

4.2 Therapies to Minimize Myocardial Injury and to Promote Myocardial Recovery Following STEMI
These proceedings summarize the educational activity of the 16th Biennial Meeting of the International Andreas Gruentzig Society held January 31-February 3, 2022 in Punta Cana, Dominican Republic
Faculty Disclosures Vendor Acknowledgments
2022 IAGS Summary Document
Statement of the problem or issue
Despite tremendous efforts over the past 40+ years, 30-day mortality in patients with ST–segment-elevation myocardial infarction (STEMI) remains ≈10%, and late mortality is significantly higher still. This makes STEMI a leading cause of death in western civilization. STEMI most often results from rupture of a vulnerable atherosclerotic plaque in a major epicardial coronary artery, with intraluminal thrombus formation leading to occlusion of this infarct-related artery (IRA). Occlusion leads to necrosis of myocardium in the IRA distribution zone. Animal and human studies show that IRA reperfusion must occur within 2 hours after onset of symptoms for significant myocardial salvage to occur. Unfortunately, after onset of symptoms, many patients delay contacting emergency medical system (EMS) providers until more than 2 hours of time has passed. Therefore, quickly initiating IRA reperfusion with fibrinolysis in the field or pre-transfer could achieve reperfusion sooner, with significant decreases in mortality, provided the risks of fibrinolysis are small. Previous randomized prehospital fibrinolytic trials excluded high-risk patients (cardiogenic shock or brief cardiac arrest) and they used higher doses of lytics than necessary. This resulted in worse outcomes compared with primary PCI (pPCI) and so enthusiasm for fibrinolysis diminished. We have learned that merely reducing door-to-balloon times in STEMI patients treated with pPCI alone has failed to demonstrate improved outcomes over the past 10 years. The major reason for the persistently high mortality in STEMI patients seems to be the fact that IRA reperfusion in the current system typically occurs beyond the 90- to 120-minute window for significant myocardial salvage. Also, paradoxically, restoration of oxygenated blood flow into the ischemic myocardium can lead to additional myocardial necrosis, a process termed reperfusion injury. Currently, there are no definitive effective treatments for prevention of reperfusion injury.
Gaps in knowledge
It is very likely that “newer” strategies to achieve prompt IRA reperfusion would markedly improve outcomes in STEMI patients. In addition to this, a handful of therapies have shown some promise of eliminating or dramatically reducing the additional myocardial damage from reperfusion injury. In order to fully investigate effectiveness of any new therapies, it will be essential to include high-risk patients (brief cardiac arrest or cardiogenic shock) in clinical trials. It is now clear that these high-risk patients are the ones most likely to benefit from aggressive treatment.1
Possible solutions and future directions:
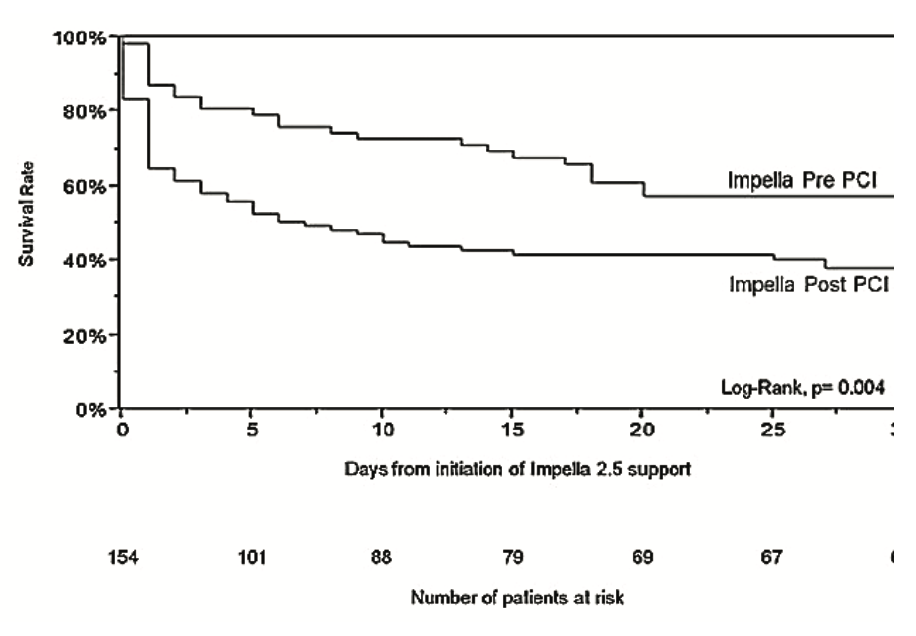
Nonrandomized studies of half-dose fibrinolysis given with aspirin, glycoprotein IIb/IIIa inhibitors, and low-dose heparin administered pre-hospital (or pre-transfer from spoke hospitals) prior to PCI have demonstrated dramatic reductions in mortality without a bleeding or stroke penalty compared with pPCI alone. But it will be necessary to perform RCTs to demonstrate definitively the benefit of half-dose fibrinolytic administration followed by urgent PCI. We also know from animal experiments, observational studies, and limited RCTs that unloading the left ventricle (LV) with an intra-aortic balloon pump (IABP) or transvascular LVAD such as Impella prior to IRA reperfusion can significantly reduce late mortality and heart failure/shock (Figure 1).2,3 The benefit of unloading may be related to reduction in reperfusion injury.
In conclusion, we must perform adequately powered randomized trials including both high-risk and intermediate-risk STEMI patients to prove the benefits of accelerated reperfusion and LV unloading for infarct salvage improved recovery.
References
1. Herrmann HC, Lu J, Brodie BR, et al. Benefit of facilitated percutaneous coronary intervention in high-risk ST-segment elevation myocardial infarction patients presenting to nonpercutaneous coronary intervention hospitals. JACC Cardiovasc Interv. 2009;2(10):917-924. doi:10.1016/j.jcin.2009.06.018
2. LeDoux JF, Tamareille S, Felli PR, Amirian J, Smalling RW. Left ventricular unloading with intra-aortic counterpulsation prior to reperfusion reduces myocardial release of endothelin-1 and decreases infarction size in a porcine ischemia-reperfusion model. Catheter Cardiovasc Interv. 2008;72(4):513-521. doi:10.1002/ccd.21698
3. O’Neill WW, Schreiber T, Wohns DH, et al. The current use of Impella 2.5 in acute myocardial infarction complicated by cardiogenic shock: results from the USpella registry. J Interv Cardiol. 2014;27(1):1-11. doi:10.1111/joic.12080














{kind=link}