

Choosing Therapy for Type 2 Diabetes Based on Patient-Related Variables
San Diego—With the expanding availability of multiple drugs to treat patients with type 2 diabetes, treatment can now be better tailored to the particular needs of each patient.
Speaking at a satellite symposia at AMCP, Stuart T. Haines, PharmD, professor and vice chair, Clinical Services, University of Maryland School of Pharmacy, Baltimore, MD, explored recent evidence on antihyperglycemic treatment strategies including add-on therapies for patients with type 2 diabetes described in 2 recently published guidelines in 2015 by the American Diabetes Association/European Association for the Study of Diabetes and the American Association of Clinical Endocrinology. The event was sponsored by an educational grant from AstraZeneca.
Along with a number of medications approved to treat type 2 diabetes before 2000 (eg, exogenous insulin, sulfonylureas, metformin, alpha-glucosidase inhibitors [AGIs], meglitinides, and thiazolidinediones [TZDs]), a number of new classes of drugs approved since 2005 has expanded the treatment armamentarium and allowed for a more personalized approach to treatment.
The more recent drug classes include the glucagon-like peptide-1 receptor agonists (GLP-1 RAs), amylin analogues, dipeptidly peptidase-4-inhibitors (DPP-4 inhibitors), bile acid sequestrant, dopamine agonist, and sodium-glucose cotransporter 2 inhibitors (SGLT-2 inhibitors).
“The treatment of type 2 diabetes has been increasingly complex as we have more than 12 classes of medications from which to select,” said Dr. Haines, adding that choice of a treatment strategy should take into account variables unique to each individual patient.
One strategy to achieve this is to treat patients with multiple therapies. “Although metformin remains the cornerstone of therapy, not everyone can tolerate it,” he said. “Moreover, most patients require more than one agent to achieve good glycemic control. Many questions remain about what the best add-on therapy to metformin should be.”
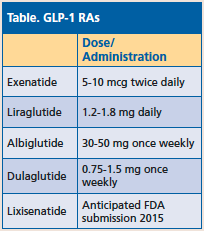 Dr. Haines spoke about the current GLP-1 RAs on the market (Table). Currently, there are 7 studies, including 1 head-to-head study, evaluating these agents as an add-on to metformin.
Dr. Haines spoke about the current GLP-1 RAs on the market (Table). Currently, there are 7 studies, including 1 head-to-head study, evaluating these agents as an add-on to metformin.
Overall, the primary benefits of these agents as monotherapy or as add-on therapy for patients with type 2 diabetes is lowering of blood glucose levels (A1c) by 1 to 1.7% while avoiding, for the most part, hypoglycemia. In addition, these agents promote weight loss (in most patients by 1-4 kg) by promoting a reduction in appetite and food intake.
The most common adverse effects with these drugs include mild-moderate nausea that usually peaks in 4 to 10 weeks and resolves in most patients, and hypoglycemia based on the patient’s background therapy and largely when combined with insulin and insulin secretagogues.
When choosing these agents, or any type of add-on therapies, clinicians need to weigh practical considerations such as what agent is the best for a given patient (ie, appropriate, potential added benefits, mitigating adverse effects, potential long-term risks, etc), will the patient have access to the medication (ie, cost issues and formulary considerations), and can the patient use the medication appropriately (ie, issues involved in drug administration technique, initiating and titrating the drug, and monitoring therapy).
“Treatment decisions should be based on individual patient-related variables such as weight and risk of hypoglycemia as well as treatment cost and complexity,” Dr. Haines.—Mary Beth Nierengarten



