Epidermoid Cyst of Orbit Requiring Cranialization of Frontal Sinus
Questions
1. How often do intracranial epidermoid cysts occur?
2. Is a coronary incision necessary?
3. What are the steps of the procedure, difficulties encountered, and process for circumventing those difficulties?
4. What is the follow-up protocol and outcome?
Case Description
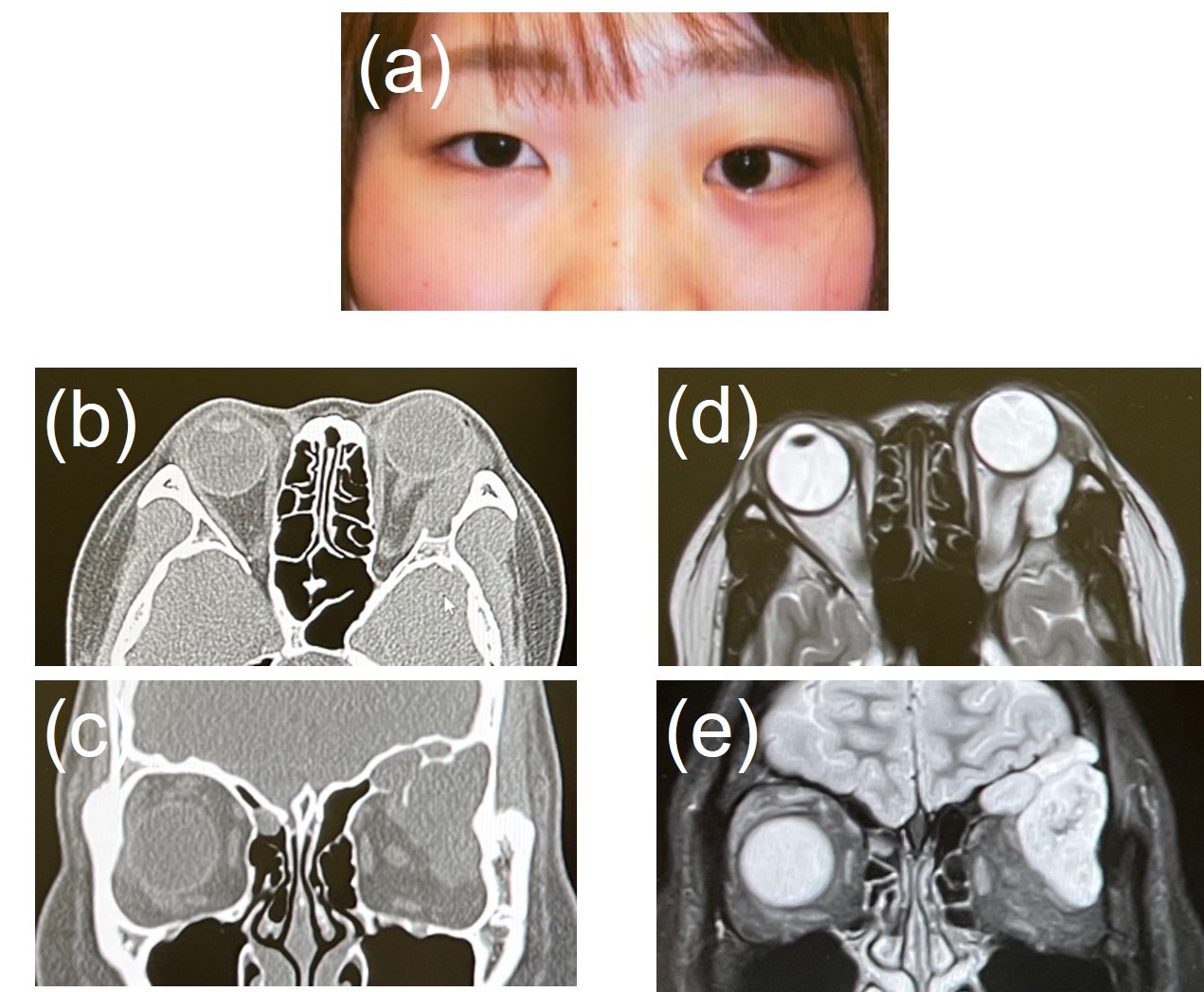
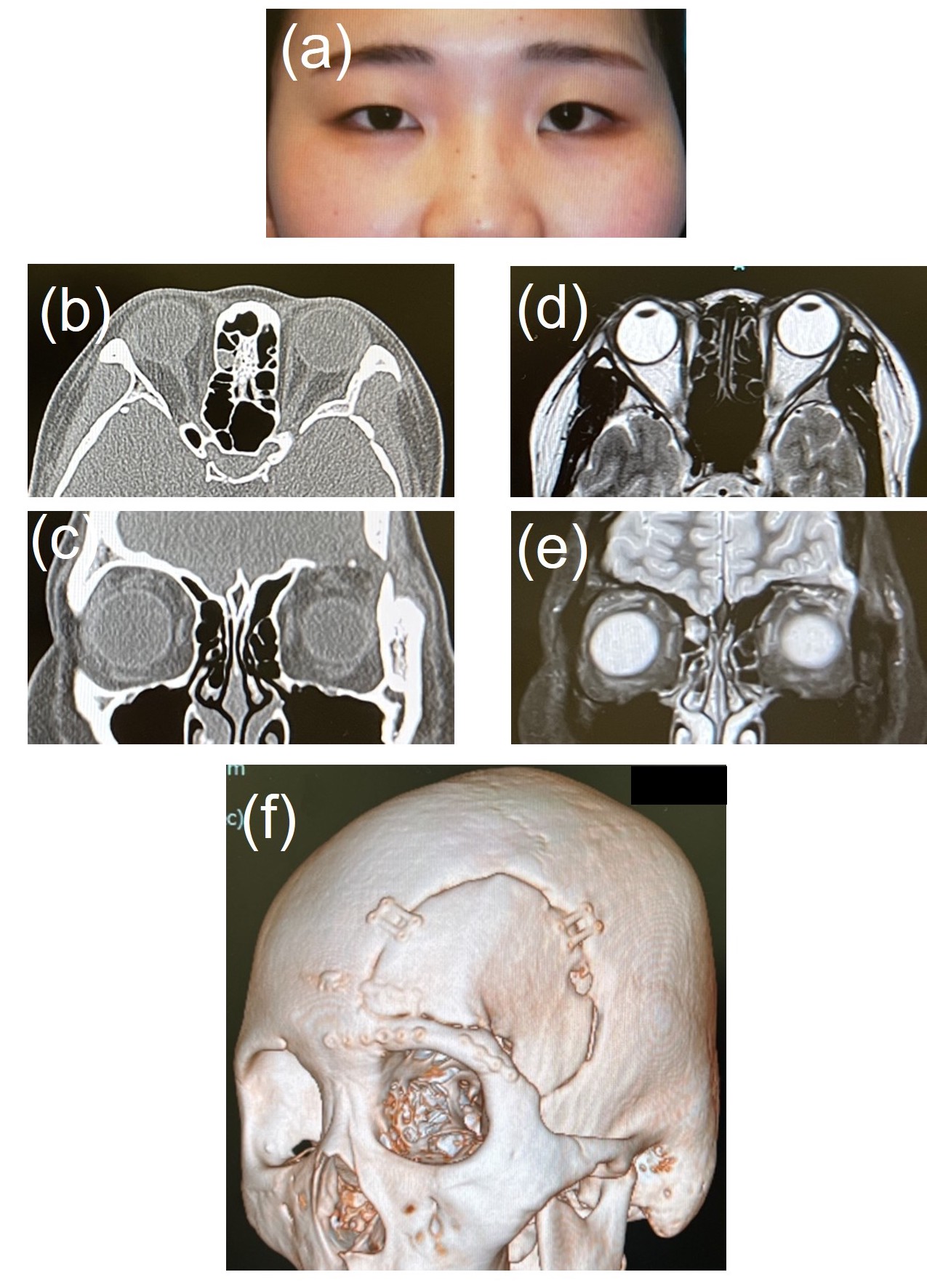
The patient was a 20-year-old female. Exophthalmos of the left eye had gradually deteriorated during a 1-year period before the consultation. At the time of consultation, diplopia on an upward gaze was noted. Visual impairment was not observed. Preoperative computed tomography (CT) revealed destruction of the left orbital bone and left frontal sinus. Furthermore, preoperative magnetic resonance imaging (MRI) suggested pleomorphic adenoma or angioma (Figure 1).
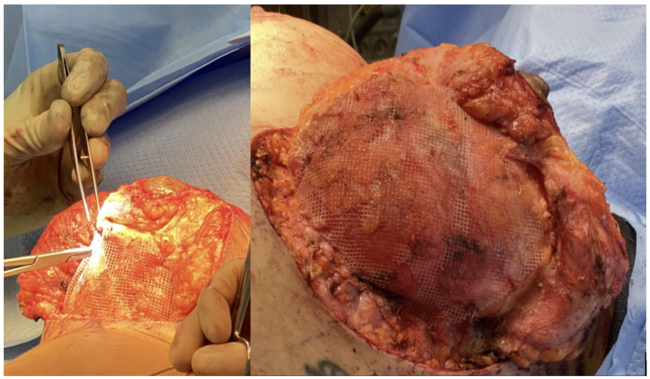
Extirpation was performed. For skin incision, a coronal incision of the head was selected. It was switched to subperiosteal exfoliation in a position 2 cm from the superior orbital margin. A scalp flap was elevated to expose the lateral orbital margin from the left superior orbital margin. Craniotomy involving the orbital margin was performed by neurosurgeons to expose the mass. The mass was exfoliated from the peripheral tissue and extirpated. In addition, the destroyed frontal sinus and its mucosa were also extirpated. While operating in the deep area of the orbit, the capsule ruptured; sufficient aspiration and curettage were conducted to remove all contents that leaked and the capsule remnants. After extirpation there was dead space at the same site. Dead space filling, that is, cranialization of the frontal sinus, was performed by elevating an anterior pericranial flap. Because the dead space was filled with the anterior pericranium flap and the dura mater was intact, the reconstruction of the orbital roof was not necessary. The bone flap was returned to the original position and fixed with an absorbable plate. Surgery was completed through surgical incision closure (Figure 2).
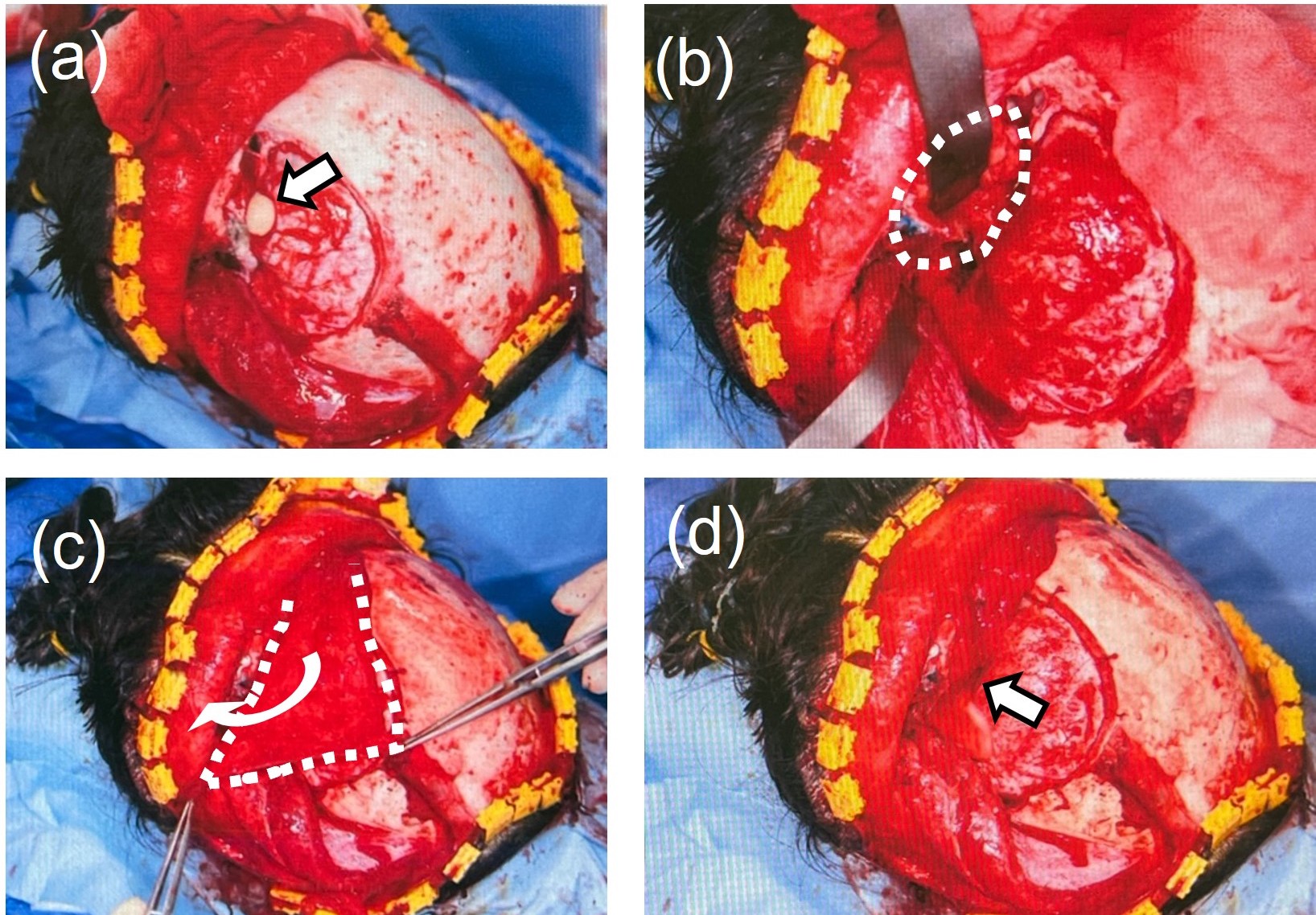
The mass involving the capsule could be completely extirpated. Pathological diagnosis suggested an epidermoid cyst. After the operation, doses of 1 g cephalosporin were given 2 times daily for 5 days. The postoperative course was favorable, and there was no complication. The patient was discharged 9 days after surgery. Exophthalmos and diplopia had reduced. There was no visual impairment. Postoperative follow-up for 18 months was possible, with no relapse during this period (Figure 3). There was no cosmetic problem.
Q1. How often do intracranial epidermoid cysts occur?
An epidermoid cyst is a benign tumor that develops through ectopic migration of epithelial cells in weeks 3 to 5 of gestation. This tumor is rare and accounts for 0.3% to 1.8% of intracranial masses.1 In addition, lesions measuring >50 mm account for 20% of intracranial epidermoid cysts.2 In the present case, the maximum diameter was 65 mm. Furthermore, patients with frontal sinus infiltration, as demonstrated in the present case, have been reported,3-5 but such cases may be extremely rare. Many epidermoid cysts are confirmed as painless nodes or swelling along the orbital margin within 1 year after birth. Most cysts are detected by parents. On the other hand, when an epidermoid cyst develops in the deep area of the orbit, painless blepharoptosis or diplopia gradually appears in young adulthood, leading to a diagnosis of this cyst.6 The patient in the present study had also consulted the hospital at the age of 19 years, and symptoms developed slowly; therefore, an epidermoid cyst may have developed in the deep area of the orbit.
Q2. Is a coronary incision necessary?
When extirpating a mass localized in the orbit, the visual field is secured using an anterior approach in the superficial layer and by combining it with orbital osteotomy in a deep area. In the present case, the mass involved the intracranial cavity through destruction of the orbital roof and frontal sinus; prior to surgery, treatment of the frontal sinus was considered as possibly being necessary, and an approach through the coronal i
Q3. What are the steps of the procedure, difficulties encountered, and process for circumventing those difficulties?
Frontotemporal craniotomy was performed, and a bone flap was removed. However, there was no skull infiltration. Also, there was no dural infiltration. However, patients with dural infiltration have been reported,7,8 and it may be necessary to prepare for dural reconstruction. A previous study indicated that epidermoid cysts in the orbit or its deep area induced changes or destruction of a larger number of bones, making complete cyst removal difficult.6 Therefore, attention was particularly required to ensure complete removal of the capsule. Because the frontal sinus had been destroyed, the frontal sinus wall and mucosa were removed. There was a dead space after mass removal. An anterior pericranial flap was elevated to the dead space, and it was filled with the flap for cranialization of the frontal sinus. If there is a possibility that a dead space may appear, as demonstrated in the present case, the forehead involving the periosteum should be elevated when exfoliating/elevating a scalp flap on coronal incision. To our knowledge, no study has reported cranialization of the frontal sinus using an anterior pericranial flap after resection of an epidermoid cyst involving the intracranial cavity.
Q4. What is the follow-up protocol and outcome?
In the present case, the capsule ruptured during surgery; fortunately, the residual capsule could be completely removed under direct vision. If cyst capsule extirpation is incomplete, the recurrence rate may be up to 30%.9 Thus, the cyst capsule must be completely extirpated. Furthermore, there is a case report in which squamous cell carcinoma developed from a capsule that remained after surgery, leading to a fatal outcome despite additional surgery and radiotherapy.10 Although epidermoid cysts are benign, they may recur through malignant alteration of the residual capsule; accurate resection is necessary. Therefore, for treatment, physicians must explain sufficient resection and reconstruction with a flap to patients. Furthermore, long-term postoperative follow-up may be important.
Summary
Resection is performed as a basic treatment in many patients with intraorbital tumors. When a tumor develops in the deep area of the orbit, it is reached using orbital bone osteotomy or transcranial approaches. When a tumor develops in the deep area of the orbit, it is reached using orbital bone osteotomy or transcranial approaches. However, when the mass involves the frontal sinus, treatment of the frontal sinus must be added. This treatment was necessary in the present case, and cranialization of the frontal sinus with an anterior pericranial flap was performed in addition to tumorectomy to reconstruct the anterior cranial base.
Acknowledgments
Affiliations: 1Department of Plastic and Reconstructive Surgery, Kindai University Faculty of Medicine, Osaka-Sayama, Japan; 2Plastic Surgery, Izumi General Hospital, Izumi, Japan; 3Department of Neurosurgery, Kindai University Faculty of Medicine, Osaka-Sayama, Japan; 4Center for Medical Education and Clinical Training, Kindai University Faculty of Medicine, Osaka, Japan; 5Nagumo Clinic Osaka, Osaka, Japan
Correspondence: Tadaaki Morotomi, MD, PhD; tadamorotomi@gmail.com
Ethics: This report was prepared in accordance with the ethical principles described in the Helsinki Declaration, which was revised in 2013. In accordance with the regulations set forth by Human Investigations Committee of the Kindai University Faculty of Medicine, informed consent was obtained from this patient and her parents.
Disclosures: The authors disclose no financial or other conflicts of interest.
References
1. Zhang F, Xu YN, Zhao W, Wang YH, He JQ. Posttraumatic giant intradiploic epidermoid cyst of orbital roof. J Craniofac Surg. 2021;32(1):e102-e103. doi:10.1097/SCS.00000000000067622.
2. Akhaddar A, Gazzaz M, El Mostarchid B, Kadiri B, Lrhezzioui J, Boucetta M. Kyste épidermoïde géant de la voûte à développement extracrânien et intracrânien. A propos d'un cas [Giant epidermoid cyst of the skull with extra and intracranial extension. A case report]. J Neuroradiol. 2002;29(3):193-199.
3. Gollapudi PR, Musali SR, Mohammed I, Pittala SR. A frontal giant intradiploic giant pearl (epidermoid cyst) with intracranial and extracranial extension: A rare entity. J Pediatr Neurosci. 2018;13(4):480-482. doi:10.4103/JPN.JPN_74_18
4. Wax MK, Briant TD. Epidermoid cysts of the cranial bones. Head Neck. 1992;14(4):293-296. doi:10.1002/hed.2880140407
5. Sauaia Filho EN, Grangeiro Barreto E, Macêdo Filho LJM, et al. Intradiploic epidermoid cyst in frontal sinus causing diplopia: Case report and literature reviewInterdiscip. Neurosurg: Adv Tech Case Manag. 2020;20:100669. doi:10.1016/j.inat.2020.100669
6. Pushker N, Meel R, Kumar A, Kashyap S, Sen S, Bajaj MS. Orbital and periorbital dermoid/epidermoid cyst: a series of 280 cases and a brief review. Can J Ophthalmol. 2020;55(2):167-171. doi:10.1016/j.jcjo.2019.08.005
7. Cho JH, Jung TY, Kim IY, Jung S, Kang SS, Kim SH. A giant intradiploic epidermoid cyst with perforation of the dura and brain parenchymal involvement. Clin Neurol Neurosurg. 2007;109(4):368-373. doi:10.1016/j.clineuro.2006.12.011
8. Hasturk AE, Basmaci M, Yilmaz ER, Kertmen H, Gurer B, Atilgan AO. Giant intradiploic epidermoid cyst presenting as solitary skull mass with intracranial extension. J Craniofac Surg. 2013;24(6):2169-2171. doi:10.1097/SCS.0b013e3182a2d820
9. Gharabaghi A, Koerbel A, Samii A, Safavi-Abbasi S, Tatagiba M, Samii M. Epidermoid cysts of the cavernous sinus. Surg Neurol. 2005;64(5):428-433. doi:10.1016/j.surneu.2005.02.011
10. Bretschneider T, Dorenbeck U, Strotzer M, Roth M, Rümmele P, Buettner R. Squamous cell carcinoma arising in an intradiploic epidermoid cyst. Neuroradiology. 1999;41(8):570-572. doi:10.1007/s002340050807