Breast Implants Save Lives: Gunshot Wound to a Silicone Gel Implant
Questions
1. What is the incidence of gunshot injuries involving breast implants?
2. What are the considerations for managing a patient with a gunshot wound to a breast implant?
3. Can a breast implant alter the trajectory of a bullet to the chest?
4. What are the considerations for reconstructing a breast after a gunshot wound?
Case Description
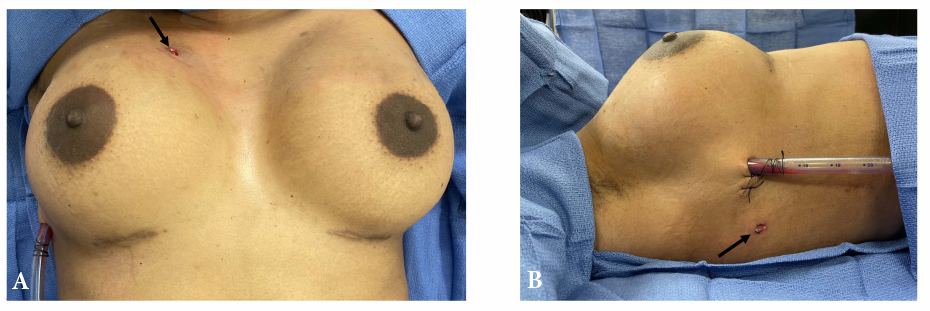
A 31-year-old woman who recently had a breast augmentation presented after sustaining a gunshot wound to the right chest. Ballistic wounds were noted on the anterior and lateral chest walls (Figure 1). Before arrival she underwent needle decompression, which was exchanged for a tube thoracostomy.
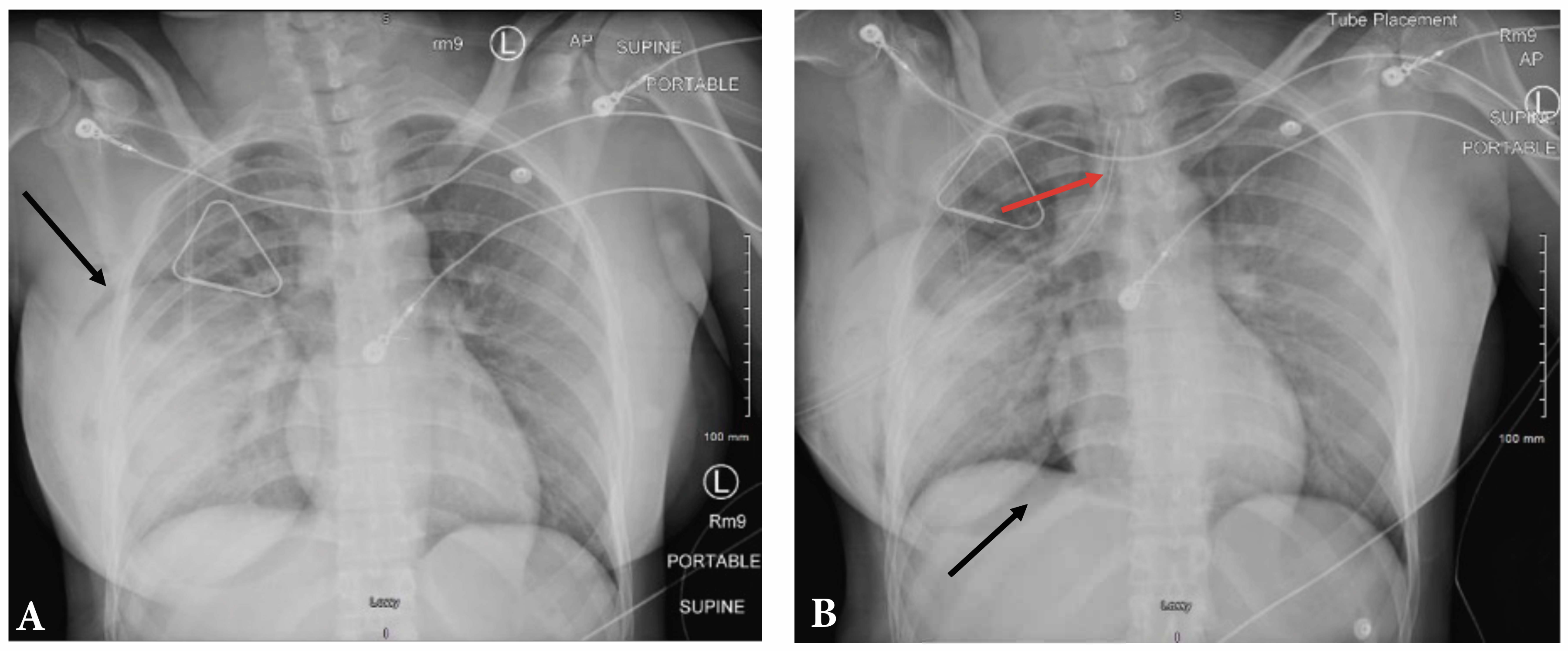
Chest radiographs showed an appropriately placed chest tube with re-expansion of the lung and air surrounding the implant (Figure 2). Computerized tomography revealed the ballistic trajectory, which grazed the right upper lobe of the lung, and demonstrated a small hemopneumothorax, air within and around the breast implant, and comminuted rib fractures (Figure 3A).
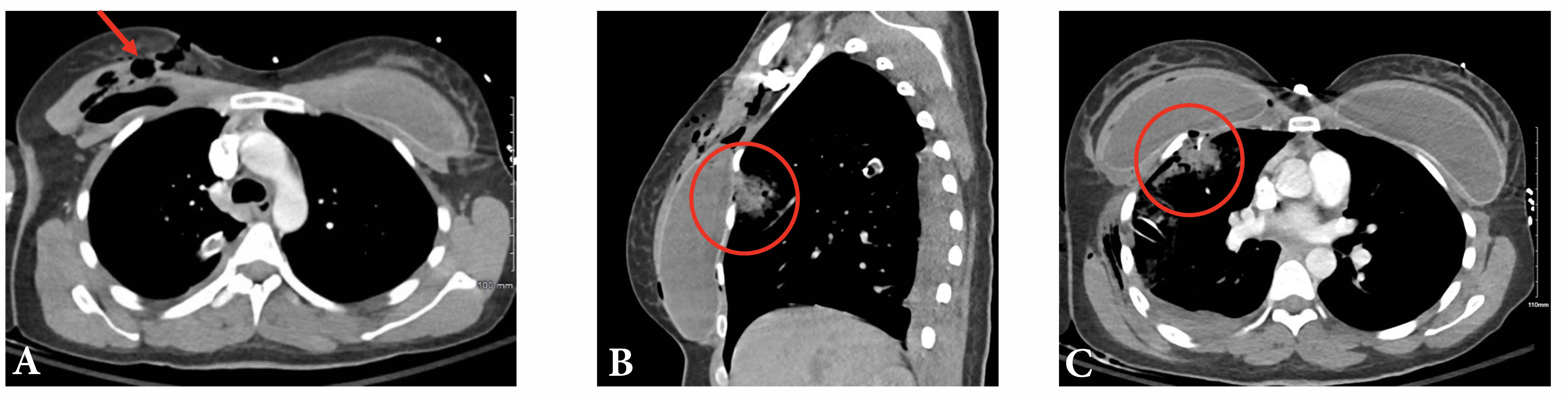
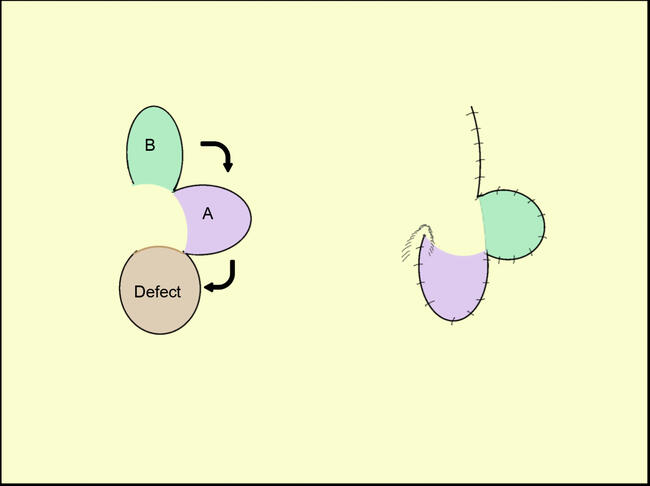
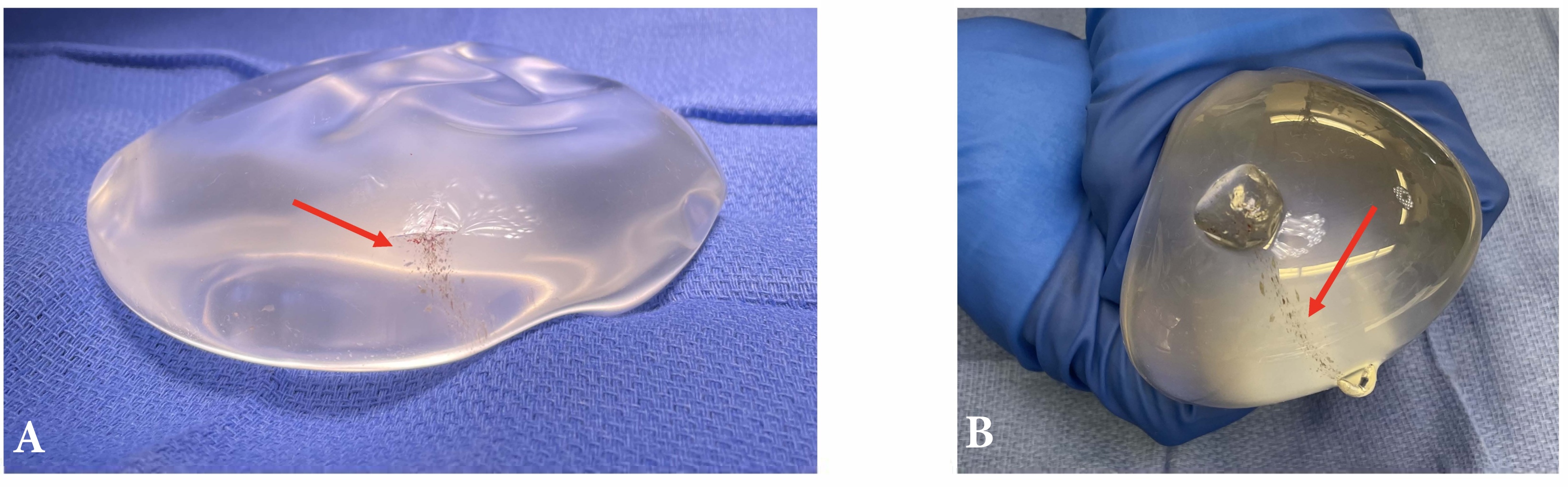
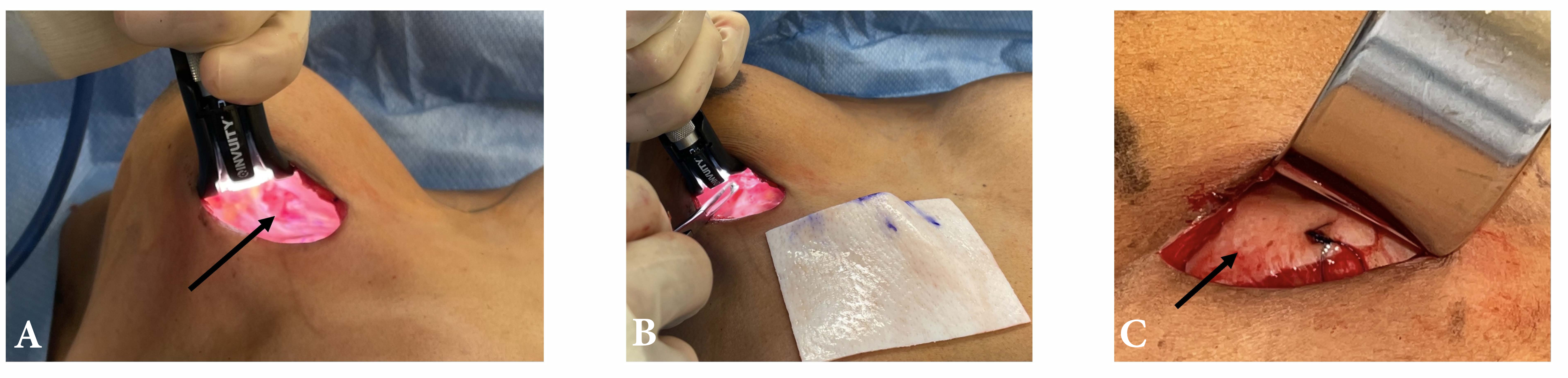
Although the patient’s condition was stable, she underwent wound exploration due to concern of silicone extrusion into the chest cavity (Figure 3B and 3C). The implant appeared to have 2 puncture sites but remarkably held its original shape and composition, with no extrusion of its contents (Figure 4). A hole was noted on the chest wall with sharp exposed rib fragments protruding (Figure 5A). The implant was removed, the fractured ribs were debrided, and the defect was covered with a small biologic mesh (Figure 5B and 5C).
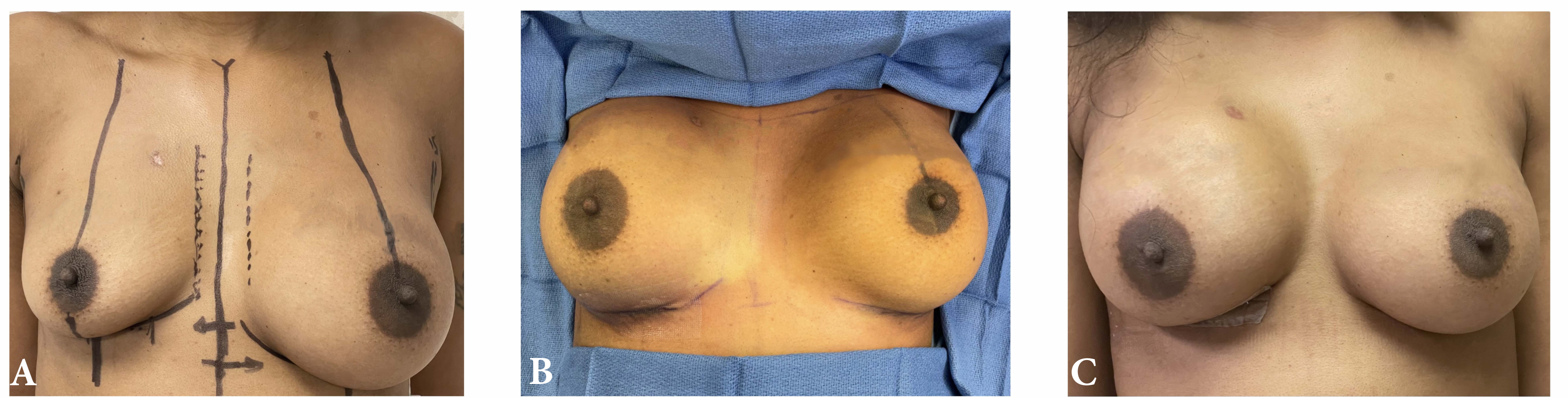
Three months following the injury, the patient’s original implant was replaced with a 360-mL moderate profile Natrelle INSPIRA Smooth Soft Touch (Allergan Aesthetics; Figure 6). She recovered well and is subjectively very happy with her result.
Q1: What is the incidence of gunshot injuries involving breast implants?
Gun violence is a growing epidemic at the forefront of US public health concerns. From 2019 to 2020, the gun death rate rose by a staggering 15%.1 There are more than 100 gun-related deaths every day, with an additional 200 Americans presenting to the emergency department with nonfatal gun-related injuries daily.2 Such nonfatal firearm-related injuries occur most often (72%) among people aged younger than 35 years.3 In assault cases specifically, gunshot wounds to the upper and lower trunk are most common, and these injuries often result in hospitalization.3
Gunshot wounds to the upper trunk may involve breast implants in women who have undergone breast augmentation. It is estimated that between 1 and 2 million women in North America have undergone augmentation mammoplasty.4 According to the American Society of Plastic Surgeons, over 313,000 augmentations and 101,000 breast reconstructions were performed in 2018 alone.5 Despite the increasing prevalence of gun-related injuries and growing numbers of patients with breast implants, statistics regarding gunshot injuries involving breast implants are lacking. There are a few case reports highlighting the management of gunshot wounds involving breast implants,6-9 but no comprehensive studies in the literature exist.
Q2: What are the considerations to managing a patient with a gunshot wound to a breast implant?
For a patient presenting with a gunshot wound to the chest, initial management should include a thorough trauma evaluation followed by any necessary emergent or urgent interventions. Once the patient is stabilized, diagnostic studies to ascertain the extent of injury can be obtained. In this case, the patient’s airway was secure, but she was having trouble breathing due to traumatic pneumothorax from the gunshot wound. With a thoracic-penetrating injury such as this, immediate management via insertion of an intercostal drain is most effective to prevent further respiratory and cardiovascular deterioration. For a patient with breast implants, however, evaluation and avoidance of the implant capsule during any intervention is necessary.
In one case following a stabbing, air accumulated within the capsule of the patient’s breast implant and masked a developing pneumothorax.10 The presence of a swollen breast, subcutaneous emphysema, or marked breast asymmetry should raise suspicion for pneumothorax or hemopneumothorax.10 In another case, a patient’s breast implant was perforated during insertion of a chest tube, after which silicone migrated into her chest cavity and led to an empyema, ultimately requiring ventilation, admission to the intensive care unit, and thoracotomy to evacuate the silicone and decorticate the lung.11 Visualization of silicone before any thoracic intervention should be noted before entering the pleural space.11
Q3: Can a breast implant alter the trajectory of a bullet to the chest?
Literature discussing thoracic gunshot injuries in the presence of breast implants is limited to a few case reports.6-9 In a recent case report describing such an injury, the patient was taken to the operating room emergently where she underwent a pericardial window, which was ultimately negative. She later underwent outpatient implant replacement, at which time multiple shotgun pellets were found within the implant.6 The authors of this case report concluded that the breast implants prevented bullet penetration into the thoracic cavity.6 Another report describing a case of bilateral gunshot wounds to silicone implants suggested the implants likely deflected the bullets’ trajectories.7
The impact of a gunshot is tied to a bullet’s path and placement within the body.12 The extent of the resulting trauma is influenced by multiple factors, one of which being the physical characteristics of the tissue that has been penetrated.12 Thus, if there is some sort of barrier (eg, bone or implant) to slow or deflect a bullet, it may serve as a protective factor. Pannucci et al evaluated the potential protective benefit of breast implants by measuring penetration distance into ballistics gel after gunshot passage through a saline implant, revealing a 20.6% decrease in penetration compared with that seen with no implant.13 Direct bullet velocity reduction and earlier impact (resulting in earlier bullet expansion) by the breast implant may help avoid intrathoracic injury.13 Given the increased viscosity of silicone compared with saline, this protective benefit may be further increased for silicone implants, although no ballistics studies evaluating this potential benefit exist in the literature.
Q4: What are the considerations for reconstructing a breast after a gunshot wound?
After a complete trauma evaluation and patient stabilization, management of the breast implant after a gunshot wound should first involve implant removal. The breast pocket should be debrided of any devitalized tissue and irrigated thoroughly. Inspection of the surrounding chest wall is necessary and may require further intervention or reconstruction. Replacement of the implant may be delayed to ensure resolution of any possible infection,7 although one case reported replacement of the implant during the initial operation without development of infection.9 The patient may decline replacement of the implant and may require removal of the contralateral implant to restore breast symmetry. Capsulectomy may be necessary at the time of implant replacement to ensure proper positioning of the implant within the breast pocket. Follow-up should include monitoring for signs of infection, adequate wound healing, and symmetric breast volume and inframammary folds.
In this case, the patient’s implant was removed, and the breast pocket was debrided and irrigated. Additionally, the fractured ribs were debrided, and the soft tissue defect present on the chest wall was reconstructed using an absorbable mesh. A conservative approach was taken to allow time for the patient to recover from her injury and for the right breast pocket to heal with no infection before performing a capsulectomy and implant replacement. However, as previously noted, reconstruction during the initial operation may have been possible.
Summary
There are limited studies in the literature discussing the management of breast implants after gunshot wounds to the chest, so this case report serves to highlight important considerations for the treatment algorithm of patients who sustain such traumatic injuries to the chest after cosmetic augmentation mammoplasty. Additionally, as seen in this case and others, patients’ breast implants seem to alter the trajectory or prevent penetration of bullets within the thoracic cavity and, thus, may in fact save lives.
Acknowledgments
Affiliations: 1Division of Plastic, Maxillofacial, and Oral Surgery, Department of Surgery, Duke University, Durham, NC; 2Division of Plastic and Reconstructive Surgery, Department of Surgery, University of Louisville, Louisville, KY; 3University of Louisville School of Medicine, Louisville, KY
Correspondence: Milind D Kachare, MD; Milind.Kachare@gmail.com
Disclosures: The authors disclose no financial or other conflicts of interest.
References
1. Solutions JHCfGV. A year in review: 2020 gun deaths in the U.S. April 28, 2022. Accessed April 27, 2022. https://publichealth.jhu.edu/sites/default/files/2022-05/2020-gun-deaths-in-the-us-4-28-2022-b.pdf
2. Violence TEFtSG. Gun Violence in the United States. February 2021. Accessed November 27, 2022. https://efsgv.org/learn/type-of-gun-violence/gun-violence-in-the-united-states/
3. Fowler KA, Dahlberg LL, Haileyesus T, Annest JL. Firearm injuries in the United States. Prev Med. Oct 2015;79:5-14. doi:10.1016/j.ypmed.2015.06.002
4. Maher JL, Bennett DC, Bennett LL, Grothaus P, Mahabir RC. Breast augmentation: a geographical comparison. Can J Plast Surg. Winter 2010;18(4):e44-e46.
5. The American Society for Aesthetic Plastic Surgery’s Cosmetic Surgery National Data Bank: Statistics 2018. Aesthet Surg J. Jun 21 2019;39(Suppl_4):1-27. doi:10.1093/asj/sjz164
6. Rosen H, Brzezienski M, Higdon KK. Silicone breast implants can save lives. Plast Reconstr Surg Glob Open. Jun 2014;2(6):e169. doi:10.1097/GOX.0000000000000065
7. McEvenue G, Oikonomou A, Ditkofsky N, Lipa J. Life-saving silicone breast implant after firearm injury: case report and treatment recommendations. Plastic Surgery Case Studies. Jan 2020;6:2513826X1989882. doi:10.1177/2513826X19898821
8. Pramod NK, Thoma A. Breast implant rupture due to gunshot injury. Plast Reconstr Surg. Nov 1994;94(6):893-4. doi:10.1097/00006534-199411000-00035
9. Pereira LH, Sterodimas A. Rupture of high-cohesive silicone implant after gunshot injury. Ann Plast Surg. Feb 2007;58(2):228-229. doi:10.1097/01.sap.0000251489.34295.5a
10. Ashcroft J, Murphy S, Laing TA, Durrani AJ, Roshan A. A new clinical presentation: breast implant pneumocapsule and pneumothorax following penetrating chest wall trauma. Ann R Coll Surg Engl. Mar 2021;103(3):e98-e100. doi:10.1308/rcsann.2020.7038
11. Rice DC, Agasthian T, Clay RP, Deschamps C. Silicone thorax: a complication of tube thoracostomy in the presence of mammary implants. Ann Thorac Surg. Nov 1995;60(5):1417-1419. doi:10.1016/0003-4975(95)00499-B
12. Pinto A, Russo A, Reginelli A, et al. Gunshot wounds: ballistics and imaging findings. Semin Ultrasound CT MR. Feb 2019;40(1):25-35. doi:10.1053/j.sult.2018.10.018
13. Pannucci CJ, Cyr AJ, Moores NG, Young JB, Szegedi M. A ballistics examination of firearm injuries involving breast implants. J Forensic Sci. Mar 2018;63(2):571-576. doi:10.1111/1556-4029.13589