

9.2 Renal Denervation: Comparison of Latest Therapeutic Approaches and Indications. Do We Need AUC Criteria?
These proceedings summarize the educational activity of the 17th Biennial Meeting of the International Andreas Gruentzig Society held January 30 to February 2, 2024 in Chiang Rai, Thailand.
Faculty Disclosures Vendor Acknowledgments
Statement of the problem or issue
Chronically high blood pressure (hypertension, HTN) leads to a vicious cascade of unfavorable pathophysiological changes, from atherosclerotic disease of blood vessels, left ventricular hypertrophy (LVH) and cardiomyopathy, to adverse cardiovascular events such as MI, CHF, and arrhythmias. Similarly, there are a number of adverse effects on the cerebrovascular and peripheral vascular systems as well. The global effects of HTN are tremendous, partly due to its high prevalence and partly due to its role as one of the greatest contributing risk factors to mortality. Nearly 30% of adults worldwide and ~50% of adults in the United States (US) currently suffer from hypertension. Importantly, adequate HTN control has plateaued at 50%, with half of the US population sub-optimally treated. One of the challenges of HTN therapy is poor medication adherence, with 30%-50% of patients non-adherent to HTN medications, even in clinical trials and registries. Importantly, even small consistent reductions in blood pressure (BP) of 10mmHg over time result in ~20% relative risk reduction of major cardiovascular and cerebrovascular events, providing support for guidelines to lower blood pressure to less than 130 mm Hg.
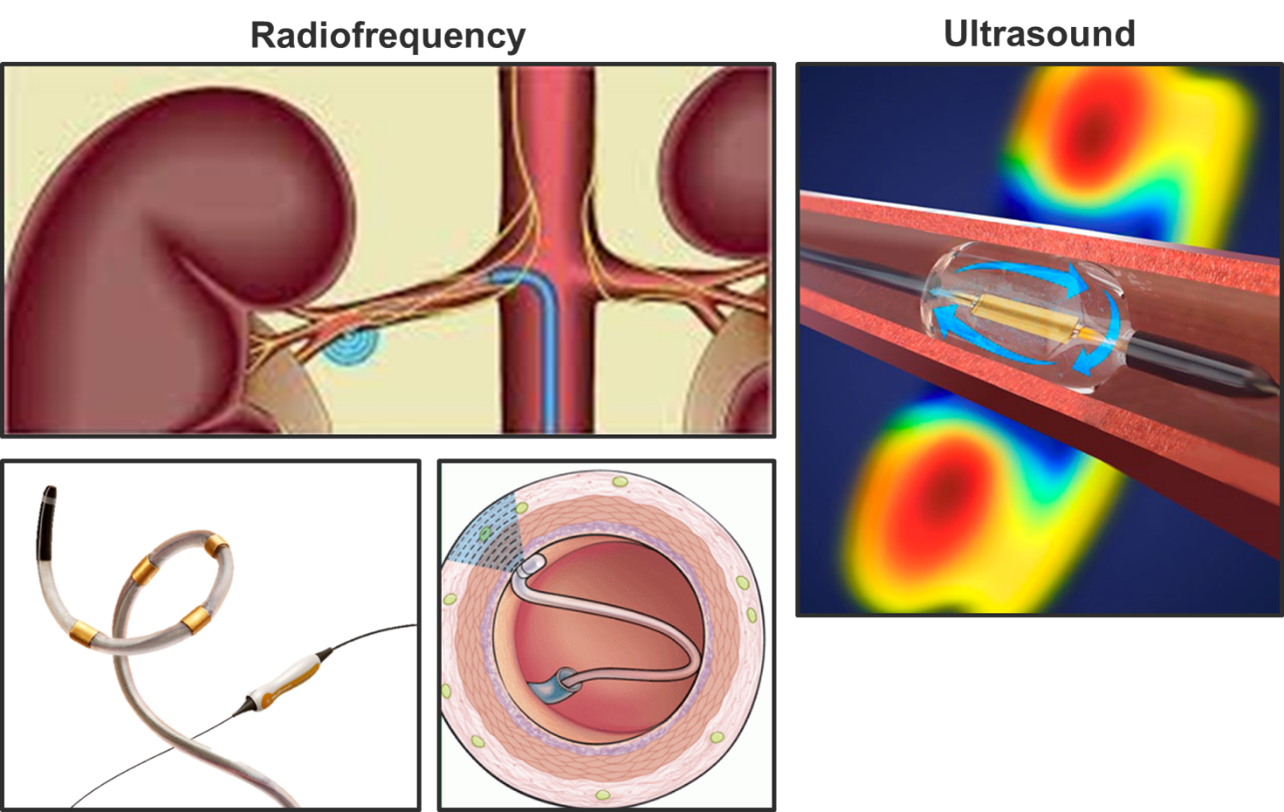
The concept of inactivating renal nerves is not novel; surgical resection of thoracolumbar sympathetic nerves was described as early as the 1930s. In the 1950s, a large study of over 1,200 patients undergoing surgical sympathectomy was published. Interestingly, surgical sympathectomy resulted in inconsistent reductions in BP, but, in those patients that achieved lower BP, there was a long-term mortality benefit. Unfortunately, surgical denervation of the lower body resulted in significant morbidity, including orthostatic hypotension, as well as bowel and bladder dysfunction. Sympathectomy as a treatment for HTN became extinct once medical management of HTN became the standard of care. More recently, the idea of performing percutaneous renal denervation without any adverse effects has resurfaced in the last 2 decades due to technological developments. Renal nerves are located in the adventitial fat layers within 3-5mm from the endoluminal space of the renal arteries. This proximity makes denervation or inactivation of renal nerves (RDN) from within the lumen of the renal arteries a target for endovascular therapies using radiofrequency (RF) energy, high-intensity ultrasound, or alcohol injection (Figure). RDN reduces renal tissue norepinephrine release and “spillover,” reduces muscle sympathetic nerve activity, decreases plasma renin levels, and increases renal plasma flow.
Figure. Renal denervation using radiofrequency (RF) energy or high-intensity ultrasound.
Gaps in current knowledge
Early trials (i.e. Symplicity HTN-3) failed to demonstrate efficacy of RDN in patients with resistant HTN. Since then, a second group of sham-controlled randomized clinical trials (RCTs), in patients with and without medication therapy, have demonstrated consistent but modest reductions in systolic, diastolic, and 24-hr average BP, and also confirmed the safety of RDN. Consistent BP reductions have been observed for up to 3 years of follow-up. Interestingly, treatment of both the main branch along with the distal branches of the renal artery has resulted in larger BP reductions when compared to treating the main branch only. These collective data led the Food and Drug Administration (FDA) in November 2023 to approve both ultrasound- and RFA-based renal denervation devices.
Several gaps remain in our knowledge of RDN therapy, mostly related to its short- and long-term efficacy, patient selection criteria, and identification of responders and non-responders:
- Who are the best candidates for RDN (clinical characteristics, biomarkers, hemodynamic parameters) and what evaluations are needed prior to referral for RDN?
- What is the explanation for non-responders (~10-30%) and can we identify pre-procedural predictors of responsiveness to RDN?
- Can we develop tests/technologies to measure baseline sympathetic activity and then validate the extent of peri-procedural denervation?
- Do we need to demonstrate importance of reducing end-organ effects and long-term cardiovascular benefits after RDN?
- What are comparative outcomes between RFA, ultrasound, and alcohol-based technologies?
- Should we investigate collateral beneficial effects of RDN in other areas (glucose/insulin sensitivity, obstructive sleep apnea, CKD, diastolic heart failure, arrythmias (e.g. atrial fibrillation, ventricular tachycardia)?
Possible solutions and future directions
Serum biomarkers identifying candidates with hyperactive renal sympathetic nervous activity need to be examined, and novel biochemical assays should be developed to predict responsiveness to RDN. Only a high baseline BP has been identified so far as a consistent predictor for treatment responsiveness to RDN. It is important to identify and ensure the completeness of denervation during the procedure itself if possible. In sheep models, pacing the aortic ganglia on each side results in BP increase and ipsilateral renal vasoconstriction, whereas denervation results in abolition of these responses. Peri-procedural nerve stimulation may be used in the future to guide the completeness of RDN and to predict BP response to RDN. Further investigations into potential beneficial effects on several conditions beyond hypertension (glucose/insulin sensitivity, sleep apnea, CKD, diastolic HF, arrythmias) need to be studied. Future devices should include lower profile systems, dedicated catheter devices for transradial procedures and a single device for performing bilateral RDN. Professional society guidelines will be important to avoid RDN overutilization (or underutilization), while focusing on appropriate patient selection, pre-procedural evaluation, strict operator training standards and institutional/facility requirements.1,2,3 Future development of appropriate use criteria for RDN procedures may be needed once the technology matures.
References
- Kandzari DE, Townsend RR, Bakris G, et al. Renal denervation in hypertension patients: Proceedings from an expert consensus roundtable cosponsored by SCAI and NKF. Catheter Cardiovasc Interv. 2021;98(3):416-426. doi: 10.1002/ccd.29884 PMID: 34343406.
- Swaminathan RV, East CA, Feldman DN, et al. SCAI position statement on renal denervation for hypertension: Patient selection, operator competence, training and techniques, and organizational recommendations. JSCAI 2023;2(6):101121. doi: 10.1016/j.jscai.2023.101121
- Barbato E, Azizi M, Schmieder RE, et al. Renal denervation in the management of hypertension in adults. A clinical consensus statement of the ESC Council on Hypertension and the European Association of Percutaneous Cardiovascular Interventions (EAPCI). Eur Heart J. 2023;44(15):1313-1330. doi: 10.1093/eurheartj/ehad054. Erratum in: Eur Heart J. 2023 Jul 14;44(27):2439. PMID: 36790101.
© 2024 HMP Global. All Rights Reserved.
Any views and opinions expressed are those of the author(s) and/or participants and do not necessarily reflect the views, policy, or position of the Journal of Invasive Cardiology or HMP Global, their employees, and affiliates.










