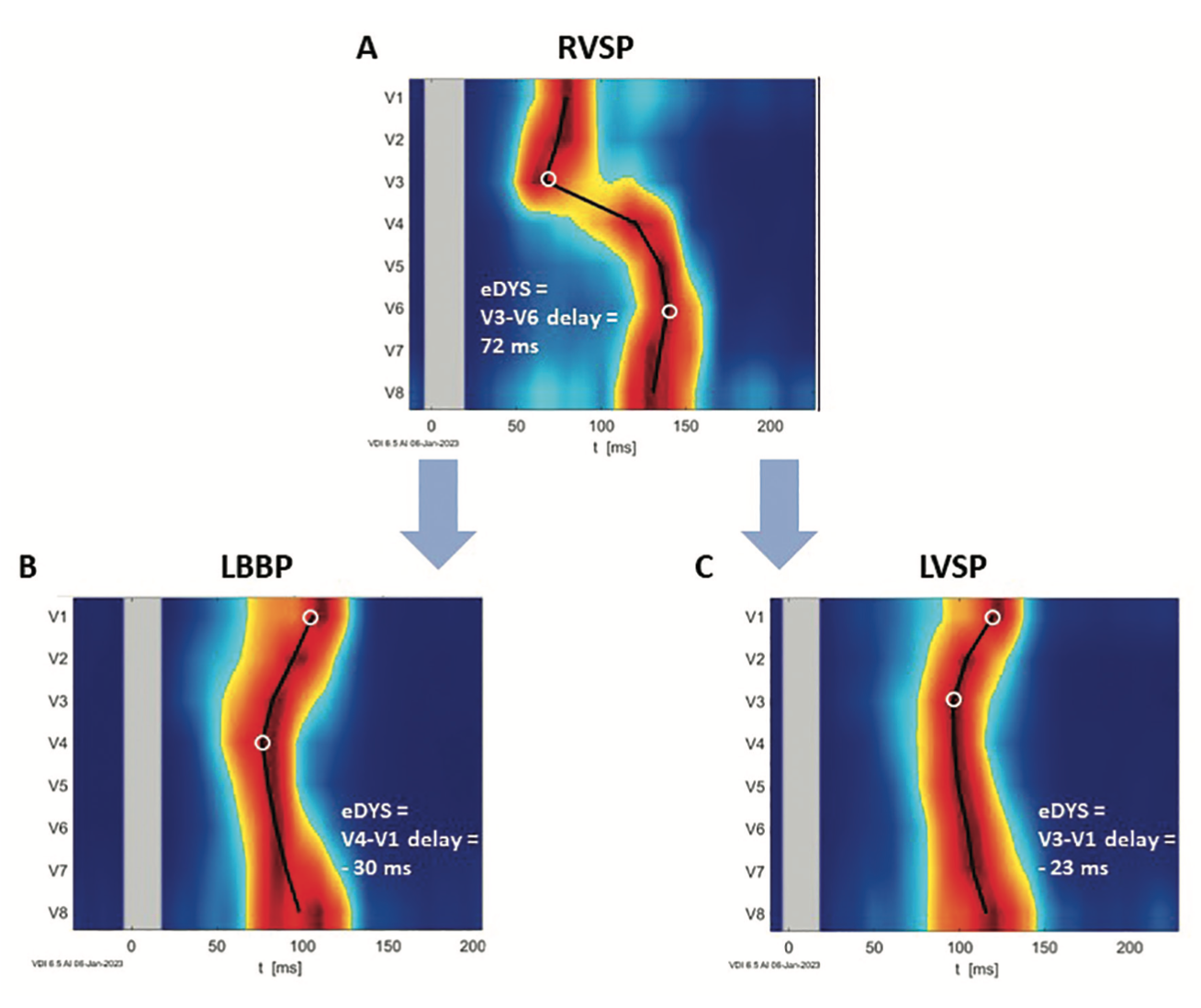
If dyssynchrony is a leading cause of the harmful effects of RV myocardial pacing, then patients with significant ventricular dyssynchrony during RV pacing are at risk of pacing-induced cardiomyopathy. Therefore, only those patients stand to benefit the most from more physiological ventricular pacing. The type of left septal pacing performed (LBBP or LVSP) should not matter since both types provide, on average and individually, more synchronous ventricular activation than RVSP. An example of LBBP and LVSP in a patient with significant dyssynchrony during RVSP is shown in Figure 4.
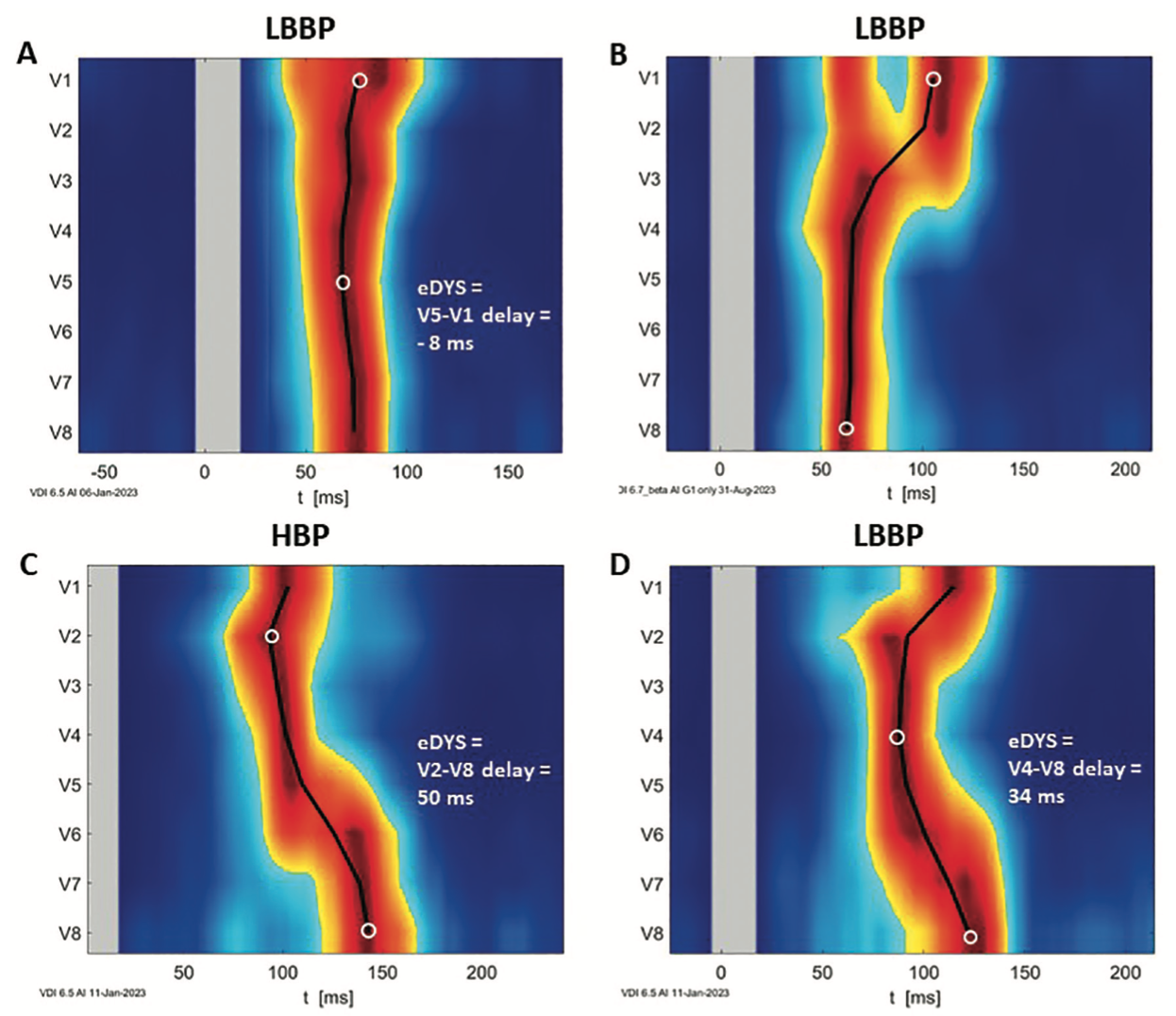
As with RVSP, where ventricular UHF-ECG dyssynchrony varies significantly between patients, LBBP and LVSP can also be associated with diverse activation patterns. In some patients, we see a right-to-left activation pattern, even during LVSP. The eDYS is positive in these patients, but the delays in the activations of the segments under V6-V8 from the first activation are rarely higher than 20 milliseconds. Other patients can have ventricular dyssynchrony close to zero milliseconds, even during LBBP. These patients usually have small hearts, very narrow intrinsic QRS complexes, and a proximal LBB pacing location (Figure 5A). In patients with BBB, LBBP may lead to significant left-to-right ventricular dyssynchrony (Figure 5B). We have also observed that in patients with LV distal conduction defects due to scars, even direct capture of the HB or LB may not lead to synchronous LV activation. An example of HBP and LBBP in a patient with a scar in the LV inferior wall is shown in Figure 5C and 5D.
In the last 20 years, many studies have demonstrated the harmful effects of ventricular dyssynchrony on the clinical outcome of patients with or without heart failure. Despite a significant need, we did not have clinically applicable tools for displaying ventricular dyssynchrony in clinical practice. Our experience shows that UHF-ECG can assess ventricular dyssynchrony in practically all patients, both in the operating room or office. UHF-ECG depicts ventricular activation and ventricular dyssynchrony in a way that is easy to understand and provides patient-specific information during intrinsic rhythms or pacing. By studying this data, CSP methods (ie, HBP, LBBP, and LVSP) result in more synchronous ventricular activation than pacing from any location in the RV. Ventricular dyssynchrony also varies significantly between patients, even when using the same type of pacing. Superior ventricular synchrony, rather than the type of pacing, should be a goal of implant procedures. Only in this way can the adverse effects of ventricular dyssynchrony on the clinical outcome of patients be minimized.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Karol Curila and Pavel Jurak filed a US patent No: US 11,517,243 B2, “Method of electrocardiographic signal processing and apparatus for performing the method,” and are shareholders of VDI Technologies. Dr Curila reports consulting fees from Medtronic, payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Medtronic, Biotronik, and Boston Scientific, and stock or stock options from VDI Technologies. Dr Jurak reports a grant or contract for a VDI mapping technological project financed by the Agency of the Czech Republic, and participation on the VDI Technologies advisory board.
References
1. Khurshid S, Epstein AE, Verdino RJ, et al. Incidence and predictors of right ventricular pacing-induced cardiomyopathy. Heart Rhythm. 2014;11(9):1619-1625. doi:10.1016/j.hrthm.2014.05.040
2. Vernooy K, Verbeek XA, Peschar M, Prinzen FW. Relation between abnormal ventricular impulse conduction and heart failure. J Interv Cardiol. 2003;16(6):557-562. doi:10.1046/j.1540-8183.2003.01061.x
3. Kiehl EL, Makki T, Kumar R, et al. Incidence and predictors of right ventricular pacing-induced cardiomyopathy in patients with complete atrioventricular block and preserved left ventricular systolic function. Heart Rhythm. 2016;13(12):2272-2278. doi:10.1016/j.hrthm.2016.09.027
4. Jurak P, Curila K, Leinveber P, et al. Novel ultra-high-frequency electrocardiogram tool for the description of the ventricular depolarization pattern before and during cardiac resynchronization. J Cardiovasc Electrophysiol. 2020;31(1):300-307. doi:10.1111/jce.14299
5. Curila K, Jurak P, Halamek J, et al. Ventricular activation pattern assessment during right ventricular pacing: Ultrahigh-frequency ECG study. J Cardiovasc Electrophysiol. 2021;32(5):1385-1394. doi:10.1111/jce.14985
6. Curila K, Jurak P, Jastrzebski M, et al. Left bundle branch pacing compared to left ventricular septal myocardial pacing increases interventricular dyssynchrony but accelerates left ventricular lateral wall depolarization. Heart Rhythm. 2021;18(8):1281-1289. doi:10.1016/j.hrthm.2021.04.025
7. Curila K, Jurak P, Prinzen F, et al. Bipolar anodal septal pacing with direct LBB capture preserves physiological ventricular activation better than unipolar left bundle branch pacing. Front Cardiovasc Med. 2023;10:1140988. doi:10.3389/fcvm.2023.1140988
8. Curila K, Jurak P, Vernooy K, et al. Left ventricular myocardial septal pacing in close proximity to LBB does not prolong the duration of the left ventricular lateral wall depolarization compared to LBB pacing. Front Cardiovasc Med. 2021;8:787414. doi:10.3389/fcvm.2021.787414
9. Curila K, Prochazkova R, Jurak P, et al. Both selective and nonselective His bundle, but not myocardial, pacing preserve ventricular electrical synchrony assessed by ultra-high-frequency ECG. Heart Rhythm. 2020;17(4):607-614. doi:10.1016/j.hrthm.2019.11.016
10. Teigeler T, Kolominsky J, Vo C, et al. Intermediate-term performance and safety of His-bundle pacing leads: a single-center experience. Heart Rhythm. 2021;18(5):743-749. doi:10.1016/j.hrthm.2020.12.031

