Video file
Original Research
Comparing the Results of External Rotational Humeral Osteotomy in Older Children to the Mod Quad and Triangle Tilt Procedures in Adults with Obstetric Brachial Plexus Injury
February 2022
1937-5719
ePlasty 2022;22:e2
Abstract
Background. External Rotational Humeral osteotomy is used to address the external rotation deficit in older children with obstetric brachial plexus Injury (OBPI). Although this procedure improves the cosmetic effect of shoulder subluxation, it has no effect on the underlying structural (glenohumeral deformity and scapular elevation and rotation) and functional problems. In this study, improvements in glenohumeral joint alignment; scapular hypoplasia, elevation, and rotation (SHEAR) deformity; and upper extremity functional movements were demonstrated in adult patients with OBPI 1 year after the mod Quad and/or triangle tilt surgeries.
Methods and Materials. The outcome of humeral rotational osteotomy reported in the literature was compared with the results from 43 adult patients with OBPI (21 men and 22 women; 23 right and 20 left sides) with a mean age of 21.3 years ( range, 17 to 38 years) who underwent mod Quad and/or triangle tilt surgeries and had over 12 months of postoperative follow-up (mean 22.9 months; range, 12 to 50 months).
Results. The preoperative average modified total Mallet score, including supination, was 14.6 ± 3.5 (P < 0.0001) in the 43 adult patients with OBPI in this report. This total Mallet score was significantly improved to 22 ± 3.9 (P < 0.0001) over 12 months after mod Quad and/or triangle tilt surgeries. Thirty-two (75%) of the patients showed great improvement in all upper extremity functions: shoulder abduction, external rotation, hand-to-mouth, hand-to-neck, hand-to-spine, and supination. The improvement after humeral osteotomy reported in the literature was a cosmetic effect that did not address the underlying structural and functional problems and was found to decrease the improved shoulder abduction in long-term follow-up.
Conclusions. Thirty-two (75%) of 43 adult patients with OBPI showed great improvement in all upper extremity functions 1 year after mod Quad and/or triangle tilt surgeries. The other 11 patients (25%) showed improvement in hand-to-mouth movement and/or supination. In contrast, humeral osteotomy, as reported in the literature, improved the cosmetic effect of shoulder subluxation but had no effect on the underlying structural and functional problems.
Introduction
The occurrence of obstetric brachial plexus injury (OBPI) varies from 0.9 to 5.8 per 1000 live births.1-3 The associated risk factors can be maternal and pregnancy-related (obesity, maternal diabetes, cephalopelvic disproportion, small maternal stature, primiparity), fetal (macrosomia, macrocephaly, extreme prematurity with low birth weight, congenital anomalies), or delivery/birth-related (shoulder dystocia, prolonged or rapid labor, vaginal delivery assisted by forceps or vacuum extractions, oligohydramnios and malpresentation, including breech presentation).4-7
The brachial plexus nerve roots, C5 to C6, are most frequently stretched in a newborn with OBPI and may restore function spontaneously.2,8 Some infants with OBPI can have medial nerve damage and continue to demonstrate loss of upper extremity function or have damage to many, if not all, nerve roots (C5 to T1), ranging from neuropraxia to severe cases such as rupture or avulsion.9 Children who do not recover fully within the first 3 months are likely to develop secondary deformities, especially at the shoulder, with the most common at that site being the lack of abduction and external rotation.10 These children demonstrate a lack of external rotation and the persistence of internal rotation due to the weakness of external rotators (teres minor and infraspinatus) compared to the internal rotators (teres major, pectoralis major, and latissimus dorsi). They develop secondary bone changes in the glenoid that includes glenohumeral dysplasia, posterior dislocation, or subluxation of the humeral head, resulting in substantial loss of upper extremity functional movements.11-15
The shoulder internal rotation deformity is treated surgically either by soft tissue release or by bony osteotomy. Traditionally, the external rotation humeral osteotomy (ERHO) is performed on older children with dislocated shoulders.16-25 These osteotomy results have been shown to be satisfactory with the improvement of external rotation, and some loss of internal rotation (manifested by the child’s inability to reach their abdomen with their hand). ERHO improves the cosmetic effect of shoulder subluxation while having no effect on the underlying structural (glenohumeral deformity, and scapular elevation and rotation) and functional problems. Moreover, ERHO has been performed on patients with OBPI up to only 17 years of age.15-25 The authors have previously demonstrated that the mod Quad procedure may improve upper extremity functions, including shoulder abduction, in adult patients with OBPI.26
Untreated adult patients with this injury, in general, use compensatory strategies to achieve their lost upper extremity functions, which may cause adverse effects. Results from the present study show improved upper extremity functional movements in 43 adult patients who underwent mod Quad and/or triangle tilt surgeries and had over 12 months of postoperative follow-up evaluation.27,28
Methods and Materials
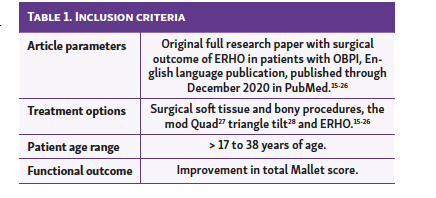
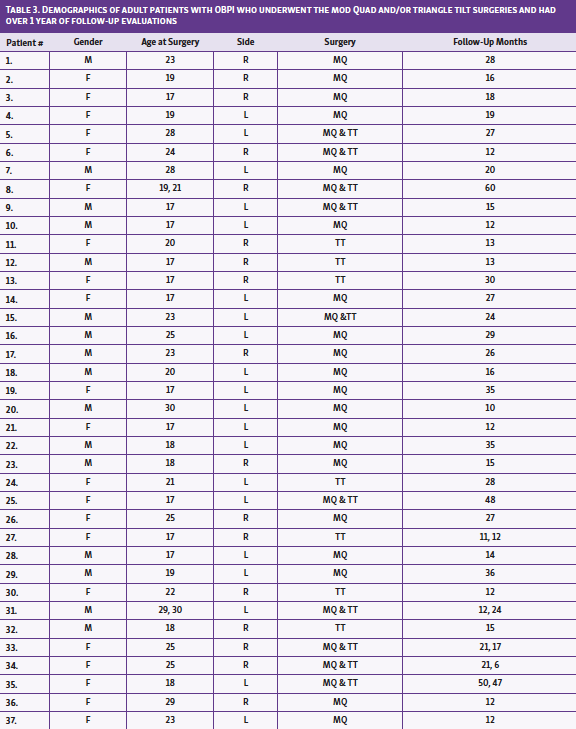
A retrospective chart review was conducted based on the institution's surgical cases. Inclusion criteria were patients with OBPI over 17 years of age who showed decreased or loss of upper-extremity functional movements with median rotation contracture (MRC) and SHEAR deformity preoperatively and who underwent the modified Quad and/or triangle tilt surgeries.28 Forty-three such patients (21 men and 22 women; 23 right sides and 20 left sides) with a mean age of 21.3 years (range, 17 to 38 years) that met these criteria were identified with a mean follow-up time of 22.9 months (range, 12 to 50 months). Of 43 adult patients with OBPI in this report, 33 had the mod Quad surgery, 14 had triangle tilt, and 10 had both surgeries. All surgical procedures were performed by the lead author (RKN).
Mod Quad Procedure
The modified Quad is a modification of the combination of muscles released and their insert positions to improve upon a previously described operation.27 Thirty-five adult patients with OBPI underwent latissimus dorsi and teres major muscle transfer; subscapularis, pectoralis major and minor contracture releases; axillary nerve decompression; and neurolysis. Transferred muscles were sutured to the teres minor muscle, not to a bony insertion point.
Triangle Tilt Procedure
The triangle tilt surgery consisted of osteotomy of the clavicle at the junction of the middle and distal thirds; osteotomy of the acromion process at its junction with the scapula's spine; osteotomy of the superomedial angle of the scapula; and splinting of the extremity in adduction, external rotation, and forearm supination. Minor elements of the procedure included bone grafting of the acromion process osteotomy site and semirigid fixation of the clavicular osteotomy segments to prevent nonunion.
Clinical Evaluation of Patients by Mallet Grading
Patients were evaluated through video recordings using a modified Mallet scale.25 Depending on their ability to perform shoulder and arm movements (shoulder abduction, external rotation, hand-to-mouth, hand-to-neck, hand-to-spine, and supination), patients were scored on a scale of 1 to 5, with 1 being most affected and 5 being normal. The overall Mallet score (6 to 30) was calculated based on these 6 movements. In addition to the modified Mallet functional movements, the angle of apparent supination (the angle between the midline of the body and the tangential line to the palm with arms straight) was also recorded and measured for each patient to more precisely define the functional disability (neutral = 0 [2], full supination = 90° [5], supination = 30° to 60° [4], supination = 0 to 30° [3], full pronation = −90° [1]).
Statistical Analysis
Paired student's t-tests were conducted using Excel 2003 (Microsoft) with the Analyze-It plug-in to determine if differences between preoperative and postoperative shoulder abduction and somatosensory evoked potentials for each function were statistically significant. The P values were two-tailed and considered significant if less than or equal to 0.05.
Results
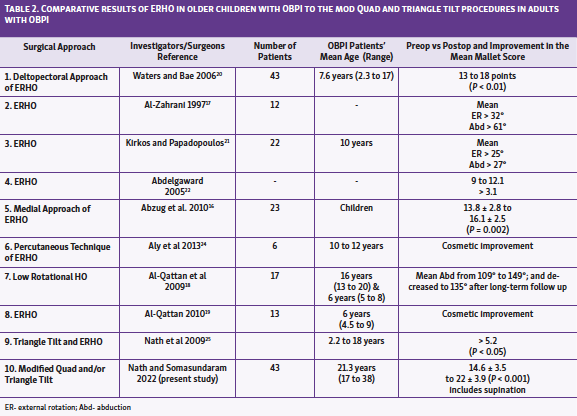
Eight studies on ERHO that addressed the internal rotation contracture (IRC) in older children with OBPI who lacked external rotation were included (Table 1, Table 2), and these were compared to the procedures conducted in the 43 adult patients with OBPI (Table 2, Table 3, Table 4) in this report. None of the studies on ERHO reported all Mallet functional outcomes as ERHO mainly addresses the external rotation in older children.16-24 However, 2 studies reported the ERHO outcome of 3 modified Mallet functions (hand-to-mouth, hand-to-neck, and external rotation motions) in children aged between 2.3 and 17 years; mean age, 7.6 years.16,20 Two other studies reported that the patients' external rotation improved to mean 25° and 32°.17,21 However, the patients' average abduction angle remained limited to 27° and 61°, respectively. Al-Qattan 201019 and Aly et al24 showed a cosmetic improvement, while their patients' shoulder abduction decreased after long-term follow-up.
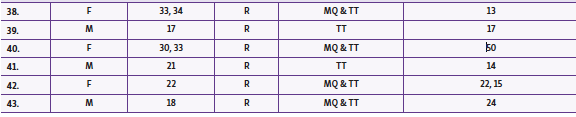
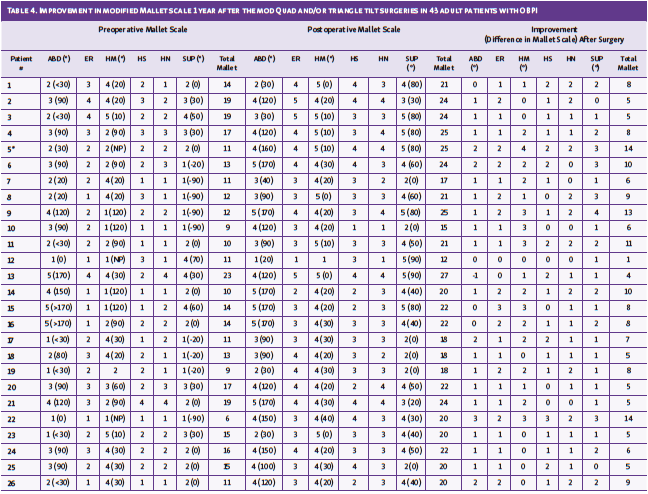
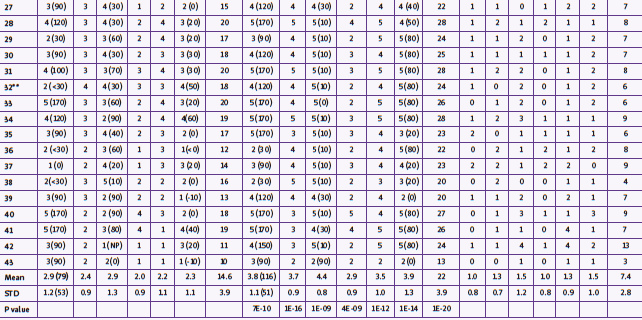
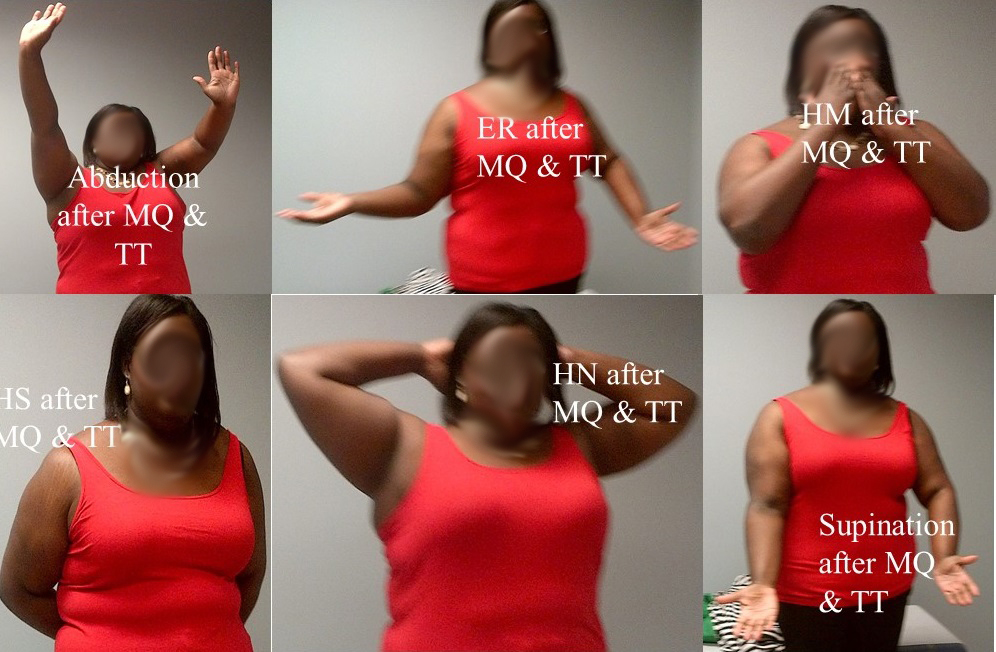
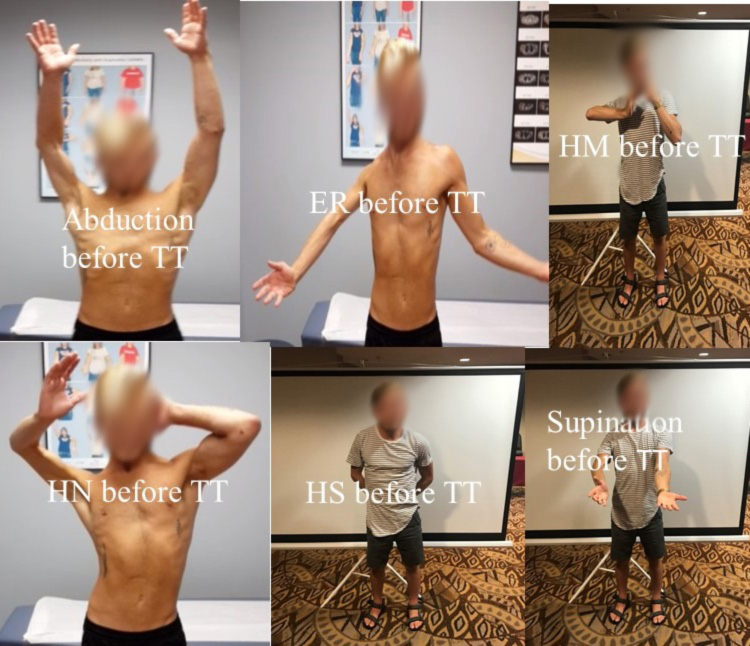
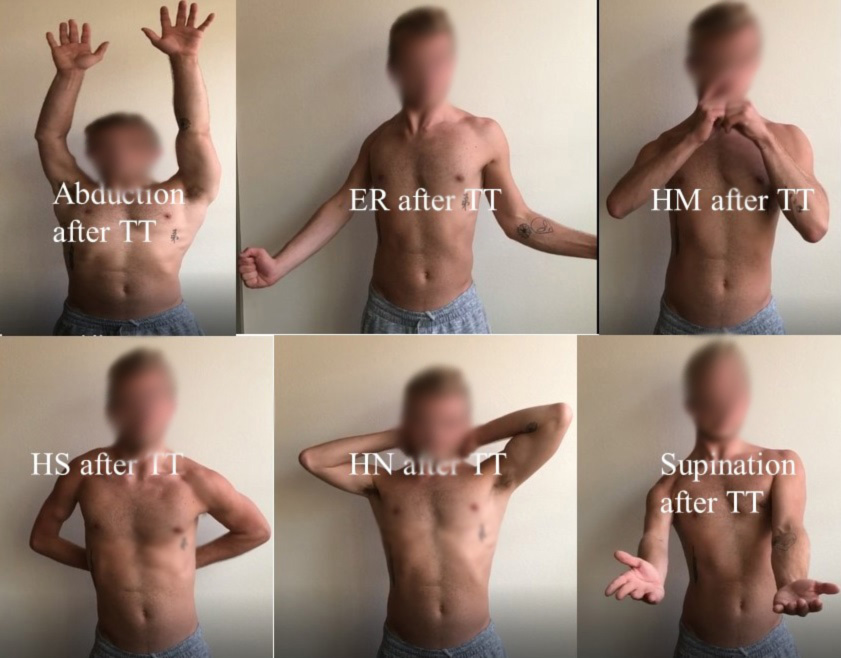
The outcome of all upper extremity functions (shoulder abduction, external rotation, hand-to-mouth, hand-to-neck, hand-to-spine, and supination) were reported in the 43 adults with OBPI included in this study. Preoperative average modified total Mallet score, including supination, was 14.6 ± 3.5. This total Mallet score significantly improved to mean 22 ± 3.9 (P < 0.0001) over 12 months after the mod Quad and/or triangle tilt procedures. Active shoulder abduction improved to a mean of 116° ± 51 (range, 20° to 170°) postoperatively from the preoperative mean of 79° ± 53 (range, 0° to 170°). Most (75%) of these adult patients showed great improvement in all upper extremity functions. There were significant improvements after surgery in the Mallet scores for shoulder abduction (2.9 ± 12. vs 3.8 ± 1.1, P < 0.0001), external rotation (2.4 ± 0.9 vs 3.7 ± 0.9, P < 0.0001), hand-to-mouth (2.9 ± 1.3 vs 4.4 ± 0.8, P < 0.0001), hand-to-spine (2.0 ± 0.9 vs 3.1 ± 0.1, P < 0.0001), hand-to-neck (2.2 ± 0.1 vs 3.9 ± 1.1, P < 0.0001), and apparent supination (2.3 ± 1.1 vs 3.9 ± 0.1, P < 0.0001; angle (–10° ± 5° vs 35° ± 15°, P < 0.0001) (Table 4 and Figure 1; Figure 2, Figure 3, Figure 4; online Video 1, online Video 2).

The mean angle for hand-to-mouth was not calculated since patients (indicated * and ** in Table 4 and Figure 5) could lift their arms up to 0 to 30° but were unable to reach their hand to mouth. However, some patients could fully abduct their arms greater than 120°, but were unable to touch their mouth. Mallet score for hand-to-mouth is calculated as hand-to-mouth angle 0 to 30° = score 5; greater than 30° to 60° = 4; greater than 60° to 90° = 3; greater than 90° = 2 and not possible (NP) = 1.

Discussion
Humeral osteotomy is traditionally used to address the external rotation deficit (ERHO in older children) in children with OBPI. This procedure, however, improves the cosmetic effect of shoulder subluxation while having no effect on the underlying structural (glenohumeral deformity and scapular elevation and rotation) and functional problems.18,19,24 Further, shoulder abduction remains limited, and the abduction range further reduced over a period of time.18,19 Moreover, frequent complications are reported for humeral osteotomy such as keloid scar, loss of external rotation secondary to bone remodeling, loss of internal rotation, prominence of osteosynthesis, distal fracture plate transient ulnar paresthesia, radial nerve palsy, and delayed union and nonunion.29
Children who have the severe limitation of passive external rotation (less than neutral) develop SHEAR deformity. The elevated scapula causes the anterior tilting of the acromioclavicular triangle, which hampers the external rotation, increases the internal rotation, and facilitates posterior subluxation of the humeral head. The triangle tilt surgery specifically addresses the scapular deformity and solves the impingement of the anteriorly tilted distal acromioclavicular triangle against the humeral head by releasing it from the medial spine of the scapula, and the abnormal twisting of the clavicle by releasing the medial clavicle through osteotomy of the clavicle. This allows the distal triangle to tilt back to its neutral position, reducing the scapula's abnormal elevation and rotation, therefore, realigning the glenohumeral joint properly. This supports the humeral head to rotate externally. The authors have previously shown excellent functional outcomes of triangle tilt in a series of 79 children with OBPI.30
As demonstrated in this study, the triangle tilt and mod Quad surgeries were successfully performed on 43 adult patients with OBPI. Thirty-two (75%) of these patients showed great improvement in all upper extremity functions 1 year after the mod Quad and/or triangle tilt surgeries. The other 11 patients (25%) showed improvement in hand-to-mouth movement and/or supination.Two patients showed a minimum improvement in total Mallet scores of 1 and 3. One patient showed improvement only in supination, and the other showed improvement both in supination and hand-to-mouth movement. Overall, hand-to-mouth (mean Mallet score > 4.4 out of 5) and supination (mean Mallet score > 3.9 out of 5) were improved more significantly, following shoulder abduction (mean Mallet score > 3.8 out of 5), external rotation (mean Mallet score > 3.7 out of 5), hand-to-neck (mean Mallet score > 3.5 out of 5) and hand-to-spine (mean Mallet score > 2.9 out of 5) movements.
Conclusions
Thirty-two (75%) of adult OBPI patients in this study showed great improvement in all upper extremity functions 1 year after the mod Quad and/or triangle tilt surgeries. The other 11 patients (25%) showed improvement in hand-to-mouth movement and/or supination. In contrast, although humeral osteotomy may improve the cosmetic effect of shoulder subluxation, it does not address the underlying structural and functional problems.
Videos
Video file
Acknowledgments
Affiliations: Texas Nerve and Paralysis Institute, Houston, Texas
Correspondence: Rahul Nath, MD, Texas Nerve and Paralysis Institute, 6400 Fannnin St, Ste 2290, Houston, Texas 77030; drnath@drnathmedical.com
Disclosures: The authors disclose no financial or other conflicts of interest.
References
1. Foad SL, Mehlman CT, Ying J. The epidemiology of neonatal brachial plexus palsy in the United States. J Bone Joint Surg Am. 2008;90(6):1258–1264. doi: 10.2106/JBJS.G.00853
2. Adler JB, Patterson RL Jr. Erb’s palsy. Long-term results of treatment in eighty-eight cases. J Bone Joint Surg Am. 1967;49(6):1052–1064.
3. Gurewitsch ED, Johnson E, Hamzehzadeh S, Allen RH. Risk factors for brachial plexus injury with and without shoulder dystocia. Am J Obstet Gynecol. 2006;194(2):486–492. doi: 10.1016/j.ajog.2005.07.071
4. Moczygemba CK, Paramsothy P, Meikle S, et al. Route of delivery and neonatal birth trauma. Am J Obstet Gynecol. 2010;202(4):361.e1-361.e6. doi: 10.1016/j.ajog.2009.11.041
5. Werner EF, Janevic TM, Illuzzi J, et al. Mode of delivery in nulliparous women and neonatal intracranial injury. Obstet Gynecol. 2011;118(6):1239-1246. doi: 10.1097/AOG.0b013e31823835d3
6. Vitner D, Hiersch L, Ashwal E, et al. Outcomes of vacuum-assisted vaginal deliveries of mothers with gestational diabetes mellitus. J Matern Fetal Neonatal Med. 2019;32(21):3595-3599. doi: 10.1080/14767058.2018.1468880
7. Dumpa V, Kamity R. Birth Trauma. [Updated 2020 Sep 9]. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2020 Jan. Available from: https://www.ncbi.nlm.nih.gov/books/NBK539831/
8. Sever JW. Obstetrical paralysis. Report of eleven hundred cases. JAMA. 1925;85(24):1862-1865.
9. Sunderland, S. A classification of peripheral nerve injuries producing loss of function. Brain. 1951;74(4):491-516. doi: 10.1093/brain/74.4.491
10. Troum S, Floyd WE 3rd, Waters PM. Posterior dislocation of the humeral head in infancy associated with obstetrical paralysis. A case report. J Bone Joint Surg Am. 1993;75(9):1370-1375. doi: 10.2106/00004623-199309000-00013
11. Beischer AD, Simmons TD, Torode IP. Glenoid version in children with obstetric brachial plexus palsy. J Pediatr Orthop. 1999;19(3):359-361.
12. Birch R, Ahad N, Kono H, Smith S. Repair of obstetric brachial plexus palsy: results in 100 children. J Bone Joint Surg Br. 2005;87(8):1089-1095. doi: 10.1302/0301-620X.87B8.15975
13. Kambhampati SB, Birch R, Cobiella C, Chen L. Posterior subluxation and dislocation of the shoulder in obstetric brachial plexus palsy. J Bone Joint Surg Br. 2006;88(2):213-219. doi: 10.1302/0301-620X.88B2.17185
14. Moukoko D, Ezaki M, Wilkes D, Carter P. Posterior shoulder dislocation in infants with neonatal brachial plexus palsy. J Bone Joint Surg Am. 2004;86(4):787-793. doi: 10.2106/00004623-200404000-00018
15. Abdelgawad A, Naga O. Birth Injuries and Orthopedic Manifestations in Newborns. In: Abdelgawad A, Naga O, eds. Pediatric Orthopedics: A Handbook for primary care physicians.14th ed. Springer; 2014:75–83.
16. Abzug JM, Chafetz RS, Gaughan JP, Ashworth S, Kozin SH. Shoulder function after medial approach and derotational humeral osteotomy in patients with brachial plexus birth palsy. J Pediatr Orthop. 2010;30(5):469–474. doi: 10.1097/BPO.0b013e3181df8604
17. Al-Zahrani S. Combined Sever’s release of the shoulder and osteotomy of the humerus for Erb’s palsy. J Hand Surg Br. 1997;22(5):591–593. doi: 10.1016/s0266-7681(97)80352-x
18. Al-Qattan MM, Al-Husainan H, Al-Otaibi A, El-Sharkawy MS. Long-term results of low rotation humeral osteotomy in children with Erb's obstetric brachial plexus palsy. J Hand Surg Eur Vol. 2009;34(4):486–492. doi: 10.1177/1753193409104552
19. Al-Qattan MM. Total obstetric brachial plexus palsy in children with internal rotation contracture of the shoulder, flexion contracture of the elbow, and poor hand function: improving the cosmetic appearance of the limb with rotation osteotomy of the humerus. Ann Plast Surg. 2010;65(1):38–42. doi: 10.1097/SAP.0b013e3181a72f9e
20. Waters PM, Bae DS. The effect of derotational humeral osteotomy on global shoulder function in brachial plexus birth palsy. J Bone Joint Surg Am. 2006;88(5):1035–1042. doi: 10.2106/JBJS.E.00680
21. Kirkos JM, Papadopoulos IA. Late treatment of brachial plexus palsy secondary to birth injuries: rotational osteotomy of the proximal part of the humerus. J Bone Joint Surg Am. 1998;80(10):1477–1483. doi: 10.2106/00004623-199810000-00009
22. Abdelgawad A. Shoulder deformity in children with Erb’s palsy. Dissertation. Ain Shams University; 2005.
23. Abdelgawad AA, Pirela-Cruz MA. Humeral rotational osteotomy for shoulder deformity in obstetric brachial plexus palsy: which direction should I rotate? Open Orthop J. 2014;8:130-134. doi: 10.2174/1874325001408010130
24. Aly A, Bahm J, Schuind F. Percutaneous humeral derotational osteotomy in obstetrical brachial plexus palsy: a new technique. J Hand Surg Eur Vol. 2014;39(5):549–552. doi: 10.1177/1753193413492058
25. Nath RK, Somasundaram C, Melcher SE, Bala M, Wentz MJ. Arm rotated medially with supination - the ARMS variant: description of its surgical correction. BMC Musculoskelet Disord. 2009;10:32. doi: 10.1186/1471-2474-10-32
26. Nath RK, Goel D, Somasundaram C. Clinical and functional outcome of modified Quad surgery in adult obstetric brachial plexus injury patients: Case reports. Clin Pract. 2019;9(3):1140. doi: 10.4081/cp.2019.1140
27. Nath RK, Paizi M. Improvement in abduction of the shoulder after reconstructive soft-tissue procedures in obstetric brachial plexus palsy. J Bone Joint Surg Br. 2007;89(5):620-626. doi: 10.1302/0301-620X.89B5.18403
28. Nath RK, Lyons AB, Melcher SE, Paizi M. Surgical correction of the medial rotation contracture in obstetric brachial plexus palsy. J Bone Joint Surg Br. 2007;89(12):1638-1644. doi: 10.1302/0301-620X.89B12.18757
29. Ivalde FC, Marazita-Valverde J, Bataglia D. Early Complication of Humeral Derotational Osteotomy Surgery for Obstetric Brachial Plexus as Salvage for a Failed Tendon Transfer. Case Report. Maedica (Bucur). 2019;14(4):418-421. doi: 10.26574/maedica.2019.14.4.418
30. Nath RK, Amrani A, Melcher SE, Wentz MJ, Paizi M. Surgical normalization of the shoulder joint in obstetric brachial plexus injury. Ann Plast Surg. 2010;65(4):411-417. doi: 10.1097/SAP.0b013e3181e1335b