

Pulsed Field Ablation for Atrial Fibrillation: Recent Advances and Future Directions
EP Lab Digest. 2023;23(3):19-21.
Catheter ablation is a well-accepted rhythm control strategy for patients with symptomatic atrial fibrillation (AF).1 Ectopic beats initiating in the pulmonary veins (PV) are the primary trigger for AF.2 Thus, catheter ablation for AF has included pulmonary vein isolation (PVI) as the mainstay of this procedure. Since its inception, catheter ablation has been performed with a thermal energy source (primarily radiofrequency [RF] energy or cryotherapy). The most recent and exciting development in this arena has been the advent of pulsed field ablation (PFA) as a nonthermal alternate energy source. As such, it has the potential to selectively target cardiac tissue without injuring surrounding tissues such as the phrenic nerve, esophagus, and other vascular structures.
Background
As a function of the transmembrane potential, an electrical pulse can either have no effect on a cell, reversibly open cell membranes and allow the cell to survive, or irreversibly make the cells permeable causing cell death.3 Various mechanisms of cell injury and death have been reported with electroporation, including increases in intracellular calcium, mitochondrial disruption, DNA damage, and reactive oxygen species production that can lead to apoptosis and necrosis.4 Electroporation has traditionally been used as a way to increase cell permeability reversibly to introduce small molecules, chemotherapeutic agents, and DNA.5 However, irreversible electroporation as a method to ablate undesirable tissue was introduced with mathematical modeling in 2005.6
Despite high voltage (~1000V), there is a limited thermal effect due to the short duration of delivery (less than 100 µs).7 This feature helps limit damage to surrounding tissues. This process is tissue specific, but the mechanism of tissue specificity is not completely understood.8 To optimize irreversible electroporation, it is important to account for the waveform, R-wave synchronization, electrical field intensity, pulse frequency, and the number of pulses applied.9 However, there is a limit, because increasing the electrical field size or number of pulses can lead to an increase in heat and potential thermal injury.10
Preclinical Studies
Lavee et al first described the use of electroporation for the ablation of cardiac tissue in 2007.11 With a porcine model, a clamp delivered electroporation to epicardial atrial tissue, demonstrating that transmural lesions could be created in as short as 1-4 seconds without thermal effects or damage to surrounding tissue. It also appeared that cardiac myoblasts may have some of the lowest thresholds for cell damage, which may make them uniquely suited for targeted damage using PFA.12 Subsequent preclinical work looked at feasibility of irreversible electroporation for the creation of PV ostial lesions and the treatment of other cardiac arrhythmias.13-15 Nerve tissue is more resistant to injury by electroporation, with full recovery seen even after PFA was delivered directly to rat sciatic nerves or porcine phrenic nerves.16,17
Even more reassuring for dreaded complications was additional data that showed no evidence of esophageal disruption, durable coronary injury, or PV stenosis with electroporation.18 Applying electroporation directly to a porcine esophagus showed no damage to the adventitia or evidence of thermal damage, although there was scarring noted in the esophageal musculature.19 A swine model with direct delivery of PFA at the base of the heart and on the left anterior descending (LAD) artery showed minimal intimal hyperplasia and no hemodynamically significant stenosis after 3 weeks.20 The earlier safety data appeared to be overwhelmingly positive for coronary artery injury, but more recent preclinical work with the Farapoint precision focal catheter (Farapulse, Boston Scientific) directly applied to epicardial coronary arteries or endocardially adjacent to the right coronary artery in a swine model has suggested that coronary artery spasm (that does not immediately respond to nitroglycerin) can be induced.21 In addition, medial fibrosis was noted for the first time. The clinical relevance of these findings remains to be elucidated.
In another model using 6-month-old pigs, a circular electroporation catheter delivering 200 J applications inside a PV was compared with a RF ablation catheter delivering 30W inside another PV of the same animal; the PVs treated with electroporation actually increased in size as expected with growth of the animal, while those treated with RF energy reduced in diameter.17 Subsequent preclinical work using a pentaspline Farawave catheter (Boston Scientific) vs a RF ablation catheter in a swine model confirmed these earlier findings.22 Both monophasic and biphasic PFA waveforms were performed and compared with RF energy for ablative effect, histologic analysis, and collateral damage. Biphasic waveforms had 100% efficacy and greater durability than monophasic and RF energy for PV and superior vena cava isolation. There was no phrenic nerve palsy or PV stenosis noted. Other ablation catheters have been studied in swine models, including a circular multielectrode ablation catheter (PVAC Gold, Medtronic) and lattice electrode catheter (Sphere-9, Affera, a Medtronic company), with similar outcomes.23,24
Clinical Pilot Studies
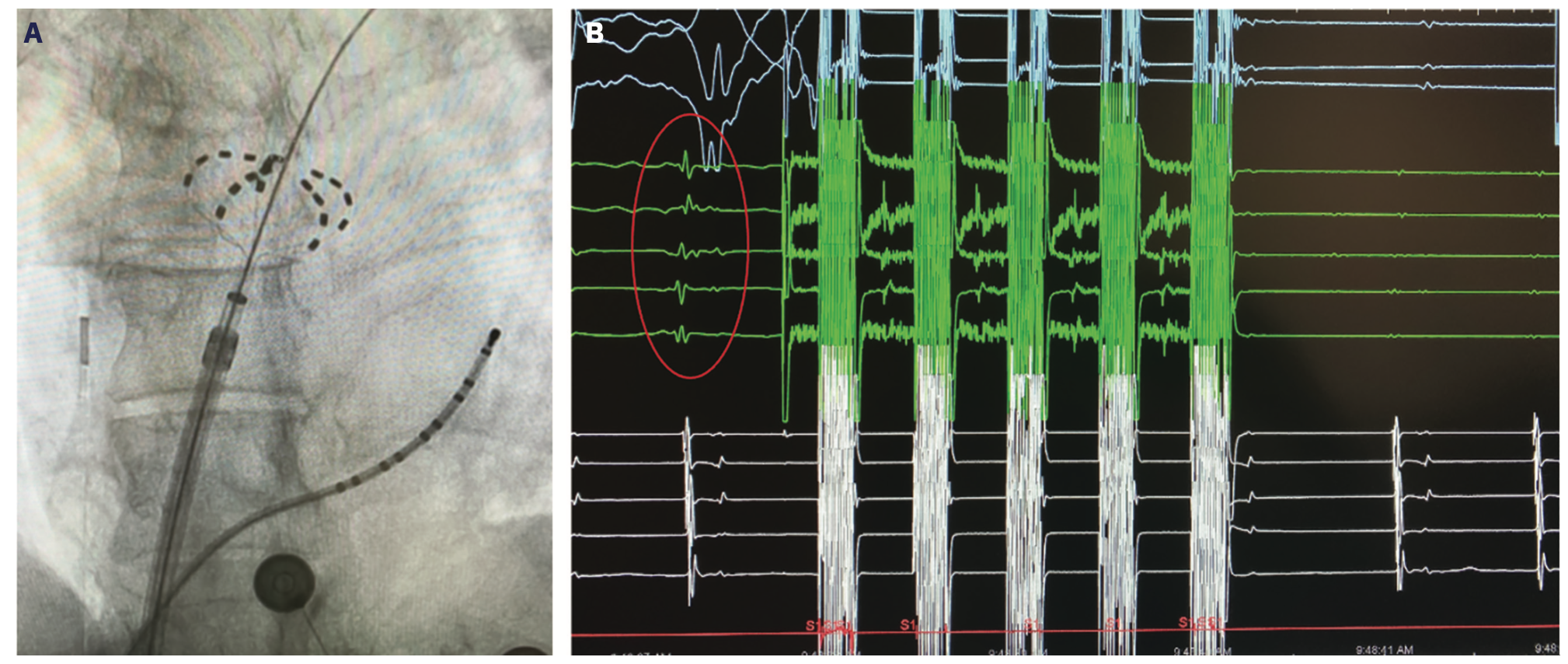
Reddy et al reported the first clinical experience in 22 patients with paroxysmal AF using pulsed electric field ablation for PVI (15 endocardial and 7 epicardial).25 Catheter-based PV isolation using the Farawave catheter was 100% successful using a total electroporation delivery time of less than 60 seconds per patient (Figure 1). The epicardial box lesion was done using a linear catheter around the PVs and successful in 86% of patients using 2 lesions per patient. The IMPULSE (n = 40) and PEFCAT (n = 41) trials also examined patients with paroxysmal AF using both monophasic (IMPULSE) and biphasic (PEFCAT) waveforms with the Farawave catheter.26 PVI was achieved in 100% of patients, with no reconnections noted during the 20-minute waiting period or with provocative adenosine testing. Monophasic waveforms required general anesthesia and paralytic agents because of profound skeletal muscle contraction. The biphasic waveform cases were better tolerated due to less contraction and performed under conscious sedation. In follow-up, no patients had phrenic nerve palsy, esophageal injury, or PV stenosis.27 A 1-year follow-up study showed durable PVI in 84.8% of PVs remapped at 90 days in 110/121 patients in the IMPUSE, PEFCAT, and PEFCAT II studies.28 Freedom from atrial arrhythmias at 1 year in the entire cohort was 78.5 ± 3.8%. The PULSED AF Pilot Trial (n = 38) for paroxysmal AF using the PulseSelect PFA System (Medtronic) also showed 100% acute PV isolation with no adverse events such as phrenic nerve injury, esophageal injury, or stroke.29 The single-arm, multicenter PersAFOne study in persistent AF patients from Homolka Hospital in Prague, Czech Republic, and Clinical Hospital Center Split in Split, Croatia, used the pentaspline Farawave catheter for PVI and posterior wall isolation (PWI) and a focal PFA catheter (Faraflex, Boston Scientific) for cavotricuspid isthmus (CTI) ablation.30 Acute isolation of the PVs and PW was achieved in all 25 patients and CTI block was achieved in 13/13 patients. Postprocedural esophagogastroduodenoscopy and computed tomography scans showed no evidence of esophageal injury or PV stenosis. Invasive remapping in 22/25 patients showed 96% of PVs isolated at 3 months and 21/21 PWs were isolated. Another trial that used the lattice tip catheter in a first-in-human experience showed that the Sphere-9 catheter could be used to toggle between RF and PFA or use PFA alone in both paroxysmal and persistent AF patients with good efficacy and safety.31 Loh et al similarly showed that PFA using a proprietary 14-polar single-shot circular catheter could achieve acute bidirectional isolation in 10 patients in another first-in-man study.32
IDE Clinical Trials
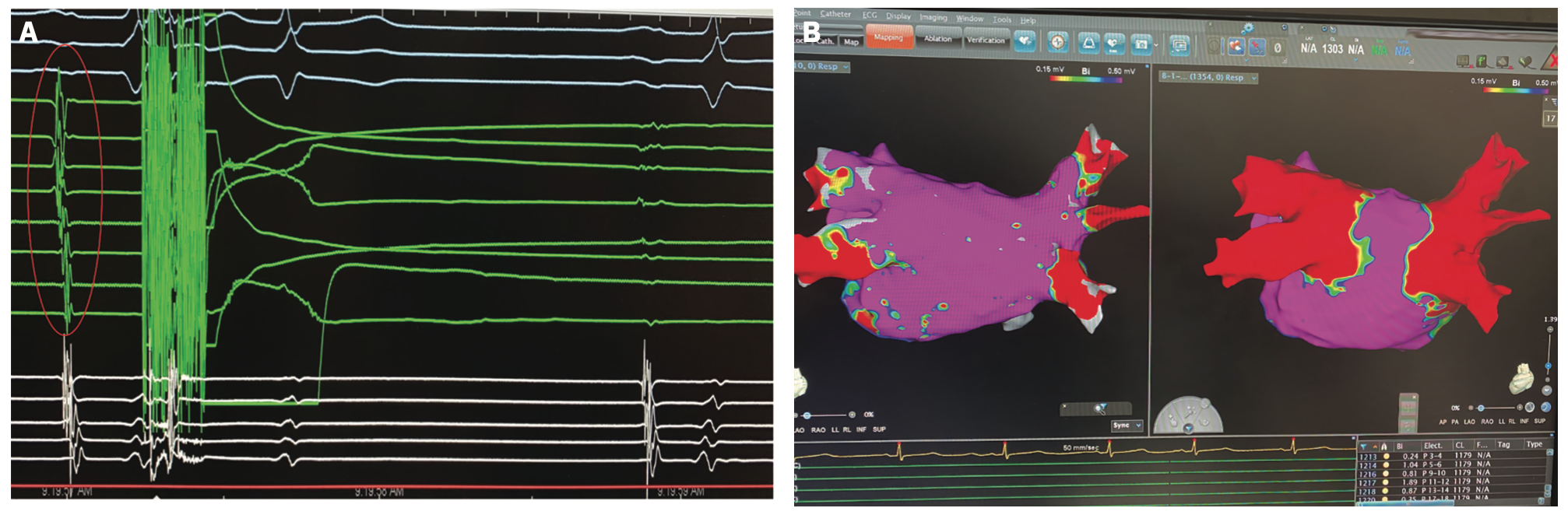
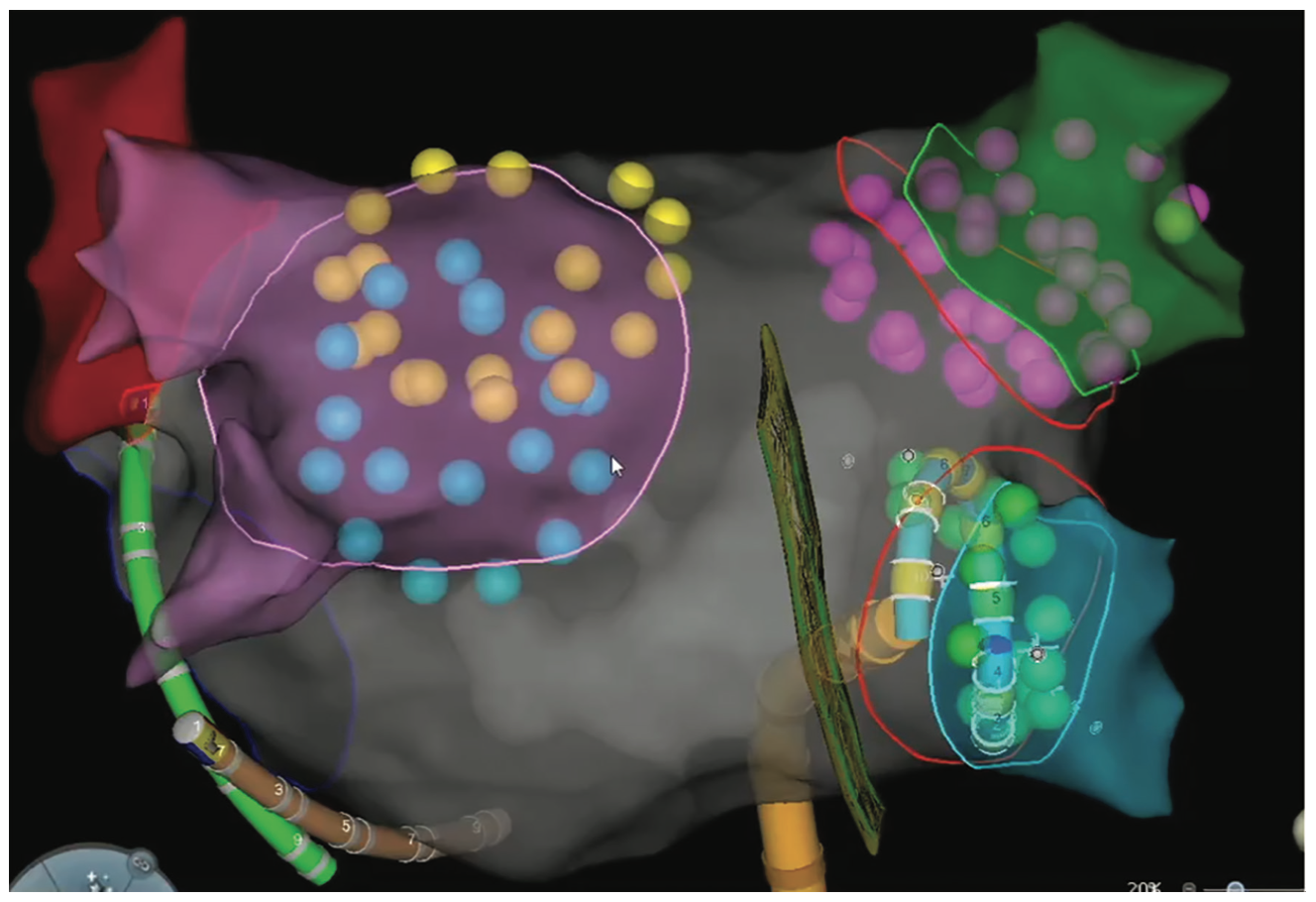
In the United States and internationally, there are over 20 trials listed as active on www.clinicaltrials.gov for PFA in patients with AF. Many of the trials are exclusive to international sites in Europe or Asia. Three clinical trials with sites in the United States are active and recently finished recruiting. The ADVENT trial compared the Farapulse PFA System to current standard of care ablation systems (RF or cryoablation) in paroxysmal AF. The PULSED AF study was a single-arm study using the PulseSelect PFA System in either paroxysmal or persistent AF patients (Figure 2). The admIRE study evaluated a circular multielectrode PFA catheter (VariPulse, Biosense Webster, Inc, a Johnson & Johnson company) in a single-arm study of paroxysmal AF patients (Figure 3). Ongoing and actively recruiting studies include the Sphere-9 lattice PF/RF system compared to RF ablation in a 1:1 randomization in persistent AF patients in the SPHERE Per-AF trial.
Limitations and Future Directions
There is still limited data on the long-term efficacy of PFA. There is justifiable concern that some of the immediate elimination of voltage seen with electroporation could be falsely reassuring and even reversible, particularly if a proper field strength is not used. It is also conceivable that enthusiasm about the safety profile of PFA may lead to an increased number of lesions delivered in the atria, which could lead to atrial mechanical dysfunction or be proarrhythmic. Outcome studies of smaller pilot studies have been encouraging at 1 year, but these are with small numbers of patients at select centers. In addition, there are a variety of catheters and pulsed field generators in development; it remains to be seen which catheter or energy delivery algorithm will be superior.
The safety of PFA has been one of its most attractive features. However, there was a recent report of coronary vasospasm when PFA was delivered for a mitral isthmus line, provoking acute left circumflex artery occlusion.33 CTI ablation with a pentaspline PFA catheter also provoked severe subtotal vasospasm of the right coronary artery in 100% (5/5) patients and was relieved with nitroglycerin in the absence of ST elevation.34 In addition, microbubbles have been observed using intracardiac echocardiography during PFA delivery.25 It is still unknown whether this could be linked to cerebral embolic events, although none were seen in early trials when screening magnetic resonance imaging (MRIs) were performed.26 There were silent cerebral lesions and events (noted by MRI) with the lattice catheter (Sphere-9) in the first-in-man study, but there were activated clotting time target differences noted in those with and without lesions.31
As additional single-center and registry data are collected, real-world experience with this technology is being gathered. The 5S study looked at 191 consecutive patients who underwent PFA for AF using the Farawave catheter in Frankfurt, Germany.35 Procedure times were noticeably shorter than current standards, averaging 39 minutes. However, cerebral MRIs did show asymptomatic injury in 10/53 patients (19%). There were 2 strokes as well, although they were linked to air embolism.
Transient right phrenic nerve palsy was also reported in 3 patients who underwent PFA for AF after delivery in the right superior PV.36 Fortunately, all recovered spontaneously in less than 1 minute. Two patients in the 5S study also had transient phrenic nerve paralysis. Many of the IDE trials exclude patients with devices and even intracoronary stents because of a theoretical risk of channeling current and the safety of PFA of patients with hardware in the heart is still unknown. When electroporation has been looked at in other settings, such as the hepatic system, metal stents have been shown to channel current.37
The largest multinational survey on postapproval use of PFA was the MANIFEST-PF study, which has confirmed much of the initial enthusiasm for PFA regarding efficacy and, for the most part, safety as well.38 At 24 sites, 1758 patients with paroxysmal or persistent AF who underwent PFA with the Farawave catheter (after it was clinically approved in Europe) were included in a retrospective survey. Acute PVI was achieved in 99.9%, with mean procedure times of about 1 hour. There was no esophageal injury or PV stenosis reported, which was reassuring. However, there were 8 (.46%) cases of transient phrenic nerve injury that resolved intraprocedurally or by the next day. There was 1 case of coronary artery spasm at the posterior mitral annulus. There were also 7 strokes (1 of which was fatal), but a number of them were attributed to poor sheath management or underlying conditions. There were 114 patients of 1748 who received routine postprocedural MRIs, and the rate of asymptomatic MRI abnormalities in those patients was 17.5%. There were no neurologic sequelae noted. There were also other non-PFA-related complications such as tamponade (.97%) and vascular hematomas (2.44%), which may be related more to operator issues rather than PFA.
Conclusion
It is no doubt an exciting time in the field of AF ablation, with PFA poised to be one of its most consequential developments in the last 10 years. There has been a wealth of promising animal and early clinical data gathered thus far, and we look forward to the definitive randomized clinical trial data that lies ahead.
Disclosures: The author has completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Patel has no conflicts of interest to report regarding the content herein. Outside the submitted work, Dr Patel reports payment or honoraria as a fellows program speaker for Biosense Webster, and leadership or fiduciary role for the Heart Rhythm Society’s membership committee.
References
1. Calkins H, Hindricks G, Cappato R, et al. 2017 HRS/EHRA/ECAS/APHRS/SOLAECE expert consensus statement on catheter and surgical ablation of atrial fibrillation. Heart Rhythm. 2017;14(10):e275-e444. doi:10.1016/j.hrthm.2017.05.012
2. Haïssaguerre M, Jaïs P, Shah DC, et al. Spontaneous initiation of atrial fibrillation by ectopic beats originating in the pulmonary veins. N Engl J Med. 1998;339(10):659-666. doi:10.1056/NEJM199809033391003
3. Al-Sakere B, André F, Bernat C, et al. Tumor ablation with irreversible electroporation. PLoS One. 2007;2(11):e1135. doi:10.1371/journal.pone.0001135
4. Batista Napotnik T, Polajžer T, Miklavčič D. Cell death due to electroporation – a review. Bioelectrochemistry. 2021;141:107871. doi:10.1016/j.bioelechem.2021.107871
5. Mir LM. Therapeutic perspectives of in vivo cell electropermeabilization. Bioelectrochemistry. 2001;53(1):1-10. doi:10.1016/s0302-4598(00)00112-4
6. Davalos RV, Mir LM, Rubinsky B. Tissue ablation with irreversible electroporation. Ann Biomed Eng. 2005;33(2):223-231. doi:10.1007/s10439-005-8981-8
7. Rubinsky B. Irreversible electroporation in medicine. Technol Cancer Res Treat. 2007;6(4):255-259. doi:10.1177/153303460700600401
8. Rubinsky B, Onik G, Mikus P. Irreversible electroporation: a new ablation modality — clinical implications. Technol Cancer Res Treat. 2007;6(1):37-48. doi:10.1177/153303460700600106
9. Zager Y, Kain D, Landa N, Leor J, Maor E. Optimization of irreversible electroporation protocols for in-vivo myocardial decellularization. PLoS One. 2016;11(11):e0165475. doi:10.1371/journal.pone.0165475
10. van den Bos W, Scheffer HJ, Vogel JA, et al. Thermal energy during irreversible electroporation and the influence of different ablation parameters. J Vasc Interv Radiol. 2016;27(3):433-443. doi:10.1016/j.jvir.2015.10.020
11. Lavee J, Onik G, Mikus P, Rubinsky B. A novel nonthermal energy source for surgical epicardial atrial ablation: irreversible electroporation. Heart Surg Forum. 2007;10(2):E162-E167. doi:10.1532/HSF98.20061202
12. Kaminska I, Kotulska M, Stecka A, et al. Electroporation-induced changes in normal immature rat myoblasts (H9C2). Gen Physiol Biophys. 2012;31(01):19-25. doi:10.4149/gpb_2012_003
13. Wittkampf FH, van Driel VJ, van Wessel H, et al. Feasibility of electroporation for the creation of pulmonary vein ostial lesions. J Cardiovasc Electrophysiol. 2011;22(3):302-309. doi:10.1111/j.1540-8167.2010.01863.x
14. Sugrue A, Maor E, Ivorra A, et al. Irreversible electroporation for the treatment of cardiac arrhythmias. Expert Rev Cardiovasc Ther. 2018;16(5):349-360. doi:10.1080/14779072.2018.1459185
15. Wojtaszczyk A, Caluori G, Pešl M, Melajova K, Stárek Z. Irreversible electroporation ablation for atrial fibrillation. J Cardiovasc Electrophysiol. 2018;29(4):643-651. doi:10.1111/jce.13454
16. Li W, Fan Q, Ji Z, Qiu X, Li Z. The effects of irreversible electroporation (IRE) on nerves. PLoS One. 2011;6(4):e18831. doi:10.1371/journal.pone.0018831
17. van Driel VJ, Neven KG, van Wessel H, et al. Pulmonary vein stenosis after catheter ablation. Circ Arrhythm Electrophysiol. 2014;7(4):734-738. doi:10.1161/circep.113.001111
18. Neven K, van Driel V, van Wessel H, et al. Safety and feasibility of closed chest epicardial catheter ablation using electroporation. Circ Arrhythm Electrophysiol. 2014;7(5):913-919. doi:10.1161/CIRCEP.114.001607
19. Neven K, van Es R, van Driel V, et al. Acute and long-term effects of full-power electroporation ablation directly on the porcine esophagus. Circ Arrhythm Electrophysiol. 2017;10(5):e004672. doi:10.1161/CIRCEP.116.004672
20. du Pré BC, van Driel VJ, van Wessel H, et al. Minimal coronary artery damage by myocardial electroporation ablation. Europace. 2012;15(1):144-149. doi:10.1093/europace/eus171
21. Koruth JS, Kawamura I, Buck E, Jerrell S, Brose R, Reddy VY. Coronary arterial spasm and pulsed field ablation. JACC Clin Electrophysiol. 2022;8(12):1579-1580. doi:10.1016/j.jacep.2022.06.015
22. Koruth JS, Kuroki K, Kawamura I, et al. Pulsed field ablation versus radiofrequency ablation. Circ Arrhythm Electrophysiol. 2020;13(3):e008303. doi:10.1161/circep.119.008303
23. Stewart MT, Haines DE, Verma A, et al. Intracardiac pulsed field ablation: proof of feasibility in a chronic porcine model. Heart Rhythm. 2019;16(5):754-764. doi:10.1016/j.hrthm.2018.10.030
24. Yavin H, Shapira-Daniels A, Barkagan M, et al. Pulsed field ablation using a lattice electrode for focal energy delivery. Circ Arrhythm Electrophysiol. 2020;13(6):e008580. doi:10.1161/circep.120.008580
25. Reddy VY, Koruth J, Jais P, et al. Ablation of atrial fibrillation with pulsed electric fields. JACC Clin Electrophysiol. 2018;4(8):987-995. doi:10.1016/j.jacep.2018.04.005
26. Reddy VY, Neuzil P, Koruth JS, et al. Pulsed field ablation for pulmonary vein isolation in atrial fibrillation. J Am Coll Cardiol. 2019;74(3):315-326. doi:10.1016/j.jacc.2019.04.021
27. Kuroki K, Whang W, Eggert C, et al. Ostial dimensional changes after pulmonary vein isolation: pulsed field ablation vs radiofrequency ablation. Heart Rhythm. 2020;17(9):1528-1535. doi:10.1016/j.hrthm.2020.04.040
28. Reddy VY, Dukkipati SR, Neuzil P, et al. Pulsed field ablation of paroxysmal atrial fibrillation. JACC Clin Electrophysiol. 2021;7(5):614-627. doi:10.1016/j.jacep.2021.02.014
29. Verma A, Boersma L, Haines DE, et al. First-in-human experience and acute procedural outcomes using a novel pulsed field ablation system: the PULSED AF pilot trial. Circ Arrhythm Electrophysiol. 2022;15(1):e010168. doi:10.1161/circep.121.010168
30. Reddy VY, Anic A, Koruth J, et al. Pulsed field ablation in patients with persistent atrial fibrillation. J Am Coll Cardiol. 2020;76(9):1068-1080. doi:10.1016/j.jacc.2020.07.007
31. Reddy VY, Anter E, Rackauskas G, et al. Lattice-tip focal ablation catheter that toggles between radiofrequency and pulsed field energy to treat atrial fibrillation: a first-in-human trial. Circ Arrhythm Electrophysiol. 2020;13(6):e008718. doi:10.1161/circep.120.008718
32. Loh P, van Es R, Groen MHA, et al. Pulmonary vein isolation with single pulse irreversible electroporation: a first in human study in 10 patients with atrial fibrillation. Circ Arrhythm Electrophysiol. 2020;13(10):e008192. doi:10.1161/CIRCEP.119.008192
33. Gunawardene MA, Schaeffer BN, Jularic M, et al. Coronary spasm during pulsed field ablation of the mitral isthmus line. JACC Clin Electrophysiol. 2021;7(12):1618-1620. doi:10.1016/j.jacep.2021.08.016
34. Reddy VY, Petru J, Funasako M, et al. Coronary arterial spasm during pulsed field ablation to treat atrial fibrillation. Circulation. 2022;146(24):1808-1819. doi:10.1161/circulationaha.122.061497
35. Schmidt B, Bordignon S, Tohoku S, et al. 5S study: Safe and simple single shot pulmonary vein isolation with pulsed field ablation using sedation. Circ Arrhythm Electrophysiol. 2022;15(6):e010817. doi:10.1161/circep.121.010817
36. Pansera F, Bordignon S, Bologna F, et al. Catheter ablation induced phrenic nerve palsy by pulsed field ablation—completely impossible? A case series. Eur Heart J Case Rep. 2022;6(9):ytac361. doi:10.1093/ehjcr/ytac361
37. Agnass P, van Veldhuisen E, Vogel JA, et al. Thermodynamic profiling during irreversible electroporation in porcine liver and pancreas: a case study series. J Clin Transl Res. 2020;5(3):109-132. doi:10.18053/jctres.05.202003
38. Ekanem E, Reddy VY, Schmidt B, et al. Multi-national survey on the methods, efficacy, and safety on the post-approval clinical use of pulsed field ablation (MANIFEST-PF). Europace. 2022;24(8):1256-1266. doi:10.1093/europace/euac050

