

Comparison of Safety and Efficacy of Two Different Transseptal Puncture Devices: Discussion With Bradley Knight, MD, and Amin Al-Ahmad, MD
© 2023 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of EP Lab Digest or HMP Global, their employees, and affiliates.
EP LAB DIGEST. 2023;23(11):20-22.
Bradley Knight, MD, and Amin Al-Ahmad, MD, discuss the outcomes of their recent study which compared the safety and efficacy of transseptal puncture using a purpose-built radiofrequency (RF) wire solution (VersaCross™ Access Solution, Baylis Medical, now Boston Scientific) to a mechanical needle with and without electrification (AcQCross™ Transseptal Access System, now rebranded as FlexCath Cross™ Transseptal Solution, Medtronic). Gain insights into their experiences using these solutions throughout the study, as well as their thoughts on the future of transseptal puncture techniques and technology.

Bradley Knight, MD: My name is Brad Knight. I am the Director of Cardiac Electrophysiology at Northwestern Medicine in Chicago, Illinois.

Amin Al-Ahmad, MD: Hi, I am Amin Al-Ahmad. I am one of the Cardiac Electrophysiologists at Texas Cardiac Arrhythmia in Austin, Texas.
Can you speak to the history of performing transseptal puncture?
Knight: Transseptal catheterization is an increasingly performed procedure, but I can recall in the mid-1990s when it was in the purview of the cardiac interventional cardiologists who were often performing mitral valvuloplasty. For patients with Wolff-Parkinson-White, we would routinely get access to the left heart going retrograde. It was not until atrial fibrillation (AF) ablation started in the late 1990s to early 2000s that electrophysiologists really became proficient at transseptal catheterization. We are now the experts in transseptal catheterization in the hospital, given how many AF ablation procedures and other left-sided procedures such as appendage closure that we do. I am sure Amin has had that same experience.
Al-Ahmad: Yes, early on we would call the interventionalists down to do it. But one of the things that changed was the onset of using intracardiac echocardiography (ICE). Once we started to use ICE, we began to do more and more of these. Over the last few years, it has been electrophysiologists who primarily do transseptals.
When did RF energy start to be used when performing transseptal puncture?
Knight: I can recall a story when I was at the University of Chicago over 15 years ago when a patient was referred for a left-sided arrhythmia. The physician had tried to go transseptal but was unable to. So, the patient was essentially referred because of a failed transseptal ablation. There was a powered wire that was made by Baylis Medical at the time, so I contacted them. They brought a powered dedicated Baylis needle for that case, and we went transseptal. After the case was over, which went very smoothly, they notified our team that we were the first ones to use their RF energy needle. We did not know it at the time. They were a small company back then that were developing powered needles dedicated for delivering energy to the tip of the needle.
Al-Ahmad: For us, it was about 15 years ago when we had a similar experience and they brought us the RF needle. It was an “aha” moment for me when we first used it. It was so much less force and so much easier to cross transseptal. It was one of those things where once it was done, we thought, “This is great. This is how we should be doing things.” It changed how we do things, for sure.
Knight: I agree. It changed as a whole group. Like many things, it is a little more expensive, but once physicians used it for the first time, it was difficult to go back to what we were doing before.
Why did RF energy start to be used when performing transseptal puncture?
Knight: RF energy started to be used for transseptal puncture for a variety of reasons. When we do transseptal catheterization with a mechanical needle, most of the cases go very smoothly. I think it is a way to minimize the outliers. There are times when a mechanical needle will have difficulty crossing, usually because the septum / fossa ovalis is very tough. It can look thick and be hard to cross, but sometimes it does not look thick on ICE and can still be difficult to cross if it is a repeat procedure. I suspect that because there was experience in the pediatric population with crossing baffles with energized wires, that someone came up with the notion of electrifying the needle in a very safe way to improve its ability and reliability in crossing during transseptal puncture.
Al-Ahmad: I agree. It solved a real need for electrophysiologists. The vast majority of these cases go very smoothly, but occasionally you have to cross, and as the needle goes into the left atrium, you must pull back very quickly and make sure that you do not perforate on the other side, or anything like that. Therefore, having a little more predictability and reliability with crossing was something we needed. Again, most cases were fine, but what you do not want is to have those cases where a small thing can create a big complication. So, it really did help. It solved one of our needs as electrophysiologists.
What are some of the current considerations when it comes to using transseptal tools today?
Knight: That is a great question. Like many institutions, we have moved entirely to a dedicated RF energy system, whether it is a needle or a wire. I have recently discovered that my colleagues have mostly moved to a dedicated RF wire, typically with a VersaCross wire (Figure 1). I continue to use the Baylis dedicated RF energy needle (NRG™ Transseptal Needle) fairly routinely and use the wire (VersaCross Access Solution) when I think it is going to be a difficult case based on what I see on ICE. Whether a patient has pacing leads, I think sometimes is a good reason to use a wire. You are less likely to interfere with the pacing leads as you come down from the superior vena cava.
So, I think we have moved as a group exclusively to that. But you sometimes have to make a decision on the fly as to what the best transseptal tool is. There are cases where you can get the needle to cross, and you just cannot get that dilator to go with it. You can apply additional force, but the dilator will not follow the needle. An alternative in that case is to use a dedicated powered wire. Once the wire is across, you have a better rail. Therefore, I think both at the beginning of the procedure based on historical information, whether it is a redo, what you see on ICE, and what you are experiencing in terms of troubleshooting is how we decide what tool to use.
Al-Ahmad: I would agree with that. For us, the main consideration is the safety of the procedure and then efficacy of getting across. We have had a similar experience where the majority of us will use the NRG electric needle (NRG Transseptal Needle), but over time, many have now gone to the dedicated RF energy system, the VersaCross, for similar reasons. I think it depends on what you see anatomically in terms of what tool you may want to use. But again, I think that with both of those, the primary objective is to cross as safely as possible. So, with the dedicated RF energy system in general, you really do not have to push as hard to do your tenting. Once you are across, it is fairly straightforward. However, in cases where it is difficult to cross, such as not being able to get the sheath across because of septal thickening, then having that wire is really helpful, because that is a good rail to get across almost anything.
What is purpose-built RF?
Knight: That term is a way to differentiate tools that have been designed from the ground up to be compatible with dedicated energy delivery rather than applying energy in an off-the-shelf way. You can take a mechanical needle and, in particular, if you have difficulty crossing the needle with a lot of force, you can apply RF or electrical current with a Bovie to the needle that is in your hand. Because it is insulated in the dilator all the way up, it will deliver current to any part of that needle that is exposed on the other end.
The same can be applied to the use of guidewires. For reasons we will discuss in a bit, there are certainly some risks of doing that and they were not designed for that purpose. So, although you may be able to get away with it in some cases, dedicated systems were built from the ground up with very specific engineering specifications that allow very concentrated energy and current to be delivered to the tip. So, you get a high current density for a very brief period of time that allows you to reliably and successfully cross into the left atrium. Amin, can you comment on this? I know that there are some places that do this type of off-label, non-dedicated approach. What is your take?
Al-Ahmad: I agree. It is interesting—we go to a lot of different hospitals and hospital systems, and I can recall going to certain places and them not having, for example, a dedicated system available. In which case, you use a mechanical standard transseptal needle. Most of the time, it works just fine. But there are times when you are doing a redo or it is a difficult transseptal, and you cannot safely cross. In those cases, you can do this off-label technique. But when we have done that, particularly with a lot of the data that has been generated over the years, it is a little uncomfortable. I think that we have essentially pushed those hospital systems to move towards a safer approach, which is a dedicated RF needle approach. So, most of the time now, wherever we go, we will have that available, primarily for those reasons. It is doable, but I do not think it is the right thing to do anymore with what we know.
Can you tell us about the study you conducted comparing purpose-built RF technology and mechanical/electrified needles?
Knight: Yes, let me talk about the study that we have done looking at purpose-built or dedicated RF wires compared to other tools. With the use of electrified needles and wires, we have been working over the years with our industry colleagues and doing some experiments supported by Baylis Medical to look at what happens with those approaches. What we have learned is that first of all, when you apply electrocautery or a Bovie to the end of a mechanical needle that has an end hole on it while you are advancing it across the septum, you are capable of coring tissue. We worry about that tissue embolizing, obviously. So, depending on the thickness of that tissue, whether in the experiments we crossed a thin fossa ovalis, a thick part of the intra-atrial septum, or for experimental reasons like a thicker structure like the aorta, the incidence of coring ranged from about 30%-50%.
We also know that if you use a wire and you apply energy to it, such as with the standard .035” wire or even an .012” wire, you can get charring, you can get inability to cross, and you can actually get melting at the tip of the dilator if there is too much wire exposed.
So, the recent experiment was to look at a newly commercially available tool, the AcQCross needle. It is a very interesting device because like many of these tools, it saves you steps of access wire and exchanging. The fewer exchanges we do when we do a transseptal catheterization, the better. This is a dilator system that with the advancing at the handle, ejects the tip of the needle through that. It is a built-in needle. Once you cross with that needle, you can place a guidewire through the end of that needle. So, you go up like a standard transseptal catheterization, bring the tip of the dilator down to the fossa ovalis, puncture with the needle, and then put a wire through. It is a very slick system in that regard. It is also permitted to deliver cautery to the end of that needle. Because that needle has an end hole, we wanted to compare what the outcomes were using this integrated needle dilator system with the VersaCross system, which is a purpose-built dedicated RF wire that can come in the form of a J-Tip wire or a Pigtail, and it is connected to a proprietary generator that delivers one second of current.
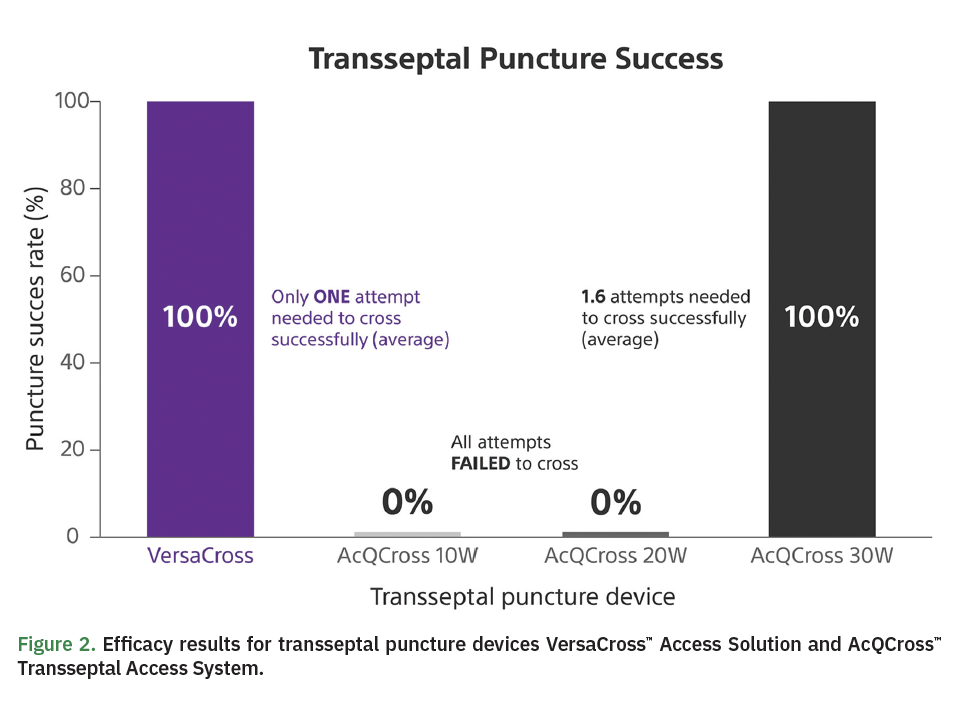
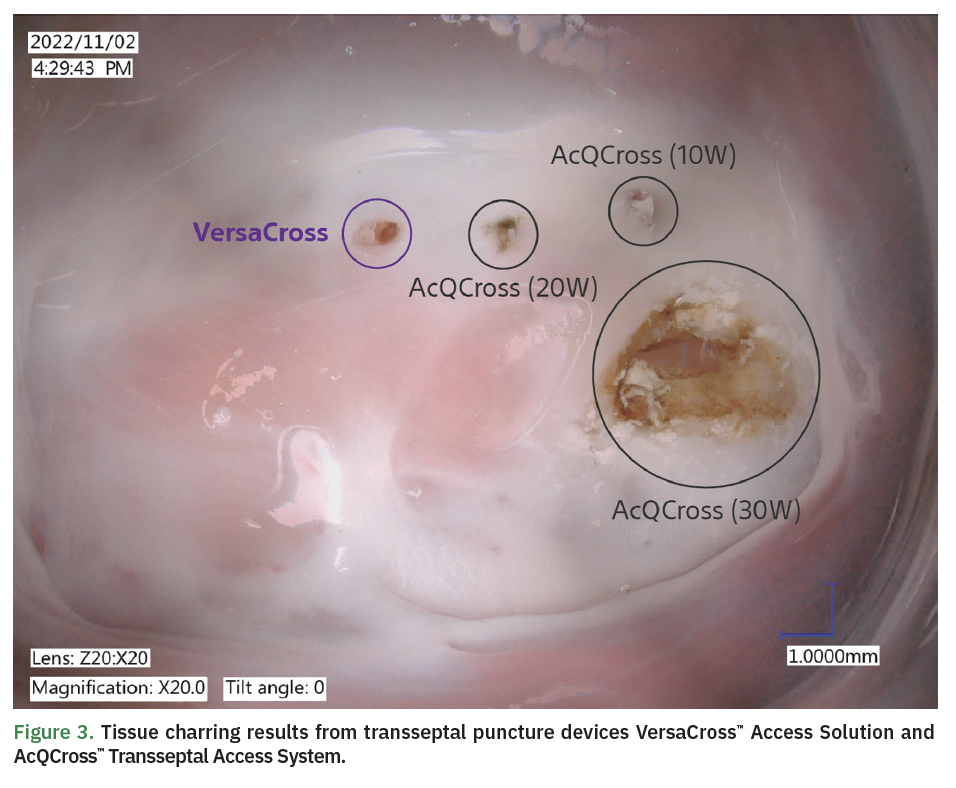
We created a model of a freshly excised porcine atrial septum and put it in a bath of saline initially, and then moved toward an egg white bath because it mimicked the impedance of blood better than saline. We looked at the comparison between the standard VersaCross system and the integrated needle system (AcQCross) with power. Without getting into all the details, and we can refer the listeners to a poster that we presented at the AF Symposium 2023 that better summarizes the data.1 When we applied energy to the dedicated VersaCross wire, we crossed in the first try in every case. There was no charring, and it left a very small hole on the interatrial septum. When we used the AcQCross needle, when we tried it mechanically, the force that was required to cross compared to VersaCross was about 6 times as high, about 1.2 newtons versus 0.2 newtons. For the purpose of the experiment, we did not mechanically cross and instead applied energy. Instructions for use are about 10 watts for 2 seconds. We tried that about 5 times. If that did not work, we went to 20 watts, since some physicians are apparently using 20 watts. If that failed after 2 attempts, we went to 30 watts. What we found is that it (AcQCross) never crossed at 10 watts and much higher energies were required. It was inconsistent when it would cross; it would require 30 watts to cross in most cases (Figure 2). When this happened, we found that there was coring just like we were concerned about. Because it is an end hole needle, there was coring, and there was also charring at the site of crossing and a larger hole (Figure 3).
The coring part was very interesting from an experimental standpoint. In this model, we wanted to be sure we were really coring tissue, and in the cores that we were generating after we would inject saline at the tip of the needle, we would expel what looked like a core. We needed to be sure we were not just coring egg white because it will also look like protein and dark matter. So, we did 2 things besides looking at it under a microscope. These were actually sent to a pathologist, who looked for myocardial cells in the expelled tissue, and we were able to confirm that what we thought was visually a core from the atrial septum, was indeed a core, in most cases, and not an egg white.
Then, to be confident that our data were reliable, transseptal punctures using this system and electrification were performed in live swine models, which also replicated the findings that coring was occurring in these. It is kind of a long description, but I think the dedicated VersaCross wire is very reproducible and safe. The AcQCross needle is very effective and sharp, but it does require more force. When you use electrification, you are going to have coring and possibly charring.
Al-Ahmad: The data that I have seen you conduct over the years with different systems is compelling from the perspective of if you are trying to cross with an electrified needle, to use the dedicated RF needle rather than try to piece something together. Some people either piece together the wire or a non-dedicated needle. However, using the dedicated needle does matter in terms of safety. I think that is compelling to the hospital systems as well as physicians.
What were the conclusions of your study in terms of safety and efficacy?
Knight: Both the VersaCross and the AcQCross are effective tools, but I worry that if power is delivered to the AcQCross needle because it has an end hole needle, you can get coring. That is probably infrequently needed, but based on the data we saw, it is not advised.
Another thing to expand on is in terms of tools, the VersaCross wire and AcQCross needle are being incorporated into other systems. For example, when we do left atrial appendage closure with the WATCHMAN™ device (Boston Scientific), we can do a standard transseptal catheterization and exchange. We now have access to a large bore access transseptal dilator that is manufactured by Boston Scientific (formerly Baylis Medical) that has the dedicated RF wire that you can use to cross and then do one exchange. Or, it is now integrated with the WATCHMAN FXD Curve™ Access System so that you can go straight up and cross with that with a single puncture / single crossing (Figure 4).
Al-Ahmad: That really does help us become more efficient and save some time. The nice thing is it (VersaCross) is going to be incorporated into some of the other ablation systems that require large sheath access, like the cryo system (Figure 4) or the pulsed field ablation system—that ability to not have to exchange matters. Because every time you exchange, there is a small but real risk of allowing air into the system. So, having that is really helpful.
What do you see as being the main value driver for transseptal tools in the future?
Knight: The value drivers for transseptal tools in the future are ease of use, speed, accuracy, success rates, and the ability to be specific about your target. There are some procedures we do where it matters where you cross. So, I think these tools need to allow you to do that. Another thing is cost. I think all these iterations that have improved the system have gotten a little more expensive. It is important that we continue to have these purpose-built dedicated RF wire systems available at a lower cost for hospitals.
Al-Ahmad: I agree. I think safety is the other one—the ability to do this safely, reproducibly, and effectively are really the value drivers. Hopefully we can achieve that at a lower cost.
Reference
1. Wasserlauf, et al. Abstracts from the 28th Annual International Atrial Fibrillation Symposium, February 2-4, 2023. AFS2023-16. J Cardiovasc Electrophysiol. 2023;34(4):1058-1059. doi:10.1111/jce.15870
This content was published with support from Boston Scientific.
Disclosure: Drs Knight and Al-Ahmad have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Knight discloses he received support for this content through the funded study by Baylis Medical (now Boston Scientific). Dr Al-Ahmad reports consulting fees and payment or honoraria for lectures, presentations, speakers bureaus, manuscript writing, or educational events from Boston Scientific and Medtronic.

