

The Different Mechanisms of Periprocedural Myocardial Infarction and Their Impact on In-Hospital Outcome
Abstract: Background. CK-MB levels exceeding 3 times the upper limit of normal (ULN) following percutaneous coronary intervention (PCI), defining periprocedural myocardial infarction (PMI), are associated with worse outcomes. This study assessed the incidence and mechanisms of PMI and their impact on in-hospital stay. Methods and Results. Over a 12-year period (1996-2007), 272 cases of PMI (overall incidence, 3.5%) were analyzed among 310 consecutive cases of periprocedural myocardial necrosis (PMN; CK-MB > ULN). Mean numbers of treated segments and stents per procedure were 1.87 ± 0.99 and 1.43 ± 1.01, respectively. Mean stent length per procedure was 29.50 ± 19.30 mm. Following analysis of angiogram, procedural data, delay between PCI and necrosis, and mechanisms of PMN were classified as follows: cryptogenic (by exclusion, 41.5%), immediate failure, side-branch occlusion (14.0% each), stent thrombosis (10.6%), prolonged ischemia (9.2%), delayed failure (8.1%), post coronary artery bypass graft (1.5%), and non-target lesion related MI (1.1%). Significantly more stents were used in stent thrombosis, prolonged ischemia during PCI, and cryptogenic cases. In-hospital mortality was 8.1% for PMN and 8.8% for periprocedural MI, decreasing from non-target lesion related MI (25.0%) to mechanisms linked to stent thrombosis (20.7%), immediate failure (17.5%), delayed failure (7.7%), cryptogenic causes (6.1%), and prolonged ischemia (3.4%). Multivariate analysis confirms that in-hospital mortality is influenced by stent thrombosis, age, ejection fraction, and extent of coronary artery disease. Conclusions. The precise mechanism of PMI was determined in about 60% of our series. Stent thrombosis and immediate failure had the poorest in-hospital outcomes.
J INVASIVE CARDIOL 2012(12);24:655-660
Key words: periprocedural myocardial infarction, mechanism of periprocedural MI, in-hospital mortality
____________________________________________________
There are 5 different types of myocardial infarction (MI) based on the pathophysiology and the history of intervention1 according to the universal definition of MI:
- Type 1: MI following a pathological process of the coronary artery wall (plaque erosion, rupture, fissuring, or dissection);
- Type 2: MI following increased oxygen demand or reduced oxygen supply (coronary artery spasm, coronary artery embolism, anemia, arrhythmia, hypertension, or hypotension);
- Type 3: MI following a sudden cardiac death;
- Type 4a: MI associated with percutaneous coronary intervention (PCI);
- Type 4b: MI associated with stent thrombosis documented by angiography or autopsy; and
- Type 5: MI associated with coronary artery bypass graft (CABG).
In the present study on periprocedural myocardial necrosis (PMN), we included MI types 4a, 4b, and 5.
PMN (CK-MB > upper limit of normal [ULN]) is the most common complication after PCI (5%-38%2 and 14%-48%3).The rate of periprocedural MI (PMI), defined as a rise of CK-MB exceeding 3 times the ULN, has been reported to be 17%-18%.4
Various mechanisms implicated in PMI have been described, such as dissection with acute occlusion after PCI, intramural hematoma, perforation, distal embolization, occlusion of one or several lateral branches, complications secondary to stenting such as failure of stent deployment, stent thrombosis, and stent infection.5 In addition to angiography, other investigations such as magnetic resonance imaging (MRI) and intravascular ultrasound (IVUS) may contribute to understanding the various mechanisms of PMI.6
The clinical significance of PMI after PCI remains controversial.5 Increased cardiac enzymes above the upper limits of normal after a PCI (PMN) are associated with a worse long-term prognosis.7,8 The adverse prognostic implications of PMI have been considered similar to the adverse consequences of spontaneous MI.9 Other studies have shown that only large PMIs were predictive of poor long-term outcomes.6,10
The purpose of this retrospective study was to assess the prevalence of the different mechanisms of PMI on the basis of angiography criteria and to measure their impact on in-hospital mortality.
Methods
 Study design and setting. This retrospective medical study took place in a cardiovascular unit where a total of 7700 PCI procedures were performed over a period of 12 years between 1996 and 2007. Patients with a rise of CK-MB above ULN were identified manually by looking through the recorded laboratory values of CK-MB values in Omnipro concerning all patients who had an angiography-PCI reported in the registry (Klinivision) from January 1, 1996 to December 31, 2007. We also retrieved their respective procedural data, stent characteristics, and mortality from the registry. The records of the post-PCI levels of CK-MB and films of all procedures with a rise of CK-MB were retrospectively analyzed to assess necrosis severity and mechanisms. A peak elevation above the ULN of CK-MB at any time after PCI was
Study design and setting. This retrospective medical study took place in a cardiovascular unit where a total of 7700 PCI procedures were performed over a period of 12 years between 1996 and 2007. Patients with a rise of CK-MB above ULN were identified manually by looking through the recorded laboratory values of CK-MB values in Omnipro concerning all patients who had an angiography-PCI reported in the registry (Klinivision) from January 1, 1996 to December 31, 2007. We also retrieved their respective procedural data, stent characteristics, and mortality from the registry. The records of the post-PCI levels of CK-MB and films of all procedures with a rise of CK-MB were retrospectively analyzed to assess necrosis severity and mechanisms. A peak elevation above the ULN of CK-MB at any time after PCI was  considered for the definition of PMN. In our hospital, a blood test for myocardial enzyme levels (CK, CK-MB) and an electrocardiogram (ECG) were systematically performed the day after PCI. CK-MB rises related to acute coronary syndrome before PCI were of course excluded, except in cases of re-infarction.
considered for the definition of PMN. In our hospital, a blood test for myocardial enzyme levels (CK, CK-MB) and an electrocardiogram (ECG) were systematically performed the day after PCI. CK-MB rises related to acute coronary syndrome before PCI were of course excluded, except in cases of re-infarction.
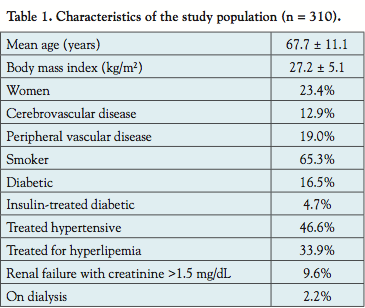
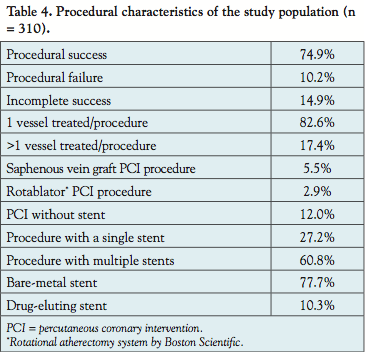
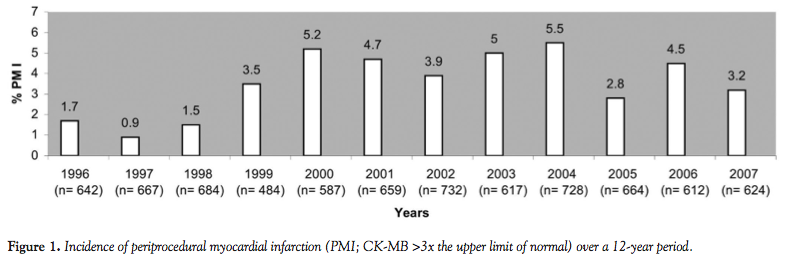
Population and procedural data. A rise of CK-MB above ULN (PMN) was observed in 310 cases. In 272 cases, a CK-MB rise exceeding 3x the normal ULN (PMI) was observed. Figure 1 illustrates the incidence of the PMI over a 12-year period, with an average value of 3.5% per year. The characteristics of the study population (n = 310) are 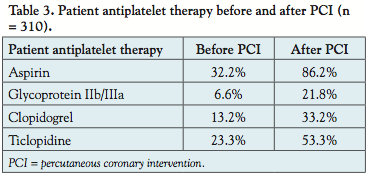 described in Table 1 and the clinical presentation in Table 2. Patient antiplatelet therapy before and after PCI is described in Table 3. The other patient medications before PCI were β-blockers (42.4%), calcium-blockers (17.6%), ACE inhibitors (24.2%), and hypolipemic drugs (27.8%). Procedural data are given in Table 4.
described in Table 1 and the clinical presentation in Table 2. Patient antiplatelet therapy before and after PCI is described in Table 3. The other patient medications before PCI were β-blockers (42.4%), calcium-blockers (17.6%), ACE inhibitors (24.2%), and hypolipemic drugs (27.8%). Procedural data are given in Table 4.
Study protocol. The extent of PMI was classified into 4 categories. By increasing severity order, the first category represented PMI with CK-MB values ranging 3-5x ULN; the second category had CK-MB >5x ULN; the third category concerned MI with Q-wave; and the fourth most serious category was fatal MI, which in our study was represented by 2 cases of death occurring rapidly after the onset of symptoms (hence, without time for a rise in CK-MB, for a Q-wave development on the ECG).
 Each case of PMI was classified as one of the suggested mechanisms based on careful analysis of the angiogram, procedural data, and delay between PCI and the occurrence of PMI: immediate failure, side-branch occlusion, prolonged ischemia during PCI, delayed failure, stent thrombosis, non-target lesion related MI, post CABG, other, and cryptogenic.
Each case of PMI was classified as one of the suggested mechanisms based on careful analysis of the angiogram, procedural data, and delay between PCI and the occurrence of PMI: immediate failure, side-branch occlusion, prolonged ischemia during PCI, delayed failure, stent thrombosis, non-target lesion related MI, post CABG, other, and cryptogenic.
- Immediate failure: PCI procedure with a poor result (procedure failure), without the possibility to improve the angiographic result. For example, an occlusive dissection after PCI and failure of recrossing.
- Side-branch occlusion: the side branch remains occluded with/without attempts to improve the patency.

- Prolonged ischemia: the procedural protocol relates prolonged episodes of ischemia, for example, by an occlusive dissection during the PCI, thrombotic occlusion, or transient no flow frequently seen during procedures on saphenous vein grafts (SVGs) or with rotational atherectomy.
- Delayed failure is a complication after an initially successful procedure. For example, by a delayed occlusive dissection distal to a stent.
- Stent thrombosis: as documented by angiography or autopsy according to the academic research consortium (ARC) definition. Only ‘definite’ and ‘probable’ stent thromboses were considered.
- Non-target lesion related MI: MI (chest pain, ECG, CK-MB rise) in a territory different from the vessel initially treated by PCI.
- Post CABG: by definition, a rise of CK-MB >5x ULN attributed to the CABG performed in an urgent/elective condition.
- Other: one case of hematoma on the left atrial wall.
- Cryptogenic: this diagnosis was frequently considered in the presence of an asymptomatic rise of CK-MB with or without angiographic control. It may represent micro-embolizations.
In cases of several possible mechanisms, we selected the ones associated with the more extensive myocardial injury.
Statistical analysis. Data are expressed as means ± standard deviations. Categorical, ordinal, and numerical variables were compared between groups by chi-square, Cochran, and Kruskal-Wallis tests, respectively. Multivariate influence of variables on in-hospital mortality was studied by logistic regression with backward selection of variables by likelihood ratio test. Odds ratios (ORs) are given with 95% confidence intervals (CIs) in brackets. All tests are two-tailed. A P-value inferior to .05 was considered to be statistically significant. Analysis was performed using SPSS 15.0 software (SPSS Inc).
Results
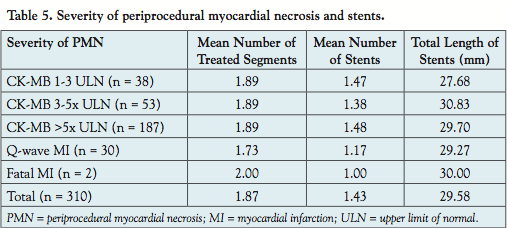 The association between PMN severity, the mean number of treated segments, mean number of stents, and mean total stent length is presented in Table 5. The mean number of treated segments was 1.87 ± 1.00. The mean number of stents per procedure was 1.43 ± 1.01. The mean total stent length was 29.58 ± 19.36 mm. No correlation between PMN severity, mean number of treated segments, mean number of stents, or mean total stent length was observed.
The association between PMN severity, the mean number of treated segments, mean number of stents, and mean total stent length is presented in Table 5. The mean number of treated segments was 1.87 ± 1.00. The mean number of stents per procedure was 1.43 ± 1.01. The mean total stent length was 29.58 ± 19.36 mm. No correlation between PMN severity, mean number of treated segments, mean number of stents, or mean total stent length was observed.
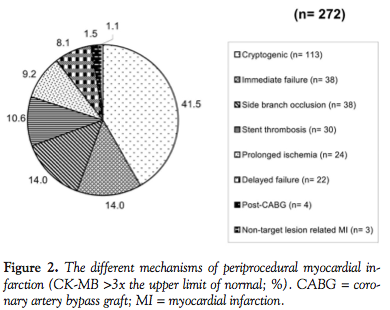 Baseline characteristics of each mechanism cohort (severity, left ventricular ejection fraction [LVEF], localization of the treated segment in the circumflex or anterior interventricular artery or right coronary, extent of coronary artery disease) were studied. Severity (P<.001), localization of the treated segment in the anterior interventricular artery (P=.001), and extent of coronary artery disease (P=.023) are significantly different for each cohort. The distribution of the different mechanisms of PMI (n = 272) is illustrated in Figure 2.
Baseline characteristics of each mechanism cohort (severity, left ventricular ejection fraction [LVEF], localization of the treated segment in the circumflex or anterior interventricular artery or right coronary, extent of coronary artery disease) were studied. Severity (P<.001), localization of the treated segment in the anterior interventricular artery (P=.001), and extent of coronary artery disease (P=.023) are significantly different for each cohort. The distribution of the different mechanisms of PMI (n = 272) is illustrated in Figure 2.
The cryptogenic phenomenon (41.5%; n = 113) is by far the most common factor. Side-branch occlusion and immediate failure accounted for 14.0% each (n = 38), followed by stent thrombosis (10.6%; n= 30), prolonged ischemia (9.2%; n = 24), delayed failure (8.1%; n = 22), post CABG (1.5%; n = 4), and non-target lesion related MI (1.1%; n = 3).
Per class of severity of PMI (n = 272), the most common mechanisms were as follows (Figure 3):

- CK-MB rise between 3-5x ULN (n = 53): the most frequent mechanism was cryptogenic (62.3%) (Figure 3A);
- CK-MB rise >5x ULN (n = 187): the most frequent mechanism was cryptogenic (41.7%) (Figure 3B);
- MI with Q-wave (n = 30): immediate failure (40.0%) and stent thrombosis (26.6%) were the most frequent causes (Figure 3C); and
- Fatal MI (n = 2): stent thrombosis (50.0%) and immediate failure (50.0%), but with only 2 cases these data are difficult to interpret.

Table 6 illustrates PMN mechanisms with the mean numbers of stents and treated segments, and the mean total stent length. PMN mechanisms were significantly related to the mean number of treated segments (P=.049) and to the mean number of stents (P<.001), but not to total stent length.
Among the 310 cases with PMN (CK-MB rise > ULN), in-hospital mortality amounted to 8.1% (25/310 patients). For the 272 analyzed cases with PMI, in-hospital mortality amounted to 8.8% (24/272 patients).
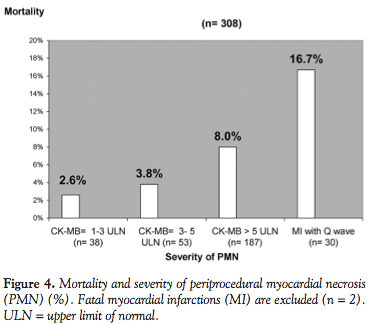 The highly significant correlation between PMN severity and hospital mortality is illustrated in Figure 4 (P=.002). By definition, the 2 cases of fatal MI were excluded (n = 308).
The highly significant correlation between PMN severity and hospital mortality is illustrated in Figure 4 (P=.002). By definition, the 2 cases of fatal MI were excluded (n = 308).
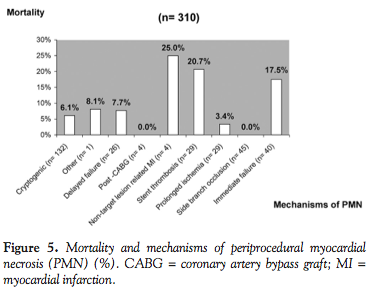
The following mechanisms of PMI were linked to a higher mortality (P=.018): stent thrombosis (20.7%) and immediate failure (17.5%) (Figure 5). There were too few cases of non-target lesion related MI for an interpretation (n = 4).
 According to a univariate analysis, the following variables were associated with in-hospital mortality: PMN severity (P=.025), different mechanisms of PMN (P=.018), LVEF (P=.006), age (P=.002), PCI in the circumflex (P=.020), and extent of coronary artery disease (P=.019). These variables were analyzed by multivariate analysis with respect to in-hospital mortality. The following variables were associated with an increased risk of death: stent thrombosis (P=.022; OR = 3.56 [1.19-10.60]), age (per year) (P=.017; OR = 1.05 [1.01-1.10]), LVEF (per class) (P=.023; OR = 1.50 [1.05-2.13]) and extent of coronary artery disease (single or multivessel disease) (P=.046; OR = 1.76 [1.01-3.09]). PCI on the circumflex was associated with a lower mortality (P=.027; OR = 0.23 [0.06-0.85]). The association between PM severity and in-hospital mortality did not resist to multivariate analysis into the group of 310 cases of PMN.
According to a univariate analysis, the following variables were associated with in-hospital mortality: PMN severity (P=.025), different mechanisms of PMN (P=.018), LVEF (P=.006), age (P=.002), PCI in the circumflex (P=.020), and extent of coronary artery disease (P=.019). These variables were analyzed by multivariate analysis with respect to in-hospital mortality. The following variables were associated with an increased risk of death: stent thrombosis (P=.022; OR = 3.56 [1.19-10.60]), age (per year) (P=.017; OR = 1.05 [1.01-1.10]), LVEF (per class) (P=.023; OR = 1.50 [1.05-2.13]) and extent of coronary artery disease (single or multivessel disease) (P=.046; OR = 1.76 [1.01-3.09]). PCI on the circumflex was associated with a lower mortality (P=.027; OR = 0.23 [0.06-0.85]). The association between PM severity and in-hospital mortality did not resist to multivariate analysis into the group of 310 cases of PMN.
Discussion
The different mechanisms of 272 cases of PMI observed following 7700 PCI procedures were classified based on clinical and angiographic data. In our study, we analyzed the occurrence of the following mechanisms: side-branch occlusion, prolonged ischemia, delayed failure, immediate failure, stent thrombosis, non-target lesion related MI, post-CABG, other, and cryptogenic. Some of these mechanisms have not been reported in the literature, such as prolonged ischemia, delayed failure, non-target lesion related MI, and cryptogenic. The assessment of these mechanisms for analysis of PMI is the main contribution of our study.
In 60% of the cases, we were able to assess the mechanism of PMI. The cryptogenic mechanism proposed for the remaining 40% probably includes a micro-embolization process as suggested by Hanna et al,11 Patti et al,12 or Pasceri et al.13 In native coronary arteries, distal micro-embolizations and occlusions of side branches have been described as the main mechanisms.14 However, all mechanisms implicated in PMI are not necessarily visible by angiography. Micro-embolizations may be assessed by MRI.
In-hospital mortality after PCI amounted to 8.1% for PMN and 8.8% for PMI. The overall hospital mortality after PCI in Belgium is 1.8%.15 Our data confirm that in-hospital mortality is higher in a population with a complication of periprocedural myocardial necrosis (PMN or PMI). In our study, in-hospital mortality was correlated to severity and mechanisms of the necrosis.
Our study confirms that MI with a Q-wave on the ECG is associated with poor in-hospital outcomes, as shown by Stone et al.4 Ioannidis et al16 found that any increase in CK-MB after PCI increased the risk of death. In our univariate analysis, we found the same relationship between severity and mortality, but the relationship did not resist to multivariate analysis. Mortality in cases of CK-MB rise between 1-3x the ULN (2.6%) and CK-MB rise between 3-5x the ULN (3.8%) are a little higher than the overall hospital mortality rate after PCI in Belgium (1.8%). Mortality rates in cases of CK-MB rise >5x the ULN (8.0%) and MI with a Q-wave (16.7%) are in consensus with the literature.4,17
In terms of mechanisms of necrosis, stent thrombosis and immediate failure (procedure failure) were associated in our study with the poorest in-hospital outcomes. According to the multivariate analysis, only stent thrombosis increased in-hospital mortality, although Jeremias et al18 have shown that increased mortality for PMI is confined to patients with unsuccessful procedures. Balaguer-Malfagon et al19 found stent thrombosis to be associated with a 20.7% mortality rate. Stent thrombosis, the only mechanism linked to mortality on multivariate analysis, may represent the main mechanism with a potential to improve outcomes. The incidence of stent thrombosis may be reduced by several factors, such as optimal stent deployment under IVUS, improvement of stent devices, or more antithrombotic medications. Mortality in cases of cryptogenic origin (6.1%) is higher than overall hospital mortality after PCI in Belgium (1.8%), but lower than mortality of stent thrombosis (20.7%).
Our multivariate analysis confirms that heart failure and older age increase the risk of death, in accordance with Ellis et al17 and Jeremias et al.18 In our study, extent of coronary artery disease also influences the in-hospital mortality. The extent of coronary artery disease may induce ventricular dysfunction, known as a main predictor of increased mortality.17.20,21
Previous studies put all CK-MB rises together without separating the cause, prompting the misleading conclusion that all CK-MB rises are harmful.3,9,16,17 We have studied the severity and mechanisms of the necrosis post PCI. Our study shows that mortality is not correlated with severity of the necrosis, but only with stent thrombosis. Kini et al showed that discharge of patients with moderate CK-MB elevation after successful coronary intervention is safe.22 Other parameters, such as heart failure, older age, and extent of coronary artery disease, also influence mortality, showing that we must consider the entire patient.
Study limitations. This study has several limitations. First, the study is retrospective. Second, procedural data between 1996 and 1998 are probably underreported for some patients, which may help explain the PMI incidence gap during the first three years of the study. Third, not all procedural events have been reported, and the authors had to determine the “precise” mechanism of PMN by looking at the angiography and the medical reports. Fourth, cardiac troponins are currently the preferred biomarkers,23 in accordance with the more recent definition of MI. However, given their high sensitivity and the availability of the data, we chose CK-MB markers to select more discriminant necrosis for this 12-year retrospective study. Finally, in some cases, it is difficult to discern whether elevations of CK-MB are due to the PCI or related to the initial acute coronary syndrome.
Conclusion
In this study covering a 12-year period and 7700 PCI procedures, a total of 272 consecutive cases of PMI were analyzed. The mean incidence of PMI was 3.5%. The mechanism of PMN could be identified in 59% of all cases, with the remaining labeled as cryptogenic. A significant correlation was found between the mechanisms of PMN and the mean numbers of stents and treated segments.
In-hospital mortality in case of PMI was markedly increased (8.8%) and was correlated to the severity of necrosis. After multivariate adjustment, stent thrombosis and immediate failure were the only PCI-related mechanisms that were associated with mortality. In multivariate analysis, the only mechanism related to in-hospital outcome was stent thrombosis.
Acknowledgments. The authors wish to express their thanks to all the staff of the cardiology department, in particular the operators, nurses, and laboratory technicians. We are particularly grateful to Prof. Claire de Burbure for revising the manuscript.
References
- Thygesen K, Alpert JS, White HD. Universal definition of myocardial infarction. Joint ESC/ACCF/AHA/WHF task force for the redefinition of myocardial infarction. Eur Heart J. 2007;28(20):2525-2538.
- Herrmann J. Peri-procedural myocardial injury: 2005 update. Eur Heart J. 2005;26(23):2493-2519.
- Califf RM, Abdelmeguid AE, Kuntz RE, et al. Myonecrosis after revascularization procedures. J Am Coll Cardiol. 1998;31(2):241-251.
- Stone GW, Mehran R, Dangas G, Lansky AJ, Kornowski R, Leon MB. Differential impact on survival of electrocardiographic Q-wave versus enzymatic myocardial infarction after percutaneous intervention: a device-specific analysis of 7147 patients. Circulation. 2001;104(6):642-647.
- Carrozza JP, Cutlip D, Levin T. Periprocedural complications of percutaneous coronary intervention. [Computer program]. Up to date; Accessed on May 2010-11-09.
- Prasad A, Herrmann J. Myocardial infarction due to percutaneous coronary intervention. N Engl J Med. 2011;364(5):453-464.
- Andron M, Stables RH, Egred M, et al. Impact of peri-procedural creatine kinase-MB isoenzyme release on long-term mortality in contemporary percutaneous coronary intervention. J Invasive Cardiol. 2008;20(3):108-112.
- Kelly D, Arora R. Prognostic significance of myocardial enzyme release after coronary interventions. Catheter Cardiovasc Interv. 1999;46(3):292-302.
- Akkerhuis KM, Alexander JH, Tardiff BE, et al. Minor myocardial damage and prognosis: are spontaneous and percutaneous coronary intervention-related events different? Circulation. 2002;105(5):554-556.
- Saucedo JF, Mehran R, Dangas G, et al. Long-term clinical events following creatine kinase-myocardial band isoenzyme elevation after successful coronary stenting. J Am Coll Cardiol. 2000;35(5):1134-1141.
- Hanna EB, Hennebry TA. Periprocedural myocardial infarction: review and classification. Clin Cardiol. 2010;33(8):476-483.
- Patti G, Pasceri V, Nusca A, Di Sciascio G. Prevention of peri-procedural myocardial damage in patients undergoing percutaneous coronary intervention. Ital Heart J Suppl. 2005;6(9):553-560.
- Pasceri V, Patti G, Di Sciascio G. Prevention of myocardial damage during coronary intervention. Cardiovasc Hematol Disord Drug Targets. 2006;6(2):77-83.
- Cavallini C, Savonitto S. Prognostic significance of the elevation of the indices of myocardial damage after percutaneous coronary revascularization interventions. Ital Heart J Suppl. 2002 Mar;3(3):270-274.
- Vrijens F, De Gauquier K, Camberlin C. Le volume des interventions chirurgicales et son impact sur le résultat: étude de faisabilité basée sur des données belges. Good Clinical Practice (GCP). Bruxelles: Centre fédéral d’expertise des soins de santé (KCE); 2009. KCE reports 113B (D/2009/10.273/34).
- Ioannidis JP, Karvouni E, Katritsis DG. Mortality risk conferred by small elevations of creatine kinase-MB isoensyme after percutaneous coronary intervention. J Am Coll Cardiol. 2003;42(8):1406-1411.
- Ellis SG, Chew D, Chan A, Whitlow PL, Schneider JP, Topol EJ. Death following creatine kinase-MB elevation after coronary intervention: identification of an early risk period: importance of creatine kinase-MB level, completeness of revascularization, ventricular function, and probable benefit of statin therapy. Circulation. 2002;106(10):1205-1210.
- Jeremias A, Baim Ds, HO KK, et al. Differential mortality risk of postprocedural creatine kinase-MB elevation following successful versus unsuccessful stent procedures. J Am Coll Cardiol. 2004;44(6):1210-1214.
- Balaguer-Malfagon JR, Pomar-Domingo F, Vilar-Herrero J, et al. Stent thrombosis in the modern era: incidence, outcome and predictive factors. Rev Esp Cardiol. 2006;59(8):842-845
- Brener SJ, Lytle BW, Schneider JP, Ellis SG, Topol EJ. Association between CK-MB elevation after percutaneous or surgical revascularization and three-year mortality. J Am Coll Cardiol. 2002;40(11):1961-1967.
- Brener SJ, Ellis SG, Schneider JP, Topol EJ. Frequency and long-term impact of myonecrosis after coronary stenting. Eur Heart J. 2002;23(11):869-876.
- Kini A, Marmur JD, Kini S, et al. Creatine kinase-MB elevation after coronary intervention correlates with diffuse atherosclerosis, and low-to-medium level elevation has a benign clinical course: implications for early discharge after coronary intervention. J Am Coll Cardiol. 1999;34(3):663-671.
- Novack V, Pencina M, Cohen DJ, et al. Troponin criteria for myocardial infarction after percutaneous coronary intervention. Arch Intern Med. 2012;172(6):502-508.
______________________________________________
From the Department of Cardiology, Université catholique de Louvain (UCL), University Hospital of Mont-Godinne, Belgium.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted May 4, 2012, provisional acceptance given May 31, 2012, final version accepted August 6, 2012.
Address for correspondence: Xavier Muschart, MD, Department of Cardiology, Université catholique de Louvain (UCL), University Hospital of Mont-Godinne, Belgium, Av. Gaston Therasse, 15530 Yvoir, Belgium. Email: xavier.muschart@uclouvain.be











