Surgical and Patient Reported Outcomes After DIEP Breast Reconstruction at a Low-Volume Community Hospital Without Microvascular Fellowship Training
Abstract
Background. Microsurgical breast reconstruction is typically performed at large, academic centers by fellowship-trained surgeons. This study examines surgical and patient-reported outcomes (PROs) after deep inferior epigastric perforator (DIEP) flap breast reconstruction at a community hospital by surgeons without fellowship training.
Methods. A prospective clinical database and BREAST-Q results were obtained from 33 patients after 45 DIEP flaps performed between 2016 and 2020. PROs and complications were compared to normative data and multi-institutional series. Regression analysis of patient and surgical factors with BREAST-Q scores was performed.
Results. Thirty-one patients completed BREAST-Q (response rate = 94%). Overall flap survival was 97.8%. Complications were not statistically different from larger published series (P > 0.05). Patients reported excellent outcomes after breast reconstruction: satisfaction with breasts (80.6 ± 4.3), satisfaction with outcome (88.3 ±17.7), psychosocial well-being (80.74 ± 17.4), sexual well-being (68.2 ± 24.1), physical well-being – chest (73.8 ± 16.1), and physical well-being – abdomen (73.3 ± 17.4). PROs were not statistically different from published multicenter data with the exception of superior scores in sexual well-being (P < 0.05) and breast satisfaction (P < 0.0001). Satisfaction with outcome varied by patient age and was 20.7 points higher for patients over 55 compared to patients 46 to 55 years of age (P < 0.05). Satisfaction with breasts was 29 points lower after total flap loss (P < 0.005). Psychosocial well-being scores were 26.98 points lower after a takeback (P < 0.05). Sexual well-being and physical well-being – chest scores were negatively related to increasing body mass index (BMI) (P < 0.05).
Conclusion. DIEP flap breast reconstruction can be performed with high quality and excellent PROs at a community hospital by surgeons without microvascular fellowship training.
Introduction
The goal of breast reconstruction is to restore an aesthetically pleasing breast mound that improves the patient’s psychosocial, physical, and sexual well-being.1 To critically assess outcomes after breast reconstruction, physicians must quantify the patient’s experience in addition to analyzing technical results and tabulating complications. Several surveys have been created to assess patient reported outcomes (PROs) after breast reconstruction, including more generalized tools such as the Patient Reported Outcomes Measurement Information System (PROMIS-29), and procedure- and disease-specific tools such as BREAST-Q. Use of these surveys has demonstrated long-term satisfaction with all methods of breast reconstruction, but more so with autologous reconstruction.2
DIEP flaps are the gold standard for microsurgical breast reconstruction. Numerous publications reveal consistent results with excellent patient satisfaction and quality of life, surpassing that of implant-based breast reconstruction.2–6 According to the 2019 American Society of Plastic Surgeons (ASPS) National Clearinghouse of Plastic Surgery Procedural Statistics, 107 238 breast reconstructions were performed in the United States; however, less than 10% were performed using DIEP flaps. Multiple barriers to microsurgical breast reconstruction have been suggested, including low financial reimbursement, lengthy operative times, expensive infrastructure, and need for microsurgical training.7,8 As a consequence, availability of DIEP flap breast reconstruction is limited, with approximately 87% of these surgeries performed at large, urban teaching hospitals.9
Barriers to microsurgical breast reconstruction have been analyzed. Studies examining the learning curve associated with microsurgical breast reconstruction,10,11 the impact of fellowship training,12 and the effect of community vs university setting13–15 have demonstrated favorable surgical outcomes. However, these reports have focused on operative results rather than PROs. In addition, these publications examined fellowship-trained microsurgeons at a community hospital or surgeons without fellowship training at academic centers. The authors sought to examine both surgical results and PROs of abdominally-based microvascular breast reconstruction performed by non fellowship-trained surgeons at a low-volume, community hospital.
Methods
Between December 2016 and August 2020, 45 DIEP flap breast reconstructions were performed on 33 patients (21 unilateral, 12 bilateral) at the Kaiser Permanente Moanalua Medical Center, Honolulu, Hawaii. This is an acute care hospital with 295 beds, which is not affiliated with a plastic surgery residency program. The authors are board-certified in plastic surgery, but none have microsurgical fellowship training. The senior author (KKK) completed plastic surgery residency in June 2016 and logged approximately 75 DIEP flaps during training. The assistant surgeon (SMN) was in practice 10 years and performed 10 DIEP flaps during training. The assistant surgeon (PDF) was in practice 21 years and never performed a DIEP flap; however, he had experience with microvascular head and neck reconstruction.
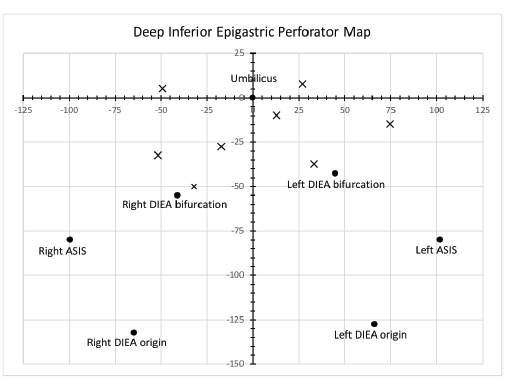
All patients underwent consultation through a multidisciplinary breast cancer clinic and underwent preoperative computed tomography angiogram (CTA) imaging of the abdomen and pelvis. Patients with cardiac disease, BMI greater than 40, active smokers, those with poorly controlled diabetes (hemoglobin A1c > 7), metastatic or stage IV breast cancer, or inadequate perforators (single, < 1.5 mm) were not offered DIEP flap reconstruction. Candidate perforator mapping was performed using Excel (Microsoft Corporation) (Figure 1) and confirmed with a hand-held doppler. The 3 authors performed simultaneous flap harvest and recipient vessel exposure. Intraoperative perfusion assessment with indocyanine green was used selectively. Postoperative monitoring was performed with venous flow-coupler doppler (GEM, Synovis Micro Companies Alliance), hand-held doppler, and clinical assessment. Patients stayed in the intensive care unit for 1 to 2 days, postoperative hourly flap checks were performed, and then patients were transferred to medical-surgical beds with flap checks performed every 4 hours. Postoperative pain was managed with acetaminophen, ibuprofen, muscle relaxants, and narcotics. All patients were assessed by a physical therapist prior to discharge.
Three months after initial reconstruction, all patients underwent revisions to address donor site standing cone deformities, scar revisions, contralateral balancing procedures, nipple reconstruction, or autologous fat grafting. BREAST-Q was obtained from each patient during a postoperative visit after final revisions. Results were compared to normative data obtained from Mundy et al16, Klifto et al,17 and one-year outcomes published by the Mastectomy Reconstruction Outcomes Consortium (MROC).18 Statistical analysis was performed using SAS 9.4 (SAS Institute). Complication rates were compared using chi-square and Fisher’s exact tests. BREAST-Q scores were compared using t-tests. To assess the relationship of patient and surgical factors with BREAST-Q scores, the authors first conducted simple linear regression for each factor separately with each individual score. Statistically significant factors (P < 0.05) were then included in the multiple linear regression models. For patients with bilateral reconstruction, the laterality for breast-specific characteristics in the regression models were randomly selected. In addition, the authors did not adjust for multiplicity in the regression analysis; therefore P-values should be interpreted with caution.
Results
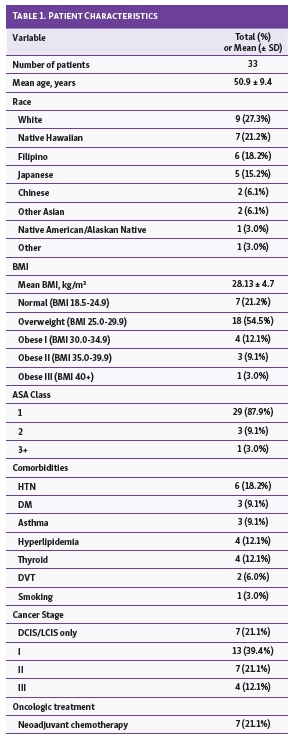
Forty-five DIEP flaps were performed in 33 patients (21 unilateral, 12 bilateral). Response rate for the BREAST-Q BR module was 94% (31 patients). Two patients with uncomplicated, unilateral breast reconstructions were lost to follow up due to change of insurance. Patient age (mean ± standard deviation) was 50.9 ± 9.4 years. The majority were of Native Hawaiian or Asian descent (72.7%). Average BMI was 28.13 ± 4.7 kg/m2. Almost all patients (96.9%) were American Society of Anesthesiologists (ASA) class 2 or less. Eleven patients (33.3%) had prior radiation therapy and 7 patients (21.1%) underwent neoadjuvant chemotherapy. Mean time from the conclusion of radiation therapy to DIEP flap breast reconstruction was 51.6 months (range 10 to 168 months). Preoperative breast data is outlined in Table 1. Two-thirds (22 patients, 66.7%) had prior abdominal surgery: 10 patients (30.3%) had a Cesarean section and 11 patients (33.3%) had laparoscopic procedures.
Surgical details are summarized in Table 2. Twenty-five (55.6%) mastectomies were skin-sparing, 17 (37.8%) were modified radical mastectomies and 3 (6.7%) were nipple-sparing mastectomies. Of the mastectomies performed, 13 (28.9%) were prophylactic, and 12 (36.4%) were bilateral. Timing of breast reconstruction was as follows: immediate (14 breasts, 42.4%); delayed (15 breasts, 45.5%), and delayed-immediate or conversion from implant-based reconstruction (4 breasts, 21.1%; 2 with expanders, 2 with implants).
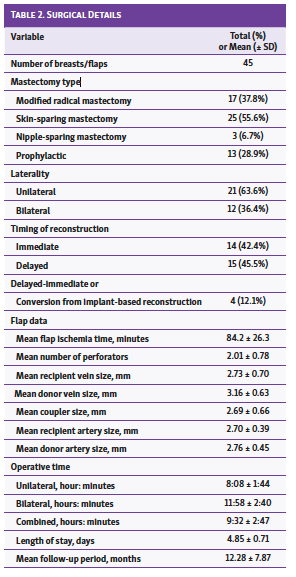
Average operative times for unilateral and bilateral reconstruction were 8:08 hours ± 1:44 and 11:58 ± 2:40, respectively. A learning curve was demonstrated with reductions in operative time: 11:12 for the first unilateral, and 5:48 for the fastest; 19:46 for the first bilateral, and 9:37 for the fastest. (Figure 2) Average ischemia time was 84 ± 26.3 minutes (range 51 to 166 minutes). On average, 2 perforators were isolated with each flap; increased number of perforators had a positive correlation with operative time (r = 0.4957; P = 0.0034). Vessel size and coupler data may be found in Table 2.
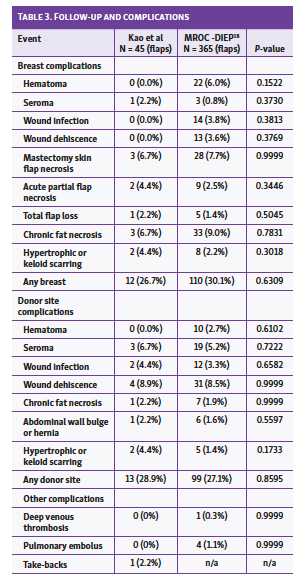
Overall flap survival rate was 97.8%. Major complications included 1 flap failure (2.2%) and 2 flaps with acute partial necrosis (4.4%). Both cases of partial necrosis were salvaged to complete breast reconstruction after debridement alone. Any breast complication was identified in 12 (26.7%) flaps, and any donor site complication in 13 (28.9%) flaps. The complication profile may be viewed alongside the MROC 1-year DIEP result in Table 3; no statistical differences were noted. Average length of hospital stay was 4.82 days (range 4 to 7 days). Mean follow up was 12.28 months.
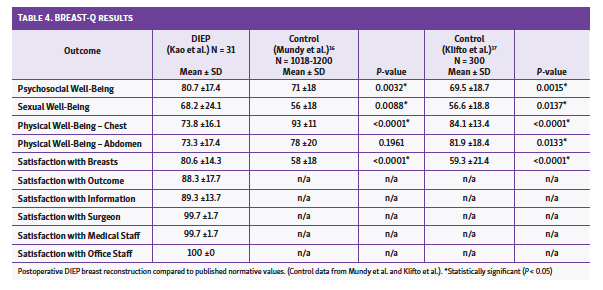
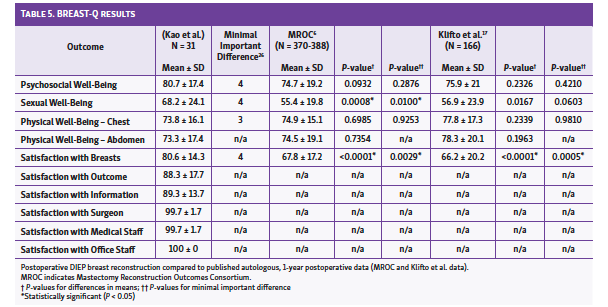
BREAST-Q surveys revealed the following: psychosocial well-being (80.7 ± 17.4), sexual well-being (68.2 ± 24.1), physical well-being − chest (73.8 ± 16.1), physical well-being − abdomen (73.3 ± 17.4), satisfaction with breasts (80.6 ± 14.3), satisfaction with outcome (88.3 ± 17.7), satisfaction with information (89.3 ± 13.7), satisfaction with surgeon (99.7 ± 1.7), satisfaction with medical staff (99.7 ± 1.7), and satisfaction with office staff (100 ± 0). Comparison of quality-of-life and satisfaction scores against published normative (noncancer, unoperated patients) and patients undergoing DIEP breast reconstruction are listed in Table 4 and Table 5, respectively.
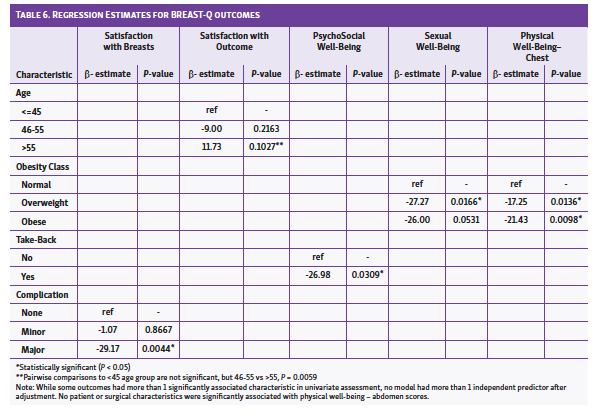
Simple linear regression analysis identified relationships between BREAST-Q scores and patient/surgical characteristics; relationships with statistical significance were then examined with multiple linear regression models. Independently related factors with statistical significance are summarized in Table 6. Patients experiencing a major complication reported satisfaction with breast scores 29 points lower (P = 0.0044) when compared to those without complications. Scores for those with minor complications were not statistically different from those without complications. Age group was independently related to satisfaction with outcome scores (P = 0.0203). Patients over 55 years of age reported scores that were on average 21 points higher than those aged 46 to 55 years (P = 0.0059). An unplanned return to the operating room (“take-back”) negatively impacted scores for psychosocial well-being, with a 26.98-point reduction (P = 0.0309). Sexual well-being and physical well-being – chest scores were inversely related to increasing BMI when compared to normal weight patients (P = 0.0465 and P = 0.0186, respectively). No factors were associated with physical well-being – abdomen.
Discussion
The authors have demonstrated favorable PRO measures and successful DIEP breast reconstruction at a low-volume center (<17 flaps annually) without fellowship-trained microvascular surgeons. The ASPS published measures of quality performance for patients undergoing autologous breast reconstruction and 5 quality measures were identified: coordination of patient care prior to surgery, patient satisfaction with reported scores of 65 or higher on BREAST-Q, discharge by postoperative day 4, operative time less than 8 hours for unilateral breast reconstruction, and absence of blood transfusion.19 The results have been consistent with these standards – all patients were referred to a preoperative multidisciplinary clinic, patient satisfaction scores have exceeded the benchmark BREAST-Q scores of 65, and no patients received a blood transfusion. Two exceptions may be found: 1) unilateral operative time of 8:08, and 2) 4.85-day average length of stay. However, both measures have converged with the ASPS quality measures over the last year, as the authors’ experience increased. (Figure 2)
A review of the Nationwide Inpatient Sample Database from 2010 to 2011 revealed 86.9% of DIEP flap surgeries were performed in urban teaching hospitals, and 87.3% were performed in large hospitals.9 The experience at a community hospital was comparable to that described in the literature within large teaching hospitals.18 Previously, the performance of DIEP flap breast reconstruction by microvascular surgeons within the community was investigated by Wildt et al; they found no significant differences between university and community hospitals in total complication rate, flap loss, or need for surgical intervention.14 Similarly, Nelson et al compared outcomes of 2 academic surgeons performing free flap breast reconstruction in community vs. university hospitals.20 They described shorter operative times, greater blood loss, and more frequent blood transfusions within the community setting; however, no significant differences in complications were identified. Gusenoff et al also examined free tissue transfer performed by academic surgeons in differing hospital settings and found no significant differences in complications.13
In the aforementioned work, however, all of the surgeons had formal microvascular training; none of the surgeons in this study had fellowship training. The impact of a lack of fellowship training on complication rates was examined by Orbay et al.12 They demonstrated a higher partial flap necrosis rate compared to those described in the literature (14.7% vs. 1.6%), as well as a higher rate of venous complications (11.7% vs. 3.3%); however their total flap loss rate proved comparable (2.9% vs. 2.2%). These results trend similarly with the authors’ flap loss results.
When examining complications, results in this study were comparable to those of MROC – a prospective multicenter cohort study of mastectomy reconstruction patients from 11 centers in North America.18 When comparing breast complications, such as hematoma, seroma, wound infection, wound dehiscence, mastectomy skin flap necrosis, total flap loss, acute partial flap necrosis, total flap loss, chronic fat necrosis, and hypertrophic scars, results were not statistically different (P > 0.05). (Table 3) When comparing donor site complications, all values including hematoma, seroma, wound infection, wound dehiscence, chronic fat necrosis, abdominal bulge, or hypertrophic scarring were not statistically different (P > 0.05). (Table 3)
Several authors have described an increased complication rate associated with the learning curve of microvascular breast reconstruction.10,21–23 In contrast, other authors have described the learning curve as a shortening of operative times without significant changes in complication rates.11,15,24 The authors’ experience corresponds with the latter cohort. Though the surgical protocol did not change between 2016 and 2020, increased operating room efficiency was achieved by virtue of repetition.
Limitations
A weakness of this study lies in the low number of patients and flaps; the surgeons performed 45 flaps in 33 patients over a 32-month period (17 flaps per year). The power to detect relationships in the regression analysis is limited, and additional independent relationships could be identified (or debunked) with a larger sample size. However, this low volume is the focus of the work. Tanna et al. examined the volume-outcome relationship for immediate breast reconstruction to determine whether complication rates would vary based on hospital or provider volume.25 They analyzed the California Office of Statewide Health Planning and Development discharge database and divided hospital volume into quartiles as high-volume (>42 per year), medium-volume (20 to 42 per year), low-volume (8 to 19 per year) and very low-volume (1 to 7 per year). They identified high-volume hospitals as having the fewest complications, and medium- or very low-volume hospitals as having the most. Interestingly, the volume-outcome relationship was imperfect, with low-volume hospitals demonstrating similar complication rates as high-volume hospitals, and better rates than medium-volume hospitals. This corresponds with the authors findings. Ironically, it is the low volume of cases that makes it difficult to pinpoint the structural and process measures that contribute to these results.
Another limitation of this study lies in the use of only postoperative BREAST-Q results. Rather than using preoperative questionnaires as a baseline, normative data compiled by Mundy et al16 and Klifto et al were used in this study.17 The authors chose to compare postoperative data with those of patients without a history of breast cancer or breast reconstruction. As Klifto states, “because the diagnosis with breast cancer affects women both physically and psychologically, it is important to have baseline scores representative of patients’ self-perception and quality of life before cancer diagnosis or knowledge of future interventions that will alter one’s appearance.”17 By comparing PROs from the series with normative data from women without breast cancer, the authors could better understand the absolute change in patient perceptions. The authors also compared the BREAST-Q PRO’s with the MROC and Klifto 1-year postoperative results after DIEP breast reconstruction to provide a benchmark for interpretation of the data. The results revealed significantly greater scores in psychosocial well-being, sexual well-being and breast satisfaction in comparison to both sets of preoperative, normative values. As would be expected, physical well-being − chest and abdomen scores were significantly lower than those reported by patients without prior surgery. (Table 4) When benchmarking against the postoperative MROC and Klifto data, no significant differences in psychosocial well-being or physical well-being of the chest or abdomen (P > 0.05) may be seen. (Table 5) However, the cohort reported sexual well-being and breast satisfaction scores that were statistically superior (P < 0.05, P < 0.001, respectively). Furthermore, the findings are clinically meaningful when applying the smallest change in BREAST-Q scores that patients perceive as important: satisfaction with breasts – 4, psychosocial well-being – 4, physical well-being – 3, and sexual well-being – 4.26
The authors also sought relationships between patient and surgical characteristics and BREAST-Q scores by using regression
models. (Table 6) It should be noted that no significant correlations were found with preoperative breast characteristics, prior breast surgery, or timing of breast reconstruction. This is consistent with previous publications.27,28 Conversely, factors that diminished PROs merit discussion. Satisfaction with outcome scores, though high overall (88.3 ± 17.7), were significantly decreased in patients aged 46 to 55 years. Within the raw data, there was a trend for lower scores noted for questions such as, “I would do it again,” and “the outcome perfectly matched my expectations.” This may reflect differing preoperative expectations in the middle-aged patient population. Sexual well-being and physical well-being − chest scores were reduced with increased BMI class; this could represent postoperative challenges faced by patients who were obese or with increased discomfort posed by larger flaps. Satisfaction with breasts was negatively influenced by total flap loss or acute partial necrosis, and psychosocial well-being was lower after a take-back. These adverse events have a clear impact on the patient experience and avoidance of these complications is critical.
The exceptional breast satisfaction scores warrant close scrutiny due to the unique patient population. The cohort was primarily of Native Hawaiian or Asian descent (72.7%), and these characteristics may not be representative of those in prior studies (MROC percent of race non-White or Black patients was 7.6%; Klifto percent of Asian patients was 3.3%).6,17 Regarding race, the regression analysis did not identify significant relationships between race and satisfaction. Prior work similarly described the influence of race with no differences in satisfaction of breast identified between racial or ethnic groups.29 An alternative hypothesis for such high satisfaction with breasts may relate to BMI, as the population was predominantly overweight and obese. Though regression analysis did not find an association, Ochoa et al examined the impact of obesity and they identified an inverse relationship between increasing BMI and lower baseline PRO’s.30 In particular, preoperative breast satisfaction scores and psychosocial well-being were lower for patients who were obese or severely obese, respectively. However, all patients, regardless of BMI, demonstrated significant increases in postoperative satisfaction with breast appearance, sexual well-being, and psychosocial well-being. The preoperative correlation between obesity and poor body image could account for improved satisfaction after DIEP breast reconstruction.
Conclusion
This study demonstrated that microsurgical abdominal flap breast reconstruction can be performed at a high level of quality by motivated surgeons without microvascular fellowship training at a community hospital. The authors do not suggest that all plastic surgeons or those without any experience should perform these complex cases. For those beginning DIEP reconstruction, microvascular courses are available, and it would be prudent to observe or assist with several cases prior to embarking alone. A stepwise approach − beginning with immediate, unilateral, right-sided breast reconstruction after skin-sparing mastectomy in healthy, non-radiated patients with BMI less than 30 – is recommended. This cohort would simplify reconstruction as there would be no scar burden about the internal mammary vessels, the right-sided anastomoses tend to be easier due to larger vessel diameter, and the modest flap size is easily managed. Ultimately, results can be attained after overcoming the steep learning curve and allocating appropriate resources and staffing. To combat the diminishing rate of microsurgical breast reconstruction, the onus is on plastic surgeons with or without formal microsurgical training, within community and academic centers, to continue to offer the full range of breast reconstruction. A surgeons duty is to, “Do what you can, with what you’ve got, where you are.”31
Acknowledgments
Authors: Kenneth K. Kao, MD; Scott M. Nishikawa, MD; Paul D. Faringer, MD
Affiliation: Department of Plastic Surgery, Kaiser Permanente Moanalua Medical Center; Honolulu, HI.
Correspondence: Kenneth Kao, MD; Kenneth.k.kao@kp.org
Disclosure: The authors disclose no financial or other conflicts of interest.
References
1. Pusic AL, Klassen AF, Scott AM, Klok JA, Cordeiro PG, Cano SJ. Development of a new patient-reported outcome measure for breast surgery: the BREAST-Q. Plast Reconstr Surg. 2009;124(2):345-353. doi:10.1097/PRS.0b013e3181aee807
2. Nelson JA, Allen RJ, Polanco T, et al. Long-term patient-reported outcomes following postmastectomy breast reconstruction: an 8-year examination of 3268 patients. Ann Surg. 2019;270(3):473-483. doi:10.1097/SLA.0000000000003467
3. Liu C, Zhuang Y, Momeni A, et al. Quality of life and patient satisfaction after microsurgical abdominal flap versus staged expander/implant breast reconstruction: a critical study of unilateral immediate breast reconstruction using patient-reported outcomes instrument BREAST-Q. Breast Cancer Res Treat. 2014;146(1):117-126. doi:10.1007/s10549-014-2981-z
4. Yueh JH, Slavin SA, Adesiyun T, et al. Patient satisfaction in postmastectomy breast reconstruction: a comparative evaluation of DIEP, TRAM, latissimus flap, and implant techniques. Plast Reconstr Surg. 2010;125(6):1585-1595. doi:10.1097/PRS.0b013e3181cb6351
5. Hu ES, Pusic AL, Waljee JF, et al. Patient-reported aesthetic satisfaction with breast reconstruction during the long-term survivorship period. Plast Reconstr Surg. 2009;124(1):1-8. doi:10.1097/PRS.0b013e3181ab10b2
6. Pusic AL, Matros E, Fine N, et al. Patient-reported outcomes 1 year after immediate breast reconstruction: results of the Mastectomy Reconstruction Outcomes Consortium study. J Clin Oncol. 2017;35(22):2499-2506. doi:10.1200/JCO.2016.69.9561
7. Panchal H, Matros E. Current trends in postmastectomy breast reconstruction. Plast Reconstr Surg. 2017;140(5S Advances in Breast Reconstruction):7S-13S. doi:10.1097/PRS.0000000000003941
8. Momoh AO, Griffith KA, Hawley ST, et al. Postmastectomy breast reconstruction: exploring plastic surgeon practice patterns and perspectives. Plast Reconstr Surg. 2020;145(4):865-876. doi:10.1097/PRS.0000000000006627
9. Zoghbi Y, Gerth DJ, Tashiro J, Golpanian S, Thaller SR. Deep inferior epigastric perforator versus free transverse rectus abdominis myocutaneous flap: complications and resource utilization. Ann Plast Surg. 2017;78(5):516-520. doi:10.1097/SAP.0000000000000936
10. Busic V, Das-Gupta R, Mesic H, Begic A. The deep inferior epigastric perforator flap for breast reconstruction, the learning curve explored. J Plast Reconstr Aesthet Surg. 2006;59(6):580-584. doi:10.1016/j.bjps.2005.04.061
11. Grinsell DG, McCoubrey GW, Finkemeyer JP. The deep inferior epigastric perforator learning curve in the current era. Ann Plast Surg. 2016;76(1):72-77. doi:10.1097/SAP.0000000000000528
12. Orbay H, Busse BK, Stevenson TR, Wang HT, Sahar DE. Deep inferior epigastric artery perforator flap breast reconstruction without microsurgery fellowship training. Plast Reconstr Surg Glob Open. 2015;3(7):e455. doi:10.1097/GOX.0000000000000428
13. Gusenoff JA, Vega SJ, Jiang S, et al. Free tissue transfer: comparison of outcomes between university hospitals and community hospitals. Plast Reconstr Surg. 2006;118(3):671–675. doi:10.1097/01.prs.0000233203.84078.6b
14. Wildt RP de, Enajat M, Sawor JH, Fresow RNGM, Nanhekhan LV, Hulst RRWJ van der. The unilateral deep inferior epigastric perforator flap: Comparing university to community hospital. J Plast Surg Hand Surg. 2012;46(3-4):159-162. doi:10.3109/2000656X.2012.686915
15. Beudeker N, Smits I, Spierings R, et al. Starting an autologous breast reconstruction program after plastic surgical training. Is it as good as it gets? J Plast Reconstr Aesthet Surg. 2020;73(2):286-294. doi:10.1016/j.bjps.2019.07.022
16. Mundy LR, Homa K, Klassen AF, Pusic AL, Kerrigan CL. Breast Cancer and Reconstruction: Normative Data for Interpreting the BREAST-Q. Plast Reconstr Surg. 2017;139(5):1046e-1055e. doi:10.1097/PRS.0000000000003241
17. Klifto KM, Aravind P, Major M, et al. Differences between breast cancer reconstruction and institutionally established normative data using the BREAST-Q reconstruction module: a comparative study. Plast Reconstr Surg. 2020;145(6):1371-1379. doi:10.1097/PRS.0000000000006810
18. Wilkins EG, Hamill JB, Kim HM, et al. Complications in postmastectomy breast reconstruction one-year outcomes of the Mastectomy Reconstruction Outcomes Consortium (MROC) study. Ann Surg. 2018;267(1):164-170. doi:10.1097/SLA.0000000000002033
19. Siddiqui A, Ueno C, Agarwal J, et al. Evidence-based performance measures for autologous breast reconstruction: an American Society of Plastic Surgeons quality performance measure set. Plast Reconstr Surg. 2020;145(2):284e-294e. doi:10.1097/PRS.0000000000006478
20. Nelson JA, Stransky CA, Fischer JP, Fosnot J, Serletti JM, Wu LC. Reexamining free flap breast reconstruction in the community and university setting: is there a difference? Ann Plast Surg. 2014;73 Suppl 2:S171-174. doi:10.1097/SAP.0000000000000204
21. Acosta R, Smit JM, Audolfsson T, et al. A clinical review of 9 years of free perforator flap breast reconstructions: an analysis of 675 flaps and the influence of new techniques on clinical practice. J Reconstr Microsurg. 2011;27(2):91-98. doi:10.1055/s-0030-1267835
22. Hofer SOP, Damen THC, Mureau MAM, Rakhorst HA, Roche NA. A critical review of perioperative complications in 175 free deep inferior epigastric perforator flap breast reconstructions. Ann Plast Surg. 2007;59(2):137-142. doi:10.1097/01.sap.0000253326.85829.45
23. Cubitt J, Barber Z, Khan AA, Tyler M. Breast reconstruction with deep inferior epigastric perforator flaps. Ann R Coll Surg Engl. 2012;94(8):552-558. doi:10.1308/003588412X13373405386457
24. Bodin F, Dissaux C, Lutz J-C, Hendriks S, Fiquet C, Bruant-Rodier C. The DIEP flap breast reconstruction: Starting from scratch in a university hospital. Ann Chir Plast Esthet. 2015;60(3):171-178. doi:10.1016/j.anplas.2015.02.005
25. Tanna N, Clayton JL, Roostaeian J, Perry AD, Crisera CA. The volume-outcome relationship for immediate breast reconstruction. Plast Reconstr Surg. 2012;129(1):19-24. doi:10.1097/PRS.0b013e31821e70ff
26. Voineskos SH, Klassen AF, Cano SJ, Pusic AL, Gibbons CJ. Giving meaning to differences in BREAST-Q scores: minimal important difference for breast reconstruction patients. Plast Reconstr Surg. 2020;145(1):11e-20e. doi:10.1097/PRS.0000000000006317
27. Sinha S, Ruskin O, D’Angelo A, McCombe D, Morrison WAJ, Webb A. Are overweight and obese patients who receive autologous free-flap breast reconstruction satisfied with their postoperative outcome? A single-centre study. J Plast Reconstr Aesthet Surg. 2016;69(1):30-36. doi:10.1016/j.bjps.2015.08.036
28. Yoon AP, Qi J, Brown DL, et al. Outcomes of immediate versus delayed breast reconstruction: results of a multicenter prospective study. Breast. 2018;37:72-79. doi:10.1016/j.breast.2017.10.009
29. Berlin NL, Momoh AO, Qi J, et al. Racial and ethnic variations in one-year clinical and patient-reported outcomes following breast reconstruction. Am J Surg. 2017;214(2):312-317. doi:10.1016/j.amjsurg.2017.02.009
30. Ochoa O, Garza R, Pisano S, et al. Prospective longitudinal patient-reported satisfaction and health-related quality of life following DIEP flap breast reconstruction: relationship with body mass index. Plast Reconstr Surg. 2019;143(6):1589-1600. doi:10.1097/PRS.0000000000005616
31. Roosevelt, T. Theodore Roosevelt: An Autobiography. Charles Scribner’s Sons; 1920.