

1.2 Plaque Modification: When to Apply Ablative vs Disruptive Therapies
These proceedings summarize the educational activity of the 17th Biennial Meeting of the International Andreas Gruentzig Society held January 30 to February 2, 2024 in Chiang Rai, Thailand.
Faculty Disclosures Vendor Acknowledgments
Statement of the problem or issue
Severe calcium is noted in target coronary lesions in about 18% to 26% of patients undergoing PCI.1,2 Importantly, calcium is associated with greater procedural complication rates, lower procedural success rates, and higher rates of restenosis and stent thrombosis. Plaque modification techniques can improve initial PCI success rates in calcified coronary lesions, however, they are used in <10% of PCI procedures overall, and there is wide variability across hospitals.3 For example, rates of coronary atherectomy range from <2% up to 15% of PCI procedures. Some of this variability in use may be due to institutional factors (availability of devices) along with operator-comfort levels. Over the past decade there has been a steady increase in use of plaque modification techniques, most notably since the introduction of intravascular lithotripsy.4
The approach to the treatment of calcified lesions, and the decision to proceed with plaque modification is best determined with intracoronary imaging — either OCT or IVUS. Plaque modification is generally indicated when OCT images reveal the following features: An arc of calcium that is >180 degrees in extent, a calcified lesion length >5 mm, and calcification that is >0.5 mm in depth. With IVUS, a calcium arc of >180 degrees (but more specifically 270 to 360 degrees), and calcium >5 mm in length are indications for plaque modification. Angiographic criteria, such as dense calcium on both sides of the arterial wall, can also be used. Additionally, inability to deliver the IVUS catheter or other devices across the lesion is usually a reliable sign that plaque modification is needed.
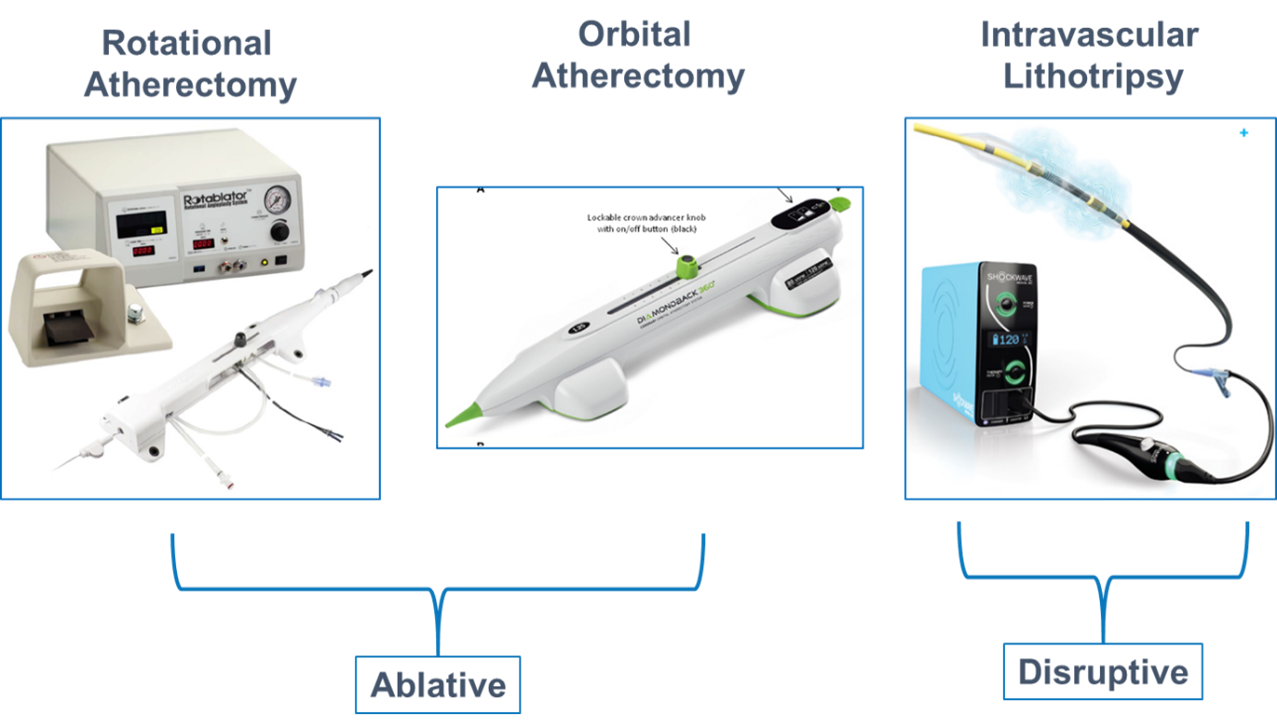
Presently, there are 3 technologies available to assist in modifying heavily calcified coronary plaques. These include ablative and disruptive devices. Rotational atherectomy and orbital atherectomy are classified as ablative, while intravascular lithoplasty is classified as disruptive. The device configurations are illustrated in Figure 1. This figure does not include all devices. Some other devices include the laser catheter (which is technically classified as one of the ablative therapies), cutting or scoring balloons (classified as ablative), and ultra-high pressure balloons (classified as disruptive). While these other devices have been used to treat calcified lesions, they generally have not been effective in cases of severe calcification.
Figure 1. Currently available plaque modification technologies.
Gaps in current knowledge
Despite improved procedural success and better stent expansion, randomized trial data have not consistently reported improvements in longer-term clinical outcomes with plaque modification devices. While use of plaque modification has increased over time, the rate of use is still quite low. This may be due to several factors. First, interventional cardiologists with lower volumes may not be comfortable using the ablative equipment. This equipment requires special training and/or proctoring and there is a learning curve that must be assimilated. Second, both rotational and orbital atherectomy catheters require special guidewires that are often difficult to deliver across tortuous lesions. On the other hand, intravascular lithoplasty catheters can be used with any guidewire and do not require formal training or proctoring. Selected comparisons of the 3 technologies are shown in the table. The listed features depict the strengths and limitations of each device and illustrate some of our gaps in knowledge. Most importantly, we lack full understanding of the appropriate niche or range of application for each device.
Table. Selected comparison of ablative and disruptive therapies.
|
Feature |
Rotational Atherectomy |
Orbital Atherectomy |
Intravascular Lithotripsy |
|
Deliverability |
+++ |
++ |
+ |
|
Wire |
Roto-wire |
Viper |
Any |
|
Cost |
$1925 |
$3795 |
$4700 |
|
Learning Curve |
+++ |
++ |
+ |
|
Certification |
Proctor/Formal Training |
Proctor/Formal Training |
None |
|
Risk of Perforation |
+++ |
++ |
-/+ |
|
No Reflow |
++ |
++ |
- |
|
Niche |
Diffuse disease Uncrossable Ostial |
Diffuse disease Uncrossable |
Focal lesions Large vessels Calcified Nodules |
Possible solutions and future directions
What are the unanswered questions we have, and what does the future hold? Is there an ideal technique to perform plaque modification? Can we derive algorithms to match lesion characteristics and overall anatomy that would favor one device and avoid the use of multiple devices? A recent review addressed this question and proposed a useful algorithm.5
Can existing devices be modified for easier use and better deliverability? This could facilitate greater device use by interventionalists. Finally, how can we ensure that operators across the country become comfortable in using devices for plaque modification?
References
- Hemetsberger R, Abdelghani M, Toelg R, et al. Impact of coronary calcification on clinical outcomes after implantation of newer-generation drug-eluting stents. J Am Heart Assoc. 2021;10(12):e019815. doi: 10.1161/JAHA.120.019815. PMID: 34056911.
- Lee MS, Yang T, Lasala J, Cox D. Impact of coronary artery calcification in percutaneous coronary intervention with paclitaxel-eluting stents: Two-year clinical outcomes of paclitaxel-eluting stents in patients from the ARRIVE program. Catheter Cardiovasc Interv. 2016;88(6):891-897. doi: 10.1002/ccd.26395. PMID: 26756859.
- Beohar N, Kaltenbach LA, Wojdyla D, et al. Trends in usage and clinical outcomes of coronary atherectomy: A report from the National Cardiovascular Data Registry CathPCI Registry. Circ Cardiovasc Interv. 2020;13(2):e008239. doi: 10.1161/CIRCINTERVENTIONS.119.008239. PMID: 31973557.
- Butala, NM, Waldo SW, Secemsky EA, et al. Use of calcium modification during percutaneous coronary intervention after introduction of coronary intravascular lithotripsy. JSCAI. 2024;3:101254. doi.org/10.1016/j.jscai.2023.101254
- Barbato E, Gallinoro E, Abdel-Wahab M, et al. Management strategies for heavily calcified coronary stenoses: an EAPCI clinical consensus statement in collaboration with the EURO4C-PCR group. Eur Heart J. 2023;44(41):4340-4356. doi: 10.1093/eurheartj/ehad342. PMID: 37208199.
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.









