

2.1 TAVR for Aortic Insufficiency: Latest Devices and Do We Have “Sufficient” Evidence?
These proceedings summarize the educational activity of the 17th Biennial Meeting of the International Andreas Gruentzig Society held January 30 to February 2, 2024 in Chiang Rai, Thailand.
Faculty Disclosures Vendor Acknowledgments
Statement of the problem or issue
Comprehensive screening studies have shown repeatedly that aortic valve regurgitation (AR) is common, and, in general, is found more frequently than aortic valve stenosis (AS). In the OxVALVE study, the HONU community study, and a large study from Guangzhou, China, AR was first or second in frequency for valvular defects, between 4% to 8% of screened patients, whereas AS was much less common, between 0.5% to 2%.1,2,3 Interestingly, when echo and cardiac magnetic resonance imaging (cMRI) imaging are performed and compared for the same patients, cMRI identifies AR more frequently and in greater severity than echo imaging.4,5 This finding has led to efforts to redefine the parameters used for classifying “severe AR,” which in turn will change guideline recommendations for invasive therapies. Already, the US and European guidelines have begun to differ somewhat on definitions and recommendations for AR. For example, in US guidelines, LV systolic dysfunction is defined as LVEF ≤55%, whereas in European guidelines it is defined as LVEF ≤50%.
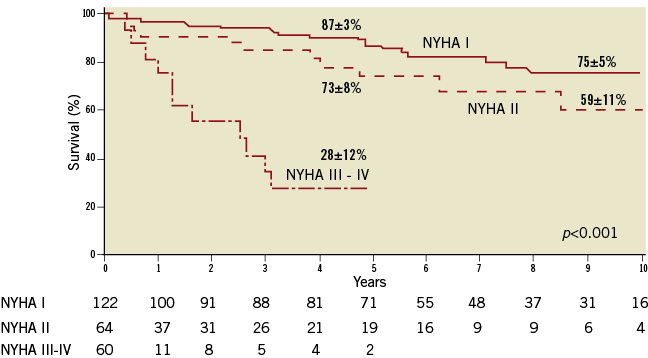
Critically, long-term survival in patients with AR is not favorable. Over time, as LV dimensions enlarge due to chronic volume overload, and LV performance deteriorates, symptoms of heart failure develop. With severe symptoms (NYHA Class II-IV) mortality may be greater than 70% at 5 years. (See Figure 1).6
Figure 1. Survival in patients with AR by NYHA class. From: EuroIntervention 2013;10;9 Suppl:S55-62.
Surgical aortic valve replacement (SAVR) improves long-term outcomes in AR compared to medical therapy. The survival benefits appear to be greater for patients with more impaired LV function (LVEF<50%) compared to patients with normal LV function (Figure 2). However, the problem is that many patients with severe symptomatic AR and low LVEF are deemed “too high risk” for surgery. The Euro Heart Survey reported that only 37% of patients with LVEF >50% underwent SAVR, only 22% with LVEF 30%-50%, and only 3% with LVEF <30%.7
Transcatheter aortic valve replacement (TAVR) has now begun to be performed for isolated AR, that is, even when there is no AS present. Many issues regarding TAVR for AR remain to be settled. New valves are under development or investigation.
Figure 2. Survival in patients with AR by treatment. From: Structural Heart. 2021;5:608-618.
Gaps in current knowledge
There are several areas that need clarification in TAVR for AR. For one, technologies for anchoring the device require improvement. Current valves often have insufficient anchoring. With AR, the aortic root is often dilated and the annulus is enlarged. When this dilated and enlarged anatomy is coupled with insufficient anchoring, this can lead to valve dislocation and possible embolization. The question of valve durability over many years of implanted life requires further studies. Additionally, how to approach AR when left ventricular support devices (LVAD) are in place, or needed, will require creative investigations.
Possible solutions and future directions
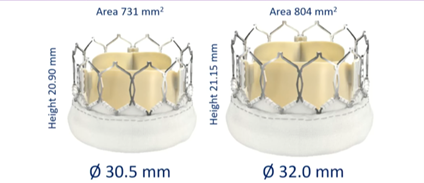
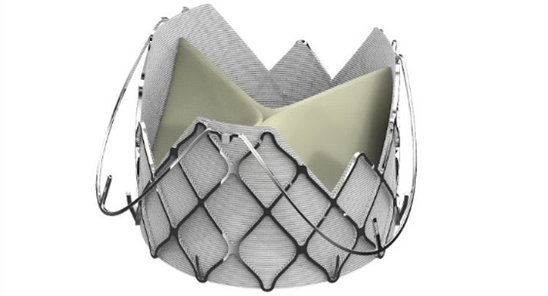
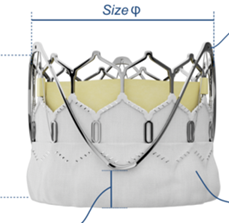
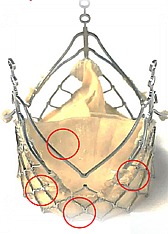
Examples of newer aortic valve designs that may be applicable for TAVR in AR are shown in Figure 3.
Figure 3. Newer aortic valves for TAVR in AR.


Studies underway or planned will help us answer many of the remaining questions. We do have sufficient evidence that untreated severe AR is associated with worse outcomes compared to surgical treatment (SAVR). Many new transcutaneous valve devices are becoming available. The field of TAVR for AR is only just in its infancy.
References
- d'Arcy JL, Coffey S, Loudon MA, et al. Large-scale community echocardiographic screening reveals a major burden of undiagnosed valvular heart disease in older people: the OxVALVE Population Cohort Study. Eur Heart J. 2016;37(47):3515-3522. Epub 2016 Jun 26. doi: 10.1093/eurheartj/ehw229 PMID: 27354049; PMCID: PMC5216199
- Gössl, M, Stanberry, L, Benson, G. et al. Burden of undiagnosed valvular heart disease in the elderly in the community: Heart of New Ulm Valve Study. J Am Coll Cardiol Img. JACC Cardiovasc Imaging. 2023;16(8):1118-1120. Epub 2023 Apr 12. doi: 10.1016/j.jcmg.2023.02.009.
- He S, Deng H, Jiang J, et al. The evolving epidemiology of elderly with degenerative valvular heart disease: The Guangzhou (China) Heart Study. Biomed Res Int. 2021;2021:9982569. doi: 10.1155/2021/9982569 PMID: 33981773; PMCID: PMC8088353.
- Kammerlander AA, Wiesinger M, Duca F, et al. Diagnostic and prognostic utility of cardiac magnetic resonance imaging in aortic regurgitation. JACC Cardiovasc Imaging. 2019;12(8 Pt 1):1474-1483. Epub 2018 Nov 15. doi: 10.1016/j.jcmg.2018.08.036 PMID: 30448117.
- Neisius U, Tsao CW, Hauser TH, et al. Aortic regurgitation assessment by cardiovascular magnetic resonance imaging and transthoracic echocardiography: intermodality disagreement impacting on prediction of post-surgical left ventricular remodeling. Int J Cardiovasc Imaging. 2020;36(1):91-100. Epub 2019 Aug 14. doi: 10.1007/s10554-019-01682-x. PMID: 31414256
- Roy D, Sharma R, Brecker SJ. Native aortic valve regurgitation: transcatheter therapeutic options. EuroIntervention. 2013;10;9 Suppl:S55-62. doi: 10.4244/EIJV9SSA11 PMID: 24025959
- Iung B, Baron G, Butchart EG, et al. A prospective survey of patients with valvular heart disease in Europe: The Euro Heart Survey on Valvular Heart Disease. Eur Heart J. 2003;24:1231-1243. doi: 10.1016/s0195-668x(03)00201-x PMID: 12831818.
- Thourani VH, Brennan JM, Edelman JJ, et al. Treatment patterns, disparities, and management strategies impact clinical outcomes in patients with symptomatic severe aortic regurgitation. Structural Heart 2021;5:608-618. doi: 10.1080/24748706.2021.1988779
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.












{kind=link}