

Abstracts from AIM RADIAL 2012: 1st Advanced International Masterclass
1st Advanced International Masterclass – AIM-RADIAL 2012: Building a Community Spirit to Reach Excellence in Education and Research About Transradial Approach!
Olivier F. Bertrand, MD, PhD on behalf of the Organizers
The number of percutaneous coronary interventions (PCI) continues to grow steadily in the world, especially due to a rapid increase in countries such as Brazil, China and India. Owing to the development of numerous devices and anti-thrombotic treatments, acute and long-term results after PCI have dramatically improved over the last decade. Yet, better recognition of the detrimental impact of bleeding and peri-procedural complications on clinical outcomes have been major drivers renewing interest in the transradial approach. Indeed, although the transradial approach was described more than 2 decades ago, its use during this time has primarily been promoted only by dedicated and most of the time very passionate operators. In the current era of device miniaturization and powerful anti-thrombotic agents, interventional cardiology has reached a state of patient care optimization. In that context, the benefits of the transradial approach for diagnostic angiography and interventions are increasingly being recognized.
A few years ago, a few international academic interventional cardiologists and dedicated radial operators joined their efforts in order to promote research and education in transradial approach. Soon after, the educational website TheRadialist.org was launched. It is an academic initiative to provide information about all aspects related to transradial approach. Since the members of the board come from various regions of the world, they are usually involved in several activities to promote the use of this approach in their countries in all clinical scenarios and all types of coronary and peripheral interventions. Our mission is now to reach at least 50% of radial use within the next 5 years across the world. Challenges, issues and obstacles are different everywhere. We believe that building a large and international community spirit among new and experienced radial operators may ultimately benefit our patients. The transradial approach is very much ‘patient-centric’ so that multidisciplinary efforts between physicians, nurses, cathlab technicians and other health care professionals are required to establish successful transradial programs. Over the years, several transradial courses have been established and have remained successful. For most of them, the content consists in either a ‘top to bottom’ teaching where beginners listen to lectures given by advanced transradial operators over 1 to 2 days, or they are based on live demos with emphasis on tips and tricks. Because the transradial approach has become fashionable, major cardiology congresses nowadays include 1 or 2 dedicated sessions to discuss specific aspects of transradial approach. Yet, we felt that there was a need for a dedicated forum where radial operators could discuss current challenges, present new results, agree on common nomenclature and interact with industry to develop radial specific devices. This is the goal of the AIM-RADIAL congress. The 1st edition of AIM-RADIAL coincides with the 20th anniversary of the first transradial PCI performed by Dr F Kiemeneij and Dr GJ Laarman in The Netherlands. In this issue of the Journal of Invasive Cardiology, you will find peer-reviewed abstracts selected for presentation during the congress as well as a few short summaries about interventional cardiology and transradial approach in a few selected countries. We hope that you will enjoy the reading of these proceedings and that you will be interested in attending a future AIM-RADIAL congress! Publication of these proceedings has been made possible through educational grants from TERUMO-US and the Faculty of Medicine of Laval University.
Coronary Interventional Cardiology and Transradial Approach in France
Yves Louvard1, Thierry Lefevre1, Hakim Benamer1, Jacques Monsegu2, Benjamin Faurie3.
1ICPS, Massy, 2Hopital des armées, Val de Grâce, Paris, 3Clinique mutualiste, Grenoble, France
Cardiovascular risk in France. Among developed countries, the risk of coronary artery disease is three times lower in France compared to northern European countries such as the UK (Scotland) and Finland (Karelia), 30% lower than in Belgium or Germany, and this north-east to south gradient is even visible inside the country (MONICA study).
Organization of interventional cardiology in France. Most data on coronary interventional cardiology activity in this paper have been provided by the GACI (Groupe Atherome et Cardiologie Interventionnelle, Atheroma and Interventional Cardiology Group of the French Society of cardiology). The board of this group, which represents French interventional cardiologists, is composed of one president, one past president, 3 cardiologists from public hospitals (university or community hospital), 3 private-practice cardiologists and 1 representative of young operators. This board is elected every 2 years, the president is alternately a private or a public operator. This group comprises 1200 members. The missions of this group include the organization of monthly meetings for discussion of professional topics, scientific themes, multicenter scientific studies, evaluation and production of documents regarding new technologies and drugs for authorities (reimbursement), and international meetings.
Coronary interventional cardiology activity. There are 204 interventional cardiology centers in France (250 cathlabs, 62 million inhabitants), 90 private, 114 public, with a mean operator number of 3. The Paris region accounts for 16% of centers (19% of the total population). The number of coronary angiographies was 131,000 in 1991, rose to 272,000 in 2006 and decreased to 253,000 in 2009 (55% public). PCIs numbered 30,000 in 1991, rose to 121,000 in 2006 and then decreased by 6% in 2009 (55% public). The PCI/angiography ratio has been stable (43-45%) since 2002. In 2003, 132,000 stents were implanted, 192,000 in 2006, and decreased to 185,000 in 2009, the number of stent per patients has been stable, 1.6, since 2006, the percentage of DES, 50% in Q1-2006 went down to 40% in Q4-2007 and increased to 52% in Q4-2009.
Interventional cardiologist training. In France, the duration of medical studies is 6 years, specialization takes 3-5 years (fellowship) and interventional cardiology 2 years (can be partially parallel to specialization). There are three well defined, recognized specializations in interventional cardiology: pediatric, adult, and rhythmology and cardiac stimulation. Specialists in interventional cardiology receive an inter-university diploma. It is obtained only after 70 hours of theoretical coursework, an annual workshop, a dissertation and a fellowship report including all cases performed, all assessed by a jury, and of course a practical fellowship. The practical fellowship training period spreads over two levels, level one (one year) is dedicated to coronary angiography and catheterization (500 cases, 250 as first operator), the second is for PCI (300, 150 as first operator) in a teaching center, private or public (>600 PCI/year). The interventional cardiology DIU has a half public /half private steering committee, elected for 2 years, the director being a university professor and a vice director a private operator.
The training program includes a mandatory degree in radioprotection. The annual need for new interventional cardiologists in France is evaluated to be around 20.
Legal aspects of interventional cardiology practice. Interventional cardiology in France is submitted to legal authorization. A minimal volume of procedures per operator is required (200 angios and 100 PCI as first operator/year). A center performs at least 350 PCIs a year. Day and night, the PCI team is composed of 2 MDs (1 interventional cardiologist) and 2 paramedics (nurse or X-Ray technician). Opening (24-hour availability) for emergency (24 hours a day) and an intensive care unit are mandatory.
Transradial approach for PCI. The transradial approach for coronary interventional cardiology started to be implemented in France in early 1994 (1.5 years after Kiemeneij-Laarman in Amsterdam). In March 1994, the first transradial PCI live case transmission ever performed was carried out from Toulouse and transmitted to the TCT meeting in Washington (Jean Fajadet). This had a big impact in France. Over the following years informal workshops in Toulouse and an annual course in Massy (1997-2006) or Paris (RITA, 2008-ongoing) resulted in an increase in the percentage of radial procedures for PCI in France to 20% in 2001, more than 40% in 2004, 60% in 2006 and probably more than 80% in 2012 (less for angiography).
The natural complement to the transradial approach for PCI, namely, outpatient angioplasty, is performed in small numbers only in a few public centers (Pitié-Salpêtrière and Henri Mondor hospitals in Paris …)(no payment of equipment and nursing costs in private centers).
Conclusion: Interventionists in France were the most avid students of Lucien Campeau and Ferdinand Kiemeneij for many years and led to the biggest absolute number of transradial approaches in the world for coronary diagnosis and treatment, but over the past 3-4 years China (with a big percentage) and even the US (despite a low percentage) have certainly been performing a larger number of transradial procedures.
Transradial Intervention in Japan
Yuji Ikari, MD, PhD
Professor, Department of Cardiology
Tokai University, Japan
The health insurance system in Japan is universal. All the Japanese people must be members of the governmental health insurance and all medical treatments are covered. No doctor can perform a treatment not covered by insurance, but if a special exception is needed for an uncovered treatment, the insurance will not pay any part of the covered treatment. Thus, the patient must pay 100%. Therefore, uncovered treatment is extremely difficult to perform. Patients have to pay 30% of the total cost. If the maximum payment is over the limited amount according to the annual income, the exceeded payment is covered by the insurance. For example, a family with average income would pay no more than 100,000 yen annually even though some of the family members may undergo extremely expensive surgery.
In the cath lab, an intravascular ultrasound is covered by the insurance. One stent and one balloon are covered for a lesion. When three lesions are found, three stents and three balloons are covered. Because PCI is covered, many institutions will perform PCI. Probably, more than 1000 cath labs exist in Japan, both private and public hospitals and both academic and non-academic hospitals exist. There are 200,000 PCIs performed annually in Japan. To become an interventional cardiologist, there is no definite educational course in Japan. For example, a fellow starts cardiology training after 2 years as a resident and learns non-invasive and invasive cardiology. During the 3-year fellowship, a fellow might decide to become an interventional cardiologist. After 300 diagnostic cases, they start PCI. They can apply for fellowship of the Japanese Association of Cardiovascular Intervention and Therapeutics after completion of 200 PCI procedures.
Transradial Intervention (TRI) is widely applied in Japan because Dr. Shigeru Saito has actively trained many doctors. Currently, the Slender Club Japan followed Dr. Saito and pursued the advanced slender TRI using 5 Fr or 4 Fr guiding catheters. Even though same day discharge after diagnostic catheterization is possible, it is not widely applied in Japan because the health insurance pays a higher cost to the hospital when the patient stays in the hospital.
Transradial approach is also applied in peripheral interventions. Renal intervention is easier using TRI. Iliac intervention is also performed using TRI. However, SFA or BK is difficult because of the limited catheter length. Recently, carotid stenting is also being performed using TRI.
Interventional Cardiology and the Transradial Approach in Israel
David Meerkin, MBBS
Shaare Zedek Medical Center, Jerusalem, Israel
Israel is a small country geographically but has seen a massive population increase over the last 50 years with the immigration of many people from a wide range of very different countries and cultures. The development of the health system to accommodate this ever-changing population and to provide top level care to the broadest spectrum of the community has been a challenge met with surprising success over the last few decades. The vast majority of the over 20,000 annual PCIs take place within the public hospital system in university affiliated hospitals, although within the center of the country two private hospitals have busy cath facilities. Almost all public hospitals offer PCI in a concerted effort to offer primary PCI to the entire populace within short access times.
Training in cardiology requires a four year post internship residency in internal medicine followed by a further three years of cardiology fellowship which should include a 6-month rotation in intervention. In Israel subspecialties of cardiology are not recognized or required and as such there are limited opportunities for interventional cardiology fellowship programs in the country. Today, almost all aspiring interventional cardiologists will spend at least two further years in an recognized program overseas, mostly in North America. The amount of transradial exposure and training is extremely variable due to the variability of the training programs.
In 1995, several years after the initial report of the transradial approach, the first Israeli report of this technique was published. The approach remained dormant until the late 90s and 2000 when physicians from three centers adopted the technique as the default approach to coronary catheterization. It remained an esoteric approach until 2006 when the first Israeli Transradial Workshop took place in Jerusalem. This provided a primer of current techniques, equipment and potentials to the attendees who represented most of the Israeli hospitals. This proved to be a turning point and over the next five years the penetration of this technique began to escalate, supported by the return of some younger cardiologists from interventional training, predominantly in Canada. This was manifest at the Second Israeli Transradial Workshop held in 2011. Now almost all hospitals are active transradial centers with an ever broadening range of experience, including not only the application as the default for primary PCI, but also for peripheral vascular procedures such as carotid stenting, renal stenting and treatment of supraaortic vessels.
Currently it is an approach offered by almost all hospitals and many physicians offer it as the default approach. This was manifest in the ACSIS registry of Israeli ACS patients where 36% of ACS patients were treated by the transradial route.
Use of the Radial Approach for Coronary Procedures in Greece
A. Ziakas, G. Papaioanou, K. Toutouzas, G. Bompotis, A.D. Mavrogianni, L. Lillis, I. Syliadis.
From the 1st Department of Cardiology, AHEPA University Hospital, Thessaloniki, Greece.
Greece has a population of about 11 million people, with almost half of them living in Attica, the largest of the country’s 13 administrative regions which includes Athens, the capital city of Greece. Another 1.9 million people live in Thessaloniki Metro area, Greece’s second most populated region. There are currently 49 cath labs operating in Greece, 30 (61%) of which are public (9 academic-18%). Academic hospitals are only public in Greece. The majority (31-63%) of the cath labs are located in the Athens Metro area, which has a population of about 4.1 million people. Nineteen of these labs are public (3 academic) and 12 belong to the private sector. Eight (16%) cath labs are located in Thessaloniki Metro area; 4 of these are public (1 academic) and 4 are private. The remaining 10 (20%) labs are scattered across the other regions of Greece; 7 of them are public (5 academic) and 3 private.
A total of 44,920 coronary angiograms and/or other coronary procedures and 16,508 PCI procedures are performed each year in Greece (data from 2010). The total number of both coronary and PCI procedures tends to decrease in Athens and Thessaloniki Metro area compared to previous years’ data. However, in the remaining administrative regions the total number of procedures has increased during the past years (2007-2010 data). This shows a certain decentralization tendency, with regional cath labs becoming more functional and organized and thus performing more procedures.
In order to become specialist cardiologists in Greece, doctors undergo two years training in Internal Medicine and four years in cardiology. All cardiology interns receive a mandatory 6-month cath lab training during this 6-year internship. However, there is no official or State-recognized training in order to become an interventional cardiologist after the internship. For this reason, most Greek interventional cardiologists get trained abroad, usually in well-recognized and experienced centers. Some cardiologists start working in public hospitals as specialist clinical cardiologists and get further but not official training in interventional cardiology in order to become interventionists. It is interesting though, that in order to perform interventional cardiology procedures in Greece, it is not mandatory to get further training apart this 6 month period during the internship.
The radial approach has been used by Greek interventional cardiologists for more than a decade and it has been gaining ground since then. More interventional cardiologists are trained in the technique and more start using it in everyday practice, offering their patients a lower complication rate and a shorter hospitalization period. However, the vast majority of procedures are still performed using the femoral access. According to the Hellenic PCI Registry, radial access is only used in 3.2% of all PCI procedures. This number is steadily increasing year after year especially in certain regions. It is interesting that in Thessaloniki Metro area the radial approach is now used in almost 40% of the cases, whereas five years ago the percentage of radial procedures was about 10%.
Regarding time of discharge after transradial coronary procedures, the majority of patients undergoing transradial coronary angiography are discharged the same day of the procedure, usually within 4 to 6 hours. Same-day discharge is not used after transradial PCI at the moment because there is no reimbursement from the National Health System. Carotid and iliac procedures are performed only by vascular surgeons in Greece, and their use of the radial approach is rare. In conclusion, the radial approach is now used in a minority of the coronary procedures in Greece, but its use is gradually gaining ground, especially in certain regions.
Interventional Cardiology and Radial Approach in Canada
Olivier F. Bertrand, MD, PhD1, Erick Schampaert, MD2, Vlad Dzavik, MD3
1Quebec heart-Lung Institute, Quebec City, Quebec, 2Hôpital du Sacré-Coeur, Montreal, Quebec, 3Peter Munk Cardiac Centre, University Health Network, Toronto, Ontario, Canada.
In 2006, the Canadian population estimate was about 32 million. However, despite its very large geographical area, 25 million of Canadian citizens reside in just a few cities, including Toronto, Montreal, Vancouver, Ottawa, Calgary and Edmonton. To cover these territories, there are only 44 cardiac catheterization and percutaneous coronary (PCI) laboratories.
The number of PCIs varies between 55,000 and 60,000 per year. Although a national PCI registry does not exist, PCI databases have been established in British Columbia, Alberta, Ontario and Newfoundland. Since PCI activity takes place in a limited number of sites, interventional cardiologists in Canada are high-volume operators with an average of 280/PCI/operator/year. It should also be noted that the rate of PCI is 3-10 times higher in the provinces of Quebec and Ontario compared to the 7 other provinces. Most centers are affiliated with universities and there are no private PCI centers in the country. The majority of these centers include cardiac surgery programs. Stand alone diagnostic cardiac catheterization laboratories are disappearing.
In 1989, the first case of cardiac catheterization via the transradial approach in the world was performed by Dr. Lucien Campeau at the Montreal Heart Institute, but his example was not followed by his peers. The initial transradial PCI cases were performed in the early nineties by Dr Dave Hilton at Royal Jubilee Hospital in Victoria and Dr Gérald Barbeau at Quebec Heart-Lung Institute in Quebec soon after the description by Drs Ferdinand Kiemeneij and Geert Jan Laarman in The Netherlands. As in many other countries, the radial approach was adopted in Canada early on by a few aficionados but remained ignored by the large majority of the interventional cardiology community. Although the Canadian Cardiovascular Society (CCS) had been in place for a long time, the Canadian Association of Interventional Cardiologists, an official affiliate of CCS, was only founded in 1990. Today its activities remain centered on educational working groups, the standards of training and competency, focused statements and guidelines, and collaboration with other national societies like the Society of Cardiac Angiography and Interventions (SCAI) in the US.
Training in cardiology is encompassed within a 3-year program following 3 years of core training in internal medicine. During this basic training, residents spend 3 months in cardiac catheterization laboratories. To become interventional cardiologists, residents will add another two years in an interventional cardiology training program.
At this stage, there are no formal recommendations for training in the radial approach, although some residents and trainees may be exposed very early on depending on the institution. In fact, in some institutions where the default access is the radial approach, it is possible that residents get insufficient experience in femoral access puncture and management. Although it is difficult in Canada to estimate the rate of use of the radial approach, estimates from industry sources in 2011-12 suggest a mean use of 50% across the country, with >70-80% in the province of Quebec and < 50% in some other provinces. A CAIC radial approach working group was officially created in 2011. The objective of this working group is to further promote research and education in the transradial approach for diagnostic angiography and interventions. AIM-RADIAL 2012 is one of the first educational activities of the CAIC radial working group.
Interventional Cardiology and Radial Approach in Italy
Enrico Romagnoli, MD, PhD1-2, Francesco Burzotta, MD, PhD3, Marco Valgimigli MD, PhD4, Alessandro Sciahbasi MD5, Fabio Tarantino MD6, Mario Galli, MD7, Cosimo Sacra, MD8, Mauro De Benedictis MD9, Orazio Valsecchi MD10, Carlo Trani MD3
From the 1Policlinico Casilino, Rome, Italy; 2SS. Filippo e Nicola Hospital, Avezzano; Italy; 3Università Cattolica Del Sacro Cuore, Rome, Italy; 4University Hospital of Ferrara, Ferrara, Italy; 5Sandro Pertini Hospital, Rome, Italy; 6Morgagni-Pierantoni Hospital, Forlì, Italy; 7Sant’Anna hospital, Como, Italy; 8Panico Hospital, Lecce, Italy; 9Azienda Ospedaliera Ordine Mauriziano di Torino, Torino, Italy; 10Ospedali Riuniti di Bergamo, Bergamo, Italy.
The Italian Population is estimated to be about 60 million and it has been stable during the last decade. Demographic distribution is quite homogenous in the 20 political districts with very few cities having a citizen number greater than 2 million. In Italy we have a total of 266 private and public catheterization laboratories joining the Italian Society of invasive Cardiology (SICI-GISE) founded in 1973. Aims of this society are the promotion of educational working groups, the development of national statements and guidelines, and the organization of the annual national meeting of interventional cardiology. SICI-GISE also promotes cultural exchange among laboratories and sponsor multicenter clinical studies. Details regarding the activities of the SICI-GISE can be found in the official website (www.gise.it). One of the most important activities of this organization is related to the collection of annual catheterization laboratory activities (diagnostic, interventional procedures, type of procedures, technical details of the procedure performed, etc.). The collected data may be consulted at the SICI-GISE website. According to this official registry, all Italian centers are performing both diagnostic and interventional procedures for a total of 275,216 and 139,263 in the 2011, respectively.
Albeit several operators use radial approach since the late eighties, only recently has the radial approach seen a widespread diffusion in Italy. Of note, during the past years, Italian interventional cardiologists practicing radial approach have founded the Italian Radialforce which recently evolved into the Italian Radial Club. This growing group of interventional cardiologists worked hard to spread the radial basic techniques and the scientific rationale favoring radial approach widely in Italy through a series of initiatives.
From its use as valid alternative to standard femoral approach in selected patients, now the radial approach is routinely utilized as the first choice in many centers. In 2010, after repeated solicitations from Italian radial operators, the SICI-GISE inserted the approach adopted for coronary procedures in the dataset of the official GISE registry of cath labs’ activity. Thus, we now know that the percentage of transradial procedures in Italy was 36% in the 2010 and increased to 46% in the 2011. The interest in the transradial approach is also evident by the current insertion of specific sessions focused on understanding issues of radial approach in the main interventional national meetings.
Regarding the interventional cardiology formation process in Italy, training in cardiology is organized in a 4-year residency program following medical degree. Access to the cardiac catheterization laboratory during this period is not standardized and there is no specific training program to become an interventional cardiologist. To overcome this deficiency the GISE has recently introduced the GISE Fellow graduation identifying the minimum requirements and the needed training program to become a certified interventional cardiologist. Any cardiologist can apply the GISE Fellow nomination if he or she has five years of experience in any of certified cath labs and has performed more than 1000 procedures as first operator. At this stage, there are no official GISE recommendations for training in the radial approach, and radial experience of residents and trainees depends on current practice of several institutions.
Current Experience with Radial in the United States
Ian C. Gilchrist, MD, Penn State Hershey Medical Center, Hershey, PA; Mauricio G. Cohen, MD, University of Miami Miller School of Medicine, Miami, FL; J. Tift Mann III, MD, Wake Heart Associates, Raleigh, NC; Samir B. Pancholy, MD, The Commonwealth Medical College, Scranton, PA; Christopher T. Pyne, MD, Lahey Clinic, Heart & Vascular Center, Burlington, MA; Sunil V Rao, MD, Duke University Medical Center, Durham, NC
All authors read and contributed to the final manuscript
The early radial experience in the United States (US) mirrored that of other countries after the promising reports in the 1990’s of transradial success with individual operators either self-learning or developing skills from direct contact with other transradial operators. Contrary to many of the non-US regions, transradial did not subsequently expand in the US. Rather, it subsisted as a niche technique supported by a small group of enthusiastic operators who were often marginalized by leaders in the US interventional community. While the suppression of innovation at first glance appears odd for cardiologists who by nature otherwise embrace new technology, there was a competing technology, vascular closure devices, that enamored practicing US cardiologists during this time. Within the last few years there has been a tectonic shift in US practice with an increased interest in transradial techniques that first manifested itself in 2009-2010 with standing-room-only crowds appearing for transradial sessions at TCT, AHA and ACC meetings. At present, the US appears to be on the early logarithmic rise in radial adoption although its uptake is regionally diverse with some areas of the eastern US with a 20-30% penetration while the western US remains below 10%.
The US healthcare system is confusing in that it is not really a system at all but rather thousands of independent providers of healthcare such as doctors and hospitals, and a few dominant payers who foot the bill. Within this system, hospitals have evolved as independent entities and at times compete across streets for the same patient population and for the attention of physicians who can admit patients to these facilities. This results in autonomy for physician practice patterns and makes it difficult to control or manage physician behavior without financial rewards or penalties.
Hospital types include government-owned facilities such as the Veterans Administration (VA) hospitals that cover former military service personnel or military hospitals for active duty servicemen, and local municipal or county hospitals that often treat with little regard for the ability of the patient to pay. There are also not-for-profit hospitals run by a variety of charitable organizations such as religious or other service-minded groups along with university affiliated academic medical centers. Finally, there are for-profit hospitals that range in size from single, physician investor owned facilities to large publicly traded corporations, such as Hospital Corporation of American (HCA), Inc., that are in the business of healthcare.
While the US does not have a national healthcare system, most of the reimbursement for healthcare is driven by policy set by the Medicare system that is run by the federal government. It provides coverage to people over the age of 65 years and is funded by taxpayer dollars. Medicare reimbursement has been driven by a Diagnosis Related Group (DRG) system where reimbursement for a certain diagnosis is uniform across hospitals with only minor variations to account for different hospital cost structures, presence of a training program, or severity of the patient’s illness. Over the last few years, the Medicare system has also evolved its reimbursement for cardiac catheterization and now these procedures are considered outpatient procedures. In other words, hospitals receive a single payment for cardiac catheterization and PCI regardless of whether patients are sent home after a few hours or kept overnight in outpatient recovery units. To encourage the appropriate use of outpatient billing practices and discourage gaming the system to receive (higher) inpatient reimbursement, there is an ongoing audit of hospitals that receive Medicare payments. These are known as Recovery Audit Contractor (RAC) audits, which ostensibly insure compliance with correct billing practices by levying significant fines and penalties for lack of compliance. This shift in reimbursement has occurred as transradial started to gain traction in the US and may be partially responsible for renewed interest.
For those patients not covered by Medicare, such as those who are actively employed, private healthcare insurance companies provide coverage. Their policies often mimic those of Medicare although the actual amounts of payment may vary depending on local situations. Both Medicare and private insurance carriers tend to pay the bulk of the hospital bill, but there are a tremendous variety of co-payments that might apply depending on the individual payer. While healthcare insurance covers most hospital costs, this does not extend to pharmaceutical costs after discharge, and many patients are left with little insurance help in paying prescription costs.
There are about 2000 cardiac catheterization sites in the United States doing about 3.75 million patient procedures per year including about 600,000 PCIs. The individual volume in these cath labs is variable as often there has been no central planning in the need for any one facility. A recent calculation estimated that 60% of US interventional cardiologists do <40 PCIs per year. The reservoir of low volume operators does present a challenge when new techniques such as transradial are introduced and dissemination is attempted.
US cardiologists performing catheterization procedures may or may not have had formal training in interventional cardiology depending on their age. Recent graduates would be expected to have completed a minimum of a 3-year cardiology fellowship after completing a 3-year Internal Medicine residency program. In addition, to become certified by the American Board of Internal Medicine in Interventional Cardiology, one needs to complete a further year of Interventional Fellowship. Despite these requirements for certification, there are actually no legal/regulatory requirements and compliance is voluntary. Moreover, payers usually don’t stipulate the experience of operators.
Transradial techniques are presently introduced to cardiology fellows early in their training, typically in parallel with transfemoral techniques, in those programs where transradial skills exist. There are a variety of well-known US programs that still do not have transradial skills in their faculty and those fellows do not learn the techniques. The Society of Cardiac Angiography and Intervention (SCAI) recently published some guidelines on transradial techniques and recent fellowship graduates have found market value in transradial skills that will further encourage learning in the fellowship years. Identifying the best approach to train practicing physicians continues to be a challenge. Corporate sponsorship by a few long time supporters of transradial such as the Terumo Corporation, and more recently organized training by the SCAI, have helped bridge the educational gap in the United States. Unfortunately, most of the corporate world has not supported this technology and funding has been limited. Compounding the problem has been a recent trend to vilify industry money used for training even though other sources to support such activities are not readily available at most institutions.
While the US healthcare system has not adopted trans-radial with the same enthusiasm seen in other countries, the tide has shifted. The decade-long infatuation with closure devices has produced very little evidence of advantage and clearly has demonstrated some interesting complications and well-documented costs. Venture capital is no longer investing large sums of capital into these companies and the distraction of these devices is waning. There has been a push to consider optimizing the patient care process and now reimbursement policies are aligned to encourage early discharge. Likewise there has been a renewed interest in avoiding complications such as vascular bleeding to the point of discussing withholding payment to hospitals for such events. These trends have all added to the attraction of a transradial approach. The Internet and patient knowledge combined with competitive physician practices have also brought transradial skills into the marketplace as a differentiating skill for practices and driving interest in transradial training. These are but some of the recent changes and shifts in the US market that have resulted in the better late than never shift in interest in transradial for this large healthcare market. Whether or not the US will show a shift to the extent seen in other countries is a point of debate, but for the moment there is a definite upward trend in transradial adoption.
Coronary Interventions in the Czech Republic and Trends in the Use of Radial Approach
I. Bernat1, M. Zelizko2, J. Vojacek3, P. Widimsky4, J. Stasek3, M. Mates5, M. Branny6, L. Pesl7, R. Fialka8, J. Jarkovsky9, P. Kala10 on behalf of the NRKI investigators
1University Hospital and Faculty of Medicine Pilsen, Czech Republic; 2IKEM, Prague, Czech Republic; 3University Hospital Hradec Kralove, Hradec Kralove, Czech Republic; 4Third Faculty of Medicine, Charles University and University Hospital Kralovske Vinohrady, Prague, Czech Republic; 5Hospital Homolka, Prague, Czech Republic; 6Hospital Trinec a.s., Trinec, Czech Republic; 7Hospital Ceske Budejovice, a.s., Ceske Budejovice, Czech Republic; 8KSRZIS, Ministry of Health of the Czech Republic, Prague, Czech Republic; 9Institute of Biostatistics and Analyses, Masaryk University, Brno, Czech Republic; 10Medical Faculty of Masaryk University and University Hospital Brno, Czech Republic.
I.Bernat and P. Kala declare the same contribution on the publication.
Abstract. The article describes the development of the coronary interventional program in the Czech Republic. Primary percutaneous coronary intervention (PCI) has been used in the vast majority of patients with ST-elevation acute myocardial infarction (STEMI) during the last 10 years. Analysis of the Czech National PCI Registry (NRKI) was used to demonstrate the trends in the use of radial approach.
PCI program in the Czech Republic. Czech coronary interventions have a 30 year history. In 1982 there was the first elective PCI performed in IKEM, Prague and the first catheter-based intervention for acute STEMI (intracoronary thrombolysis) in two other hospitals (University Hospital Brno and University Hospital Kralovske Vinohrady in Prague). The modern history of the PCI program in the Czech Republic started after communism fell in 1989. There are several milestones observed: first, several new cathlabs were opened during the nineties; second, the well-known PRAGUE and PRAGUE-2 trials established primary PCI as the treatment of choice for patients with ST-elevation myocardial infarction (STEMI)1,2; and third, the Czech National Cardiovascular Programme was accepted by the national authorities as the guideline for acute cardiac care in the whole country. This was associated with several other cathlabs opening which finally covered the whole Czech territory in an optimal manner (one PCI hospital serving the mean population of 500,000). Every new cathlab had to prove three full-time contracts for licenced interventional cardiologists to receive the reimbursement from the health care payers. Furthermore, 24/7 acute interventional treatment of all STEMIs had to start within the 3-month period after the cathlab opening. Of course to become an interventional cardiologist in the early 90s was very different from current practice. In 1997 the Czech Society of Cardiology along with the Czech Medical Chamber developed the new postgraduate system introducing so called “functional licenses” for diagnostic and interventional cardiology, a system that remains in place today. At present, to receive an “interventional license,” physicians specialized in cardiology have to perform 400 diagnostic catheterizations and 100 PCIs during a 1-year training program in the cardiac center accredited by the Ministry of Health of the Czech Republic.
Currently there are 22 PCI hospitals in the Czech Republic, most of them are public (19 centers) and all of them provide the 24/7 service. This means that since 2002 the rate of thrombolysis among all hospitalized STEMI patients is below 1% and the number of primary PCIs for STEMI exceeded 600/million during the last 10 years and still represents almost one third of all PCIs. Together with the Netherlands and Sweden, the Czech Republic was appreciated as one of the best nationwide examples of AMI care on the international level which system was applied in the European “Stent for Life” Initiative.3-5
Czech National PCI Registry (NRKI). In 2005 the Czech National PCI Registry (NRKI) started to collect the data from all PCI procedures from all cathlabs. This can be seen as another milestone of interventional cardiology development in the Czech Republic. Since that time all consecutive patients and procedures are independently followed by the Ministry of Health of the Czech Republic in term of all-cause mortality as the hardest clinical endpoint.
Access route to PCI. The access site to PCI is one of the important parameters that has been followed in the NRKI. Regarding the use of different arterial approaches to PCI, recent analysis of the NRKI data of 120,099 PCIs performed from January 2005 to June 2011 clearly demonstrate the increasing use of transradial access (TRA). In 2005, the femoral artery was the preferred access to the vast majority of PCIs; however, by 2011 the radial access reached half of all PCI procedures. This has been a dramatic change of the access route during the last 6 years that has been reflecting the lower vascular complication rate after TRA together with lower cost and improvement of patient comfort with some potential to improve the outcome of patients requiring acute PCI.
The use of TRA (28,319 PCI procedures) and transfemoral approach (TFA) (91,780 PCI procedures) was evaluated and compared from the Czech PCI centers for each year and overall. Other approaches with complete data in this registry (320 PCI procedures) were not included in this analysis.
The use of transradial PCI increased significantly every year - from 5.6% in 2005 to 49.3% in 2011. This trend was evident both in acute and non-acute patients. (Figure 1) Also the percentage of TRA procedures in each PCI center has changed. While in 2005 only one center used TRA in more than 20% of PCIs, in 2011 more than half centers used it in >60% of procedures and one third in >80% (Figure 2). Transradial coronary interventions were associated with a similar rate of procedural success (93.3% vs. 92.3%; p<0.001).
Perspectives of coronary interventions in the Czech Republic. In 2005 the number of PCI in the Czech Republic reached its maximum and since that time we are in the “plateau” phase. The whole Czech population is covered by both the acute and elective PCI program and this is an excellent “quantity” base for further improvements in quality. One of the steps forward is the “ACT NOW. SAVE A LIFE” public campaign as part of the Stent for Life Initiative that is currently starting. Besides that there is a need for implementation the new pharmacoinvasive protocols, concept of functional revascularization, the use of special interventional and imaging techniques, further improvements in the time-to-treatment time intervals and high-quality research. Another quality oriented topic is the use of TRA to PCI partly discussed in this article. The TRA PCI has increased almost tenfold during the last six years and this trend was observed nationwide, i.e. in all PCI centers. Based on these results it is realistic to suppose that TRA will become the first choice to PCI in a majority of cases in near future.
Nevertheless the main perspective remains the same – the patient being at the center of our interest.
Acknowledgement: The authors thank the Ministry of Health of the Czech Republic, Working Group of Interventional Cardiology of the Czech Society of Cardiology and especially all the participating centers for their continuous support and huge enthusiasm.
References
- Widimský P, Groch L, Zelízko M, et al. Multicentre randomized trial comparing transport to primary angioplasty vs immediate thrombolysis vs combined strategy for patients with acute myocardial infarction presenting to a community hospital without a catheterization laboratory. The PRAGUE study. Eur Heart J 2000;21:823-831.
- Widimsky P, Budesınsky T, Vorac D, et al. Long distance transport for primary angioplasty vs. immediate thrombolysis in acute myocardial infarction. Final results of the randomized national multicentre trial - PRAGUE-2. Eur Heart J 2003;24:94–104.
- Knot J, Widimsky P, Wijns W et al. How to set up an effective national primary angioplasty network: lessons learned from five European countries. EuroIntervention 2009(3):299,301-309.
- Widimsky P, Wijns W, Fajadet J, et al. on behalf of the European Association for Percutaneous Cardiovascular Interventions. Reperfusion therapy for ST elevation acute myocardial infarction in Europe: description of the current situation in 30 countries. Eur Heart J 2010; 31:943-957.
- Kristensen SD, Fajadet J, Di Mario C, et al. Implementation of primary angioplasty in Europe: stent for life initiative progress report. Eurointervention 2012;8:35-42.
Transradial Intervention in the United Kingdom
K. Ratib, MD, Jim Nolan, MD
University Hospital of North Staffordshire, Staffordshire, UK
The National Health Service (NHS) was set up in 1948 with the aim of providing free healthcare at the point of delivery to all residents of the United Kingdom (UK). This publicly funded body serves a population of over 62 million and treats over 3 million people per week. The NHS provides medical care to the entire population, and is funded from direct taxation. Outside of this system some individuals pay for personal private health insurance which covers healthcare delivered in a small number of private hospitals, but the vast majority of the population receives its healthcare via the NHS.
Cardiology training in the UK follows on from an initial 4-year period of exposure to core medical subjects. Candidates who succeed in gaining membership of the Royal College of Physicians (via a multi part written and practical examination) can apply for entry into a 5 year cardiology program that covers a broad spectrum of general cardiology in the first three years. Entry into a cardiology training program is via a nationally administered selection process that is fiercely competitive. Sub-speciality PCI training occurs in the final 2 years of the program, giving first operator experience in several hundred PCI procedures, including adjunctive techniques such as IVUS, OCT, rotablation and laser therapy. Trainees frequently supplement this with research posts (during which they are expected to publish in peer reviewed journals and complete a research degree) and further interventional fellowships in the UK and abroad, which typically leads to a total training period of more than 10 years. The curriculum mandates that trainees are experienced in both transfemoral and transradial access which is feasible given the large volume of procedures now performed by both access sites in the UK.
Percutaneous coronary intervention has been undertaken in the UK since the early 1980s. The British Cardiovascular Intervention Society (BCIS) was set up in the late 1980s with the aim of promoting education, training, audit and research in cardiovascular intervention as well as developing and upholding professional and clinical standards. For the last 25 years the society has performed an annual audit of cardiovascular interventional procedures carried out in the UK. The BCIS database aims to record data on every PCI procedure performed in the UK. Annual reports on PCI activity from 1992 onwards are publicly available for download from the society’s website (https://www.bcis.org.uk). As of 2009, 97% of all PCI procedures performed in NHS hospitals were entered into the database. Data is collected on 113 procedure related variables including patient demographic features, indications for PCI, procedural details and outcome data. Robust mortality data is available by tracking patients unique NHS number in the NHS Central Register which records all deaths in the UK. The database contains information on almost half a million PCI procedures and the publicly available annual report details risk adjusted outcome data for individual units. The database also provides risk-adjusted funnel plots for individual operator performance, which will provide the basis for awarding an annual practice licence The database also provides a unique resource for ongoing research into PCI.
Since 1991, the number of PCI procedures has increased from 10,000 to over 85,000 procedures in 2010, with the rate of PCI increasing from 174 to 1407 PCI procedures per million population. As of 2010, there were 97 NHS hospitals that provided PCI with 52 of these offering a 24 hour/7 day per week primary PCI service. BCIS recommends a minimum requirement of 75 PCI procedures per year to maintain operator competency. Each operator performs on average 124 procedures per year.
In the early 1990s a small number of UK interventionists developed an interest in radial access, reporting their early experience in the literature. In 2000 an annual UK based Transradial Masterclass was established. In addition, a number of international transradial training fellowships were set up to allow trainees to spend up to a year in high volume radial units. The objective of the masterclass was to facilitate education and training in radial procedures using a format of live cases, lectures and angiogram review. In recent years the remit has expanded to include an international audience of high volume radial experts. The developing body of favorable published data and these educational initiatives have had a dramatic effect on UK access site practice. Use of radial access for PCI has increased from 50% in 2010. As of 2010, over 50% of hospitals use radial access for the majority of their PCI procedures. Radial access is used in 50% of all primary PCI and in 28% of procedures for cardiogenic shock. The rate of change in access site practice shows no sign of slowing, suggesting that radial access will largely have replaced femoral access in the UK within the next five years. Despite >50% use of femoral closure devices, the BCIS database records an incidence of vascular access complication with TFA that is more than double that observed with TRA. Analysis of the database has shown an association with reduced mortality in acute patients undergoing PCI with radial access, supporting the findings in smaller selected randomized studies.
Radial access is rapidly becoming the dominant access site for percutaneous cardiac procedures performed in the UK. The BCIS database provides a powerful tool to study this practice change in detail and this is the subject of a number of ongoing research projects supported by the society.
Transradial Cardiac Catheterization in Hungary
Imre Ungi*, György Szabó$, Ferenc Nagy*
*University of Szeged, Department of Cardiology, Szeged, Hungary and $Semmelweis University, Department of Cardiology, Budapest, Hungary
Number of invasive cardiology centers and proportion of public and private cathlabs in Hungary. For a long time before the millennium, cathlab capacities did not change much in our country: traditionally the medical universities and the National Heart Institute did all the diagnostic and interventional catheterizations. During the first decade of this millennium, our invasive cardiology care started to develop intensively. This change was mostly quantitative initially, i.e. the number of interventional centers rose from 6 cathlabs to 17 by this year, and the new labs were more evenly distributed according to the populations of regions. This increase was mostly boosted by a national program to decrease mortality of acute myocardial infarction (AMI).
In line with increasing density in the cathlabs, we worked up a highly organized primary PCI network. Interventional cardiology centers presently admit 80% of the AMI patient population, and only every 10th patient receives thrombolytic drug due to the inaccessibility of an interventional center in time.
The overwhelming majority of cathlabs in Hungary are in public hospitals and academic centers. Only three municipal and one university hospital were run by the private sector for a few years, but 3 of these 4 private labs were nationalized again.
Curriculum and education of interventional cardiology. Training has to meet the needs of increasing invasive cardiology activity by producing more and more trained interventional cardiologists. Background education in general cardiology is followed by practical experience, which is facilitated by the rapidly increasing caseload. The Working Group on Interventional Cardiology started a system of accreditation and developed a curriculum in interventional cardiology in 2008. The curriculum covers all the theoretical and practical fields of the specialty, the exam consists of a test and an essay on a real-world interventional case. The accredited doctors are classified into 1st, 2nd and 3rd level classes based on their experience, and the result of an examination in interventional cardiology. The 1st level of accreditation entitles one to perform diagnostic catheterization and start interventional training. The 2nd level of accreditation entitles one to perform coronary angioplasty independently, including acute MI service. The 3rd level of accreditation is given to the most experienced senior professionals with the skill of complex procedures. Directors of interventional centers are selected from this group of experts with 3rd level accreditation.
Evolution of radial access and number of procedures. Transradial approach remained a sporadic method of vascular access for a long time since the first TR diagnostic catheterization was performed in 1997. At first, the opportunity of early ambulation motivated us to start a TR program. Fighting down the major bleeding complications came only second. There were centers with serious limitations of sick-bed capacity at departments of cardiology, therefore we faced an intense push to discharge patients at the earliest possible time following cardiac catheterization.
In the period of 2000-2005 the rate of TR access varied between zero to 60% due to uneven infrastructural facilities and the diverse personal approach among operators. In the middle of the last decade we faced two factors that quickly propagated TR activity: an overwhelming majority of patients required this approach that provided them better comfort. Understandably, more and more interventional cardiologists met this challenge and attended intensive practical training course in high volume transradial centers. The other factor that pushed up the use of the TR approach was the growing published literature on the feasibility and safety of using the radial artery. Between 2005 and 2012 there was intense investment into new catheter centers and this led to widespread use of the TR approach, largely thanks to the activity of a young, ambitious generation of cardiologists and also because the growing evidence showing mortality reduction due to the TR approach in the most vulnerable acute MI population (Figure 1).
The statistical figures of both diagnostic and interventional procedures rapidly increased during the last 1-2 decades. While 15 years ago we performed 1500 diagnostic catheterizations and 200 PCI/1 million people, in 2011 these figures changed to 4000 coronary angiographies and 1900 PCIs, i.e. the number of coronary interventions grew almost ten times. The augmented experience and improved manual skill in TR technique extended its application into the field of acute interventions as well. During the last 1-2 years we performed more than 500 primary PCI/1 million annually, and the sum of all the acute MI cases including rescue interventions and non-ST elevation MI, reached about half of all procedures.
The statistics of interventional cardiology activity during 2011 demonstrated a 79% TR rate of all the cardiac catheterizations, and what is also important, today the radial artery is the first vessel of choice in the overwhelming majority of the centers (Figure 2). We have no data on how this high percentage is shared between elective and emergency procedures, however the rate of TR access for primary PCI exceeds 50% in all of the high-volume centers doing more than 300 primary PCI/year. This figure seems to be an important indicator that our operators are familiar with TR approach. Indeed, a significant mortality reduction gained by using the radial artery in acute MI population must be the primary goal of an acute MI service.
Policy on same-day discharge, challenges for the future. As we mentioned, the principal motivation of starting a TR program initially, was the early ambulation after cardiac catheterization. The present practice is usually the same-day discharge after TR diagnostic catheterization. Patients are supervised in an outpatient lounge for 4 hours, and then following a final checkup of the access site they are discharged. Following PCI, the patients have to stay at the hospital overnight due to reimbursement regulations. Presently, due to these rules we cannot follow the same-day-discharge principle for elective PCI, however, the overall hospital stay is significantly shorter for TR PCI than following the femoral approach.
Even with our high rate of TR access in Europe, we still have some challenges in this field. With the growing number of complex coronary interventions like complex morphology of bifurcations, calcified lesions, left main interventions and complex chronic total occlusion procedures, TR approach sometimes seems to be less feasible than using large diameter femoral guiding catheters. In this patient group we experienced a trend to step back to the femoral approach for safety reasons. Nevertheless, in the high volume TR centers we work hard on maintaining the high proportion of TR access with advanced techniques and devices, and making all attempts not to sacrifice the minimal invasivity for the bare technical success in case of a challenging intervention.
For a further development in application of TR approach we must increase its rate in acute MI, and for complex lesion subsets. We repeat more and more catheterizations for the same patient from the same radial artery; therefore we have to work out advanced methods of post-catheter vascular care in order to prevent a silent radial occlusion, and to preserve the vessel for future interventions.
BA001 - Bleeding & Anticoagulation
WARFARIN AND HEMOSTASIS AFTER TRANSRADIAL CARDIAC CATHETERIZATION Lippe C., Reineck E.A., Gilchrist I.C.
Corresponding author: Ian C Gilchrist, MD, Penn State Hershey Medical Center, 500 University Drive, Hershey, PA, 17033 USA. igilchrist@hmc.psu.edu
BACKGROUND: Warfarin has historically not been used during cardiac catheterization due to femoral bleeding risk, although this is now being questioned in the transradial era. The interaction between warfarin, hemostasis, and other potential safety issues has not been fully explored.
OBJECTIVE: This study examined if patients taking warfarin have similar hemostasis times to patients not taking warfarin after transradial catheterization.
METHODS: A convenience sample of patients underwent transradial catheterization at Hershey Medical Center June 2010 through May 2011. Hemostasis times of 187 patients taking warfarin (n=34) and not taking warfarin (n=153) were compared. Patients were further separated, based on anti-platelet therapy: clopidogrel alone, aspirin alone, clopidogrel and aspirin, and neither clopidogrel nor aspirin. Compression band time was used as a hemostasis marker. After data collection, an analysis of variance model was used to adjust for aspirin, clopidogrel, and warfarin.
RESULTS: Of 187 patients, 34 (18%) were taking warfarin. Anti-platelet data was assessed with 5 patients (3%) taking clopidogrel alone, 91 patients (49%) taking aspirin alone, 63 patients (34%) taking both aspirin and clopidogrel, and 28 patients (15%) taking neither aspirin nor clopidogrel. The difference in mean band times between warfarin versus non-warfarin patients was not non-statistically significant (120 minutes vs. 115 minutes, respectively; p = 0.16). Likewise, there was not a statistically significant difference between patients taking aspirin versus not taking aspirin (118 minutes vs. 107 minutes, respectively; p = 0.09). The use of clopidogrel independently correlated with a prolonged hemostasis time (125 minutes clopidogrel vs. 111 minutes no clopidogrel; p = 0.02).
DISCUSSION: The observed differences in hemostasis time likely relate to differering mechanisms of antihemostatic agents. Aspirin and clopidogrel are both anti-platelet agents, which decrease platelet adhesion and aggregation, modifying hemostatic platelet activity at the site of arterial wall injury. Contrastingly, warfarin blocks production of vitamin K clotting factors and proteins C and S, which are activated only after platelets start the clotting process. This may account for why warfarin was observed to have a lesser effect on hemostasis times.
CONCLUSION: There was no apparent difference in hemostasis times between patients taking warfarin and those not taking warfarin once the confounding influence of antiplatelet therapy was controlled. This suggests hemostasis time is associated with the intensity of antiplatelet therapy rather than antithrombin effects.
Nothing to disclose / No conflicts of interest
BA002 - Bleeding & Anticoagulation
LOWER TRANSFUSION RATES FOLLOWING PERCUTANEOUS CORONARY INTERVENTION VIA THE RADIAL APPROACH: A FOUR-YEAR, SINGLE-CENTER EXPERIENCE
Kahan D.J., Riskalla N.S., Pyne C.T.
Corresponding author : Christopher T Pyne, MD, Department of Cardiology, Lahey Clinic Medical Center, 41 Mall Road, Burlington, Massachusetts, 1805 USA. Christopher.T.Pyne@Lahey.org
PURPOSE: We sought to assess the hypothesis that transfusion rate--as a marker for significant bleeding--would be lower using the radial approach in percutaneous coronary intervention (PCI). We also sought to identify the causes of blood transfusions in patients recieving PCI through the radial approach.
BACKGROUND: Prior investigators have demonstrated the substantial, negative effect of bleeding following percutaneous coronary intervention (PCI). The transradial approach for PCI significantly decreases access site bleeding compared to the femoral approach. The impact on RBC transfusion in an institution performing a large volume of PCI cases of all presentation types remains unknown.
METHODS: Retrospectively reviewing all PCI procedures at our institution performed between Jan 2006 and Feb 2010, we compared transfusion rates by access site and procedure indication, and explored etiologies of bleeding. Propensity matching was used to control for differences in the radial and femoral group.
RESULTS: Overall, there were 5255 PCI cases during the study period, 1038 via the radial approach, 4217 via femoral. The overall transfusion rate was significantly lower in the radial group, 2.1% vs. 6.2% (p<0.0001), had more chronic kidney disease (51% vs. 30%; P=0.0012) and underwent more often primary PCI (30% vs. 14%, P
CONCLUSIONS: A transradial approach for PCI is associated with a significantly lower transfusion rate following elective and emergent procedures. Transfusions in radial PCI patients occurred at non-access sites, or from additional femoral access for hemodynamic support devices.
Nothing to disclose / No conflicts of interest.
BA003 - Bleeding & Anticoagulation
BIVALIRUDIN VERSUS HEPARIN-MONOTHERAPY IN ALL COMERS AFTER PERCUTANEOUS INTERVENTION: THE QUEBEC HEART-LUNG INSTITUTE EXPERIENCE.
MacHaalany J., Abdelaal E., Bataille Y., Larose E., Déry J-P., Delarochellière R., Rinfret S., Roy L., Proulx G., Gleeton O., Rodés-Cabau J., Noël B., Barbeau G., Nguyen C., Costerousse O, Bertrand OF.
Corresponding author : Jimmy MacHaalany, MD, Quebec Heart and Lung Institute, 2725 chemin Sainte-Foy, Quebec, QC, G1V 4G5, Canada. jmach@magma.ca
PURPOSE: Bivalirudin, a direct thrombin inhibitor, has been shown to reduce major bleeding and provide a better safety profile compared to unfractionned heparin (UFH) in patients undergoing percutaneous coronary intervention (PCI) via transfemoral access. Data pertaining to the clinical benefit of bivalirudin over UFH monotherapy in patients undergoing transradial PCI is lacking. This study sought to compare the in-hospital net clinical adverse events (NACE) including death, MI, target vessel revascularization and bleeding of these two different antithrombotic regimens in all comers at a tertiary care high-volume radial center.
METHODS: From Apr 2009 to Feb 2011, all patients treated with bivalirudin were matched for access-site to UFH patients. Baseline characteristics, procedural data, and blood tests were analysed for in-hospital: i) NACE, ii) major adverse cardiovascular events (MACE) (defined as death, myocardial infarction (MI) and target vessel revascularization (TVR)), and iii) non-CABG related bleeding (BARC Type 3-5).
RESULTS: Radial approach was used in 71% in both groups. Patients in the bivalirudin group (n=125) were older (72 ± 13 years vs. 66 ± 11 years; P<0.0001), had more chronic kidney disease (51% vs. 30%; P=0.0012) and underwent more often primary PCI (30% vs. 14%, P<0.0037) than UFH-treated patients (n=125). Baseline bleeding risk according to Mehran’s score was similar in both groups (14 ± 9 vs. 15 ± 8, P = 0.48). In-hospital mortality was 2% in both groups (P= 1.00). No difference in NACE, ischemic or bleeding complications was detected between the 2 groups.
CONCLUSION: Bivalirudin reduced both ischemic and bleeding events in femoral treated-patients whereas no such clinical benefit was observed in radial treated-patients. As peri-PCI bleeding-avoidance strategies have become paramount to optimize the clinical benefit, the interaction between bivalirudin and radial approach deserves further investigation.
Nothing to disclose / No conflicts of interest
BA004 - Bleeding & Anticoagulation
TRANSRADIAL CATHETERIZATION DURING UNINTERRUPTED ORAL ANTICOAGULATION: RESULTS OF A PILOT STUDY EMPLOYING AN INR - ADJUSTED HEPARIN DOSING PROTOCOL.
Visweswaran G.K.(1), Singh G.(2), Yadav P.K.(2), Gilchrist I.C.(2).
(1) Division of General Internal Medicine; (2) Penn State Hershey Heart and Vascular Institute. Milton S. Hershey Medical Center, Penn State College of Medicine.
Corresponding author : Gautam K Visweswaran, MD, Milton S. Hershey Medical Center, Penn State College of Medicine. Hershey, Pennsylvania, 17033 USA. gvisweswaran@hmc.psu.edu
PURPOSE: Temporary discontinuation of anticoagulation and/or heparin bridging remains prevalent practice prior to cardiac catheterization in chronically anticoagulated patients. The optimal heparin dose to achieve a therapeutic ACT (Activated Clotting Time) of 200secs remains unclear with widespread use of arbitrary dosing. We report preliminary results of an INR-adjusted heparin dosing algorithm to minimize radial artery occlusion (RAO)/complications while effecting same day diagnostic transradial catheterization without discontinuation of oral anticoagulation.
METHODS: Standard NCDR baseline demographics and medications were recorded. ACT measurements immediately before and 10 mins after administration of an INR-adjusted heparin dosing regimen (if INR 200secs.
RESULTS: Patients (N=43) underwent diagnostic radial catheterization on uninterrupted oral anticoagulation [INRs < 1.5 (16.3%); ≥ 1.5 and < 2 (32.5%); ≥ 2 and < 3 (48.9%) and ≥ 3 (2.3%)] with planned heparin therapy. A strong positive correlation was noted between the Index INR and Index ACT (r=0.598, p<0.01). 32 (74.41%) patients received heparin dosing per protocol with 11 (25.6%) receiving dose as per the discretion of the attending physician (median=27.78 IU/kg, range 14.03 IU/Kg – 53.28 IU/kg). Of the 32 patients who received heparin per protocol the final ACT was 213.71 ± 31.95 (p=0.021). No instances of hyperanticoagulation or bleeding were noted. All the patients were discharged the same day. Follow up was available for 72% of patients (median=8 days, range 1-86days) during which no complaints of late arm weakness or pain was reported.
CONCLUSION: An INR-adjusted heparin dosing protocol may be a safe and reasonable method to achieve optimal anticoagulation as assessed by ACT in patients on Coumadin. Further work is needed to assess such INR-driven, heparin-dosing algorithms on outcomes such as RAO that has been reported to be relatively high on warfarin alone. Uninterrupted anticoagulation employing procedural heparin may be protective against post procedure RAO though objective Doppler assessment was not done. Transradial diagnostic radial catheterization can be safely undertaken without interruption of chronic anticoagulation optimizing health care resource utilization.
Nothing to disclose / No conflicts of interest
BA005 - Bleeding & Anticoagulation
INCIDENCE, PREDICTORS AND CLINICAL IMPACT OF BLEEDING AFTER TRANSRADIAL CORONARY STENTING AND MAXIMAL ANTIPLATELET THERAPY
Bertrand OF, Larose E, Rodes-Cabau J, Gleeton O, Taillon I, Roy L, Poirier P, Costerousse O, De Larochellière R
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND : Bleeding after percutaneous coronary intervention (PCI) using femoral approach has recently emerged as an independent risk factor of early and late mortality. Transradial PCI is associated with a lower risk of access site complications than femoral approach. We sought to determine the predictors of bleeding and evaluate the impact of major bleeding on death and major adverse cardiac events (MACE) after transradial PCI and maximal antiplatelet therapy.
METHODS: In the EASY trial, 1348 acute coronary syndrome patients were enrolled and underwent transradial PCI. All patients received clopidogrel (90% ≥ 12h pre-PCI) and a bolus of abciximab prior to first balloon inflation. Independent predictors and prognostic impact of major bleeding on death and MACE (death, MI and TVR) were assessed using multivariate analysis.
RESULTS : From the study population, 19 patients (1.4%) presented major bleeding. Among baseline characteristics only creatinine clearance < 60 ml/min was an independent predictor of bleeding (Odds Ratio (OR) 3.49, 95% CI 1.17-9.48, P = 0.017). Peri-procedural independent predictors of bleeding were procedure duration (OR 3.42, 95% CI 1.25-10.31, P = 0.020) and sheath size (OR 4.98, 95% CI 1.33-32.36, p = 0.038). In patients with major bleeding, the incidence of MACE was higher at 30 days (37% vs. 3%), 6 months (42% vs. 8%) and at 12 months (53% vs. 12%), P < 0.0001 for all comparisons. By multivariate analysis, major bleeding was an independent predictive factor of 1-year mortality and MACE.
CONCLUSION : After transradial PCI and maximal antiplatelet therapy, the incidence of major bleeding remains low. Major bleeding is an independent predictive factor of adverse acute and 1-year outcomes, regardless of the access site.
Nothing to disclose / No conflicts of interest
BA006 - Bleeding & Anticoagulation
INCIDENCE, RANGE AND CLINICAL IMPACT OF HEMOGLOBIN AND PLATELET DECREASE AFTER TRANSRADIAL CORONARY STENTING AND MAXIMAL ANTIPLATELET THERAPY IN THE EASY TRIAL.
Bertrand O, Rodés-Cabau J, Rinfret S, Larose E, Déry JP, Gleeton O, Nguyen CM, Proulx G, Roy L, Costerousse O, Poirier P, De Larochellière R
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND : Major bleeding is a major predictor of death and adverse outcomes after percutaneous coronary intervention (PCI). Yet, several definitions have been applied with different cut-offs. Although transradial approach dramatically reduces the incidence of major bleeding, the hemoglobin (Hb) changes after transradial PCI have not been defined. We have compared the baseline values of Hb and platelets with those obtained 4-6 h and 12-24 h after transradial coronary stenting and maximal antiplatelet therapy.
METHODS : In the EASY trial, 1348 patients with acute coronary syndrome underwent transradial coronary stenting. All patients received clopidogrel prior to PCI (90% ≥ 12h pre-PCI) and a bolus of abciximab prior to first balloon inflation. Hb and platelet counts were measured immediately after sheath insertion, 4-6h after PCI and 12-24h later. MACE (Death, MI and TVR) were assessed up to 3 years after PCI.
RESULTS : The mean Hb value was 13.97 ± 1.34 g/dL before PCI, 13.11 ± 1.31 g/L 4-6h after PCI and 13.32 ± 1.42 g/L 12-24h post-PCI. According to World Health Organization (WHO) classification, 13% of men (Hb < 13 g/dL) and 23% of women (Hb < 12 g/dL) were anemic prior to PCI (P < 0.0001) and 38% of men and 60% of women were anemic post-PCI (P < 0.0001). At 30 days, patients with MACE had lower Hb value 12-24h post-PCI, 12.77 ± 1.51 g/dL compared to patients without cardiac events, 13.34 ± 1.41 g/dL, P = 0.01. Patients with MACE at 3 years had lower Hb value prior to PCI, 13.80 ± 1.37 g/dL vs 14.01 ± 1.34 g/dL (P = 0.024) and lower Hb value 12-24h post PCI, 13.09 ± 1.50 g/dL vs 13.38 ± 1.39 g/dL (P = 0.004). By multivariate analysis, Hb pre-PCI was an independent predictor of MACE at 3 years (HR 0.98 95% CI 0.97-0.99, P = 0.01). Platelets dropped from 239 ± 60 x109/L prior to PCI to 235 ± 63 x109/L 4-6h post-PCI and 234 ± 64 x109/L 12-24h post-PCI. Patients with MACE at 30 days had lower platelets counts prior to PCI, 4-6h and 12-24h post-PCI (P < 0.05 for all) compared to patients without cardiac events.
CONCLUSION : After transradial PCI and maximal antiplatelet therapy, there was a mean Hb decrease of 1 g/dL and 13 x109/L platelets counts. Using WHO classification, ~ 40% of men and 60% of women were anemic post-PCI. The exact duration of post-PCI anemia and its clinical impact requires further investigation.
Nothing to disclose / No conflicts of interest
BA007 - Bleeding & Anticoagulation
TRANSRADIAL APPROACH AND BIVALIRUDIN USE IN ELDERLY PATIENTS UNDERGOING EARLY INVASIVE STRATEGY FOR ACS
Summaria F, Patrizi R, Romagnoli E, De Luca L, Mustilli M, Pagnanelli A.
Corresponding author : Francesco Summaria, MD, Interventional Cardiology, Policlinico Casilino, Rome, 168, Italy. f.summaria@gmail.com
PURPOSE: Due to the ageing population and raised life expectancy, elderly patients are increasingly referred for percutaneous coronary intervention (PCI) during acute coronary syndromes (ACS). A disproportionately lower use of cardiovascular medications and invasive treatment in elderly compared to younger patients with ACS is observed. Notably, major bleeding became an increasing concern for interventional cardiologists and different studies demonstrated an increased mortality for patients with haemorrhagic complications. Recent studies pointed out that bivalirudin compared to heparin and GPIIb/IIIa inhibitors is associated with an approximately 40% reduction in both nonaccess site as well as access site bleedings together with similar antithrombotic protection if an adequate antiplatelet pretreatment is provided.
METHODS: We prospectively collected data from 84 consecutive ACS patients aged above 70 years treated with an early revascularization strategy by transradial approach using bivalirudin as antithrombotic therapy. The bivalirudin was used intraprocedural with a bolus dose of 0.75 mg/kg followed by infusion of 1.75 mg/kg/h. All patients included were pretreated with a loading dose of 300mg of ASA and 600mg of clopidogrel. Patients were stratified for bleeding complications and for ‘frailty’. The overall in hospital and 1-month MACE rates (cardiac death, myocardial infarction and target lesion revascularization), need for blood transfusions, length of hospital stay and stent thrombosis were evaluated.
RESULTS: Diagnosis at admission was a STEMI in 53 and a NSTEMI in 31 cases. Male/female ratio was 22/62. Mean age was 79.74 years (range 70–91) and median 81. The transradial approach was successfully performed in all procedures: in 79 (94%) from left wrist and in 5 (6%) from right one. No patient required blood transfusion during hospital stay, but one patient (1.19%) experienced a clinically relevant gastrointestinal bleeding. No patient died during hospitalization and one (1.19%) subacute stent thrombosis occurred 16 days after the procedure, related to premature dual antiplatelet discontinuation. At mean follow-up of 30+5 days MACEs occurred in five (5.95%) patients including one (1.19%) cardiac death, two (2.38%) myocardial infarction and two (2.38%) target lesion revascularization.
CONCLUSION: This registry shows that combined pharmacoinvasive treatment using intraprocedural bivalirudin and the radial approach to PCI is well tolerated and associated with a low incidence of adverse events in elderly patients with ACS.
Nothing to disclose / No conflicts of interest
BA008 - Bleeding & Anticoagulation
REDUCED BLEEDING RATES AND IMPROVED CLINICAL OUTCOMES WITH THE USE OF RADIAL ACCESS IN OCTOGENARIANS UNDERGOING PERCUTANEOUS CORONARY INTERVENTION
Déry JP, Déry U, Tizon-Marcos H, Barbeau G, Rodes-Cabau J, Rinfret S, Larose E, Alexander KP, Rao SV, Nguyen CM, Noel B, Proulx G, Roy L, Gleeton O, De Larochelliere R, Bertrand OF.
Corresponding author : Jean-Pierre Déry, MD MSc, Quebec Heart and Lung Inst, Quebec, QC, Canada;
BACKGROUND: Octogenarians undergoing PCI are at a higher risk of bleeding complications. The use of the radial artery for vascular access site has been proposed to lower the risk of bleeding in patients undergoing PCI. We sought to compare bleeding risks with transradial PCI vs transfemoral PCI in octogenarians undergoing PCI.
METHODS and RESULTS: We retrospectively analyzed a cohort of 891 consecutive octogenarians who underwent PCI between 2002 and 2007 at a tertiary care centre where the default vascular access is the radial artery. Bleeding events and long-term mortality were obtained by chart review and phone interview (98% complete). Outcomes of patients who underwent transradial PCI (n=779) were compared to those of patients who were treated from the femoral artery (n=112). Transfemoral patients more frequently had a history of heart failure (26.8% vs 18.7%;p=0.04), peripheral vascular disease (34.8% vs 19.2%;p=0.0003), prior CABG (26.8% vs 12.1%;p<0.0001), 32 (74.41%) patients received heparin dosing per protocol with 11 (25.6%) receiving dose as per the discretion of the attending physician (median=27.78 IU/kg, range 14.03 IU/Kg – 53.28 IU/kg). Of the 32 patients who received heparin per protocol the final ACT was 213.71 ± 31.95 (p=0.021). No instances of hyperanticoagulation or bleeding were noted. All the patients were discharged the same day. Follow up was available for 72% of patients (median=8 days, range 1-86days) during which no complaints of late arm weakness or pain was reported.
CONCLUSION: In octogenarians undergoing PCI, the use of a transradial approach was associated with a lower risk of bleeding and improved one-year survival. This suggests that transradial PCI is an effective bleeding reduction strategy which may potentially reduce long-term mortality. Radial access should be encouraged in all patients with an increased bleeding risk, including octogenarians.
Nothing to disclose / No conflicts of interest
HRO001 - Hemostasis & Radial Artery Occlusion
ABCIXIMAB FACILITATES THE TREATMENT OF RADIAL ARTERY OCCLUSION
Jaradat Z., Basir B., Revtyak, G.
Corresponding author : George E. Revtyak, MD, IU Health Physicians Cardiology, 1801 N Senate Blvd, Suite #310, Indianapolis, IN, 46202 USA. grevtyak@iuhealth.org
PURPOSE: To study an alternative strategy for treating radial artery occlusion (RAO) using balloon angioplasty (PTA) and intra-thrombus administration of abciximab.
METHOD: A retrospective review patients in our data base between 2009 and 2011 who underwent treatment for symptomatic RAO was made. These patients were treated with PTA alone or PTA and intra-arterial abciximab administered directly at the site of occlusion.
RESULTS: Five patients with symptomatic RAO following transradial catheterization were treated with PTA. Of these patients, four received a 90 second intra-thrombus infusion of abciximab via a Clearway catheter placed at the site of initial occlusion. All procedures were initially successful. Radial artery patency was documented with duplex sonography immediately post-procedure, the following day and again at follow-up (mean 189 days). Radial artery patency was maintained in the four patients who received abciximab in addition to PTA. RAO was observed in the only patient treated with PTA alone. All patients remained free of symptoms at follow-up.
CONCLUSIONS: PTA with intra-thrombus administration of abciximab using a Clearway catheter appears to be a safe, effective and durable technique for re-establishing the patency of an occluded radial artery following transradial catheterization. Larger studies are needed to confirm our findings and establish the role for this technique in an algorithm for treatment of RAO.
Nothing to disclose / No conflicts of interest
HRO002 - Hemostasis & Radial Artery Occlusion
PREDICTORS OF RADIAL ARTERY SIZE IN PATIENTS UNDERGOING CARDIAC CATHETERIZATION – INSIGHTS FROM THE GOOD RADIAL ARTERY SIZE PREDICTION STUDY (GRASP)
Kotowycz MA, Johnston KW, Ivanov J, Asif N, Almoghairi AM, Choudhury A, Nagy C, Sibbald M, Seidelin PH, Barolet AW, Overgaard CB, Džavík V
Corresponding author : Mark A. Kotowycz, MD MBA FRCPC, Peter Munk Cardiac Centre, University Health Network, Toronto General Hospital, Toronto, ON, Canada. mark.kotowycz@mail.mcgill.ca
BACKGROUND: A small percentage of patients undergoing cardiac catheterization or percutaneous coronary intervention (PCI) via the transradial approach develop permanent occlusion of the radial artery as a result of the procedure. Although the use of a sheath that is larger than the resting diameter of the radial artery is one of the risk factors for radial artery occlusion, radial artery size is not routinely assessed prior to catheterization.
METHODS: We designed a prospective, observational study to determine if there are reliable bedside predictors of radial artery size. Ninety patients presenting for elective PCI or diagnostic coronary angiography were studied with ultrasound prior to catheterization and the diameters of their radial, ulnar and brachial arteries were measured. We correlated these measurements with prespecified candidate variables in order to identify predictors of radial artery size.
RESULTS: The mean internal diameters of the right radial, ulnar and brachial arteries were 2.41 +/- 0.61, 2.04 +/- 0.47 and 4.47 +/- 0.86 mm, respectively. Results for the left arm were similar. The right radial artery was larger in men than in women (2.56 vs. 1.83 mm, p<0.001), and smaller in patients of south Asian descent (1.89 vs. 2.54 mm, p<0.001), and smaller in patients of south Asian descent (1.89 vs. 2.54 mm, p<0.001). Radial artery diameter was correlated with wrist circumference (r2=0.36, p<0.001) and shoe size (r2=0.31, p<0.001). There was weaker correlation between radial artery diameter and height (r2=0.19, p<0.001), weight (r2=0.22, p<0.001), body mass index (r2=0.09, p=0.008), body surface area (r2=0.29, p<0.001) and no correlation with reverse Allen’s time (r2=0.02, p=0.31). The independent predictors of radial artery diameter from a multiple linear regression were shoe size (r2=0.352, p<0.001), male sex (r2=0.027, p=0.078) and non-south Asian ancestry (r2=0.024, p=0.094). The final model r2=0.40 (p<0.001). Patients who experienced pain on sheath insertion or removal had smaller radial arteries than those who did not (1.87 vs. 2.57 mm, p<0.001). Patients with acute radial artery occlusion (4%) had smaller arteries than those without occlusion (1.96 vs. 2.45 mm, p<0.001).
CONCLUSION: Radial artery occlusion is observed in patients with smaller arteries and patients with smaller radial arteries are more likely to experience pain on sheath insertion or removal. Shoe size, male sex and non-south Asian ancestry are independent predictors of radial artery size.
Nothing to disclose / No conflicts of interest
HRO003 - Hemostasis & Radial Artery Occlusion
PULSE OXIMETRY VERSUS DOPPLER FOR PATENCY EVALUATION AT 24H AND 1 MONTH AFTER TRANSRADIAL APPROACH. RESULTS OF THE RANDOMIZED CRASOC (COMPRESSION OF RADIAL ARTERIES WITHOUT OCCLUSION) STUDY.
Dangoisse V., Guédès A, Chenu P, Jamart J, Gabriel L, Marchandise B, Jourdan J, Albert C, Dury C, Schroëder E
Corresponding author : Vincent Dangoisse, MD, CHU Mont Godinne, UCL, Av Therasse,1, YVOIR, 5530, BELGIUM. vdangoisse@me.com
PURPOSE: 24 h after transradial access (TRA) for cardiac catheterization, the finding of a positive pulse oximetry (PPO) when compressing the ulnar artery signs a patent radial artery and can be used as a surrogate for long-term radial artery patency. The aim of the study was to analyze the radial artery patency by Doppler when negative or doubtful pulse oximetry was present at 24h and to assess final patency at 1 month.
METHOD: From January 2007 to June 2011, 2032 TRA were randomized to compression with “low inflation volume” (13cc of air) versus “ultra low inflation volume“(10 cc) using the TR Band compression device. Type of compression (“patent hemostasis “ or not) was assessed at the time of TR Band positioning.
RESULTS: PPO was present at 24h for 1871 of 2032 TRA (92%). For 137 of the 161 non positive pulse oximetries (85,1%), a first Doppler signal (before hospital discharge for 125 or later for 12) identified a positive wave (patent artery) for 98 arteries (71,5%). The signal was negative (occlusion) or doubtful for 40 (36 in hospital + 4 out of hospital). Of the 36 abnormal Doppler results analyzed at 24 h, 18 were re analyzed at 1 month, and we found patency for half (radial pulse and positive Doppler wave).
CONCLUSION: A positive signal Doppler (patent artery) is present for about 70% of the negative or doubtful pulse oximetry tests when performed 24h after TRA. 50% of occluded or doubtful radial artery patency at hospital discharge (by pulse oximetry and by Doppler analysis) are patent by 1 month. With these observations, we extrapolated the value for the full cohort of 2032 TRA. We counted 13 radial artery occlusions (RAO) but with extrapolation, 24 (1,2%) arteries would be occluded (50% RAO for the 30% of the 161 negative or doubtful pulse oximetry at 24h). With «patent hemostasis», RAO extrapolated value is 1,07%(10/933), versus 1,39%(14/1004) for non-patent hemostasis. With ultra low volume of compression (n =851), corrected RAO rate is 0,94% (8/851), versus 1,44 % (17/1181) for low volume of compression (n=1181). Finally, ultra low volume of air (10 cc) used with the TR Band compression results in a less than 1% of RAO at 1 month.
Nothing to disclose / No conflicts of interest
HRO004 - Hemostasis & Radial Artery Occlusion
RECANALIZATION OF LATE OCCLUSION OF RADIAL ARTERY AFTER PREVIOUS TRANSRADIAL INTERVENTIONS: CAN WE USE THE SAME ARTERY FOR REPEAT INTERVENTIONAL PROCEDURES?
Babunashvili A.M., Dundua D.P.
Corresponding author : Avtandil M Babunashvili, MD, PhD, 111123, 62 shosse entuziastov, Moscow, Russian Federation, Center of Endosurgery, Department of cardiovascular surgery, Moscow, Russian Federation. avtandil.babunashvili@gmail.com
PURPOSE: To assess possibility of recanalization and reuse of chronic or subacute radial/ulnar artery occlusion (RAO/UAO) after previous transradial or transulnar interventions (TRI/TUI).
METHODS: RAO/UAO occurred in 71 cases out of 1131 repeat TRI/TUI (6,2%). We analyzed results of recanalization procedures 60 occluded segments of radial (RA) or ulnar (UA) artery after previous TRI/TUI. The mean age of cohort was 61,5±9,8 years (ranged 45-84), 51 (85%) were men and 5 (8,3%) were diabetics. The time interval from initial TRI/TUI procedures until repeat catheterization (recanalization) was 1 day-5,9 year (mean 299±421 days). Majority of the patients (n=48, 80%) were admitted with CTO of 47 RA and 1 UA. Remaining 12 patients (20%) had subacute occlusion of 11 RA and 1 UA. In cases of successful recanalization we used “Dotter type” vessel recanalization in 16 (31,4%) cases, balloon angioplasty without previous Dotter procedure in 22 (43,1%) cases and combined technique in 12 (23,5%) cases. For each pre- and post-treatment angiogram following QA parameters were calculated. Follow-up results were assessed by retrograde angiography of radial/ulnar artery, as well as with Doppler ultrasound examination.
RESULTS: Recanalization of occluded RA/UA was successful in 51 cases (85%). Procedure was completed successfully in 11 out of 12 cases of subacute occlusion (91,7%) and in 40 out of 48 cases of CTO (83,3%). Mean procedure time was 16±9,6min, radiation exposure dose - 47,26±120,4 µGy/m2 (mean 2% of total dose of coronary intervention procedure thereafter). The final Minimal Lumen Diameter (MLD) measured after recanalization of occluded artery was 2,15±0,4mm. In terms of recanalization technique MLD was 2,12±0,35mm, 2,16±0,49mm and 2,17±0,32mm after “Dotter-type” recanalization, balloon angioplasty only and combined technique, respectively (p=0,942). Multivariate logistic regression analysis shown that lengths of occlusion and distal postocclusion segment were predictors of technical failure (p=0,039 and p=0,013, respectively). At follow-up (3 day-85 month) reocclusion was occurred in 23 cases (45,1%). In 2 patients we performed successful repeat recanalization after reclosure of radial artery 3 and 5,5 months after intial recanalization.
CONCLUSION: Our findings indicate that recanalization of late occlusion of radial/ulnar artery could be performed with high success rate, minor risk of complication and minimal radiation exposure dose. There are more benefit than disadvantages of this technique which are partially addresses the difficulties of punction and catheterization of distal postocclusion part of occluded radial/ulnar artery.
Nothing to disclose / No conflicts of interest
HRO005 - Hemostasis & Radial Artery Occlusion
AMPUTATION OF THE RIGHT ARM AS A CONSEQUENCE OF DIAGNOSTIC CORONARY ANGIOGRAPHY
Rezek M.
Corresponding author : Michal Rezek, MD, 1st Department of Internal medicine – cardioangiology, St. Anne’s University Hospital, International Clinical Research Center, Brno, Czech Republic, Bulgarian Cardiac Institute, Cardiology Clinic Varna, Bulgaria, Brno, 61500, Czech Republic. rezek@fnusa.cz
INTRODUCTION: Amputation of the arm is a nightmare complication for every interventional cardiologist who is performing cardiac catheterization via radial artery. We report a rare case, which due to several unhappy conditions led to this frightening complication.
DESCRIPTION OF THE CASE: 42-year-old man underwent a diagnostic coronary angiography via radial access in one of the catheterization laboratories in Varna, Bulgaria. There was no complication of the procedure and the patient was discharged the next day. Retrospectively the patient reported very strong and prolonged compression after the procedure.
Two days after, this patient presented to another hospital with acute pain of the right hand and the physical examination revealed acute ischemia with no pulsations on the radial and ulnar artery. The patient was admitted to the Department of Vascular Surgery and a trombectomy was performed via right brachial artery using Fogarty catheter. There was no angiography or other diagnostic method performed before or after the surgery. After the trombectomy restoration of the pulsations on the ulnar artery was described. Two days after, another trombectomy was performed because of the pulseless right hand and two days later the patient was finally sent to our institution for an angiography of the right arm. This was done via right femoral access and an occlusion of both arteries radial and ulnar with no collateral flow was described. We performed an attempt for recanalization of the two arteries, but without success. It was not possible to cross the occlusions using different coronary angioplasty wires (Terumo Runthrough, PT2LS, PT2MS). The patient was sent back to the Department of Vascular Surgery, then signed the AMA form and left for another hospital in the capital city of Bulgaria, Sofia, where due to progressive ischemia the amputation of the right hand in forearm had to be performed.
CONCLUSION: It remains unclear, why the patient had occlusion of both radial and ulnar artery. There was no angiography performed before the trombectomy and even though the restoration of pulsations after the trombectomy was reported, the most probable reason for ulnar occlusion was the dissection after the surgery with Fogarty catheter. This case illustrates the importance of very careful and standardized management of patients after radial catheterization and the need of precise diagnostic documentation before and after every interventional procedure.
Nothing to disclose / No conflicts of interest
HRO006 - Hemostasis & Radial Artery Occlusion
SUCCESSIVE TRANSRADIAL ACCESS FOR CORONARY PROCEDURES: EXPERIENCE OF QUEBEC HEART-LUNG INSTITUTE
Abdelaal E., Molin P., Plourde G., MacHaalany J., Bataille Y., Provencher C., Montminy S., Larose E., Roy L., Gleeton O., Barbeau G., Nguyen C., Noël B., Costerousse O., Bertrand O.F.
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
PURPOSE: The aim of current study was to evaluate the number of times the same radial artery can be used for repeat access for coronary procedures, and reasons for failure.
BACKGROUND: Transradial approach (TRA) for cardiac catheterizations and interventions improves clinical outcomes compared to transfemoral access and its use is increasing worldwide. However, there is limited data on successive use of same artery for repeat procedures.
METHODS: Between May 2010-May 2011, all consecutive patients undergoing a repeat TRA procedure (≥2) were identified. Success rates and reasons for failure to use ipsilateral radial artery for repeat access were identified.
RESULTS: A total of 520 patients underwent 1423 procedures. In 480 patients (92%) right radial artery was used as initial access, and left radial artery in 39 patients. All patients underwent ≥ 2 procedures, 219 patients ≥ 3, 87 patients ≥ 4, 39 patients ≥ 5, 19 patients ≥ 6, 11 patients ≥ 7, and 5 patients ≥ 8 procedures. Two patients had respectively 9 and 10 procedures. The success rate for second attempt was 93%, 81% for third, declining to 60% for ≥ 8. Linear regression analysis estimated a 5% failure rate for each repeat attempt (R2 = 0.87, P = 0.007). The main reason for failure was related to clinical radial artery occlusion (RAO) including absent or faint pulse, poor oxymetry, and failed puncture. All patients with clinical RAO were asymptomatic. By multivariate analysis, female gender (OR 3.08, 95% CI: 1.78-5.39, P < 0.0001), prior coronary artery bypass graft (OR 5.26, 95% CI: 2.67-10.42, P < 0.0001) and repeat radial access (OR 2.14, 95% CI: 1.70-2.76, P < 0.0001) were independent predictors of radial access failure.
CONCLUSION: Successive TRA is both feasible and safe in a majority of cases for up to 10 procedures. However, failure rate for TRA increases with successive procedures, primarily due to clinical RAO. Strategies to minimize the risks of chronic clinical RAO and allow repeat use of ipsilateral radial artery need to be further defined.
Nothing to disclose / No conflicts of interest
HRO007 - Hemostasis & Radial Artery Occlusion
DRUG ELUTING BALLOON ANGIOPLASTY FOR REPEATED REOCCLUSION OF THE RADIAL ARTERY
Katona A., Ungi I.
Corresponding author : András Katona, MD, 2nd Department of Internal Medicine, Cardiology Center, Invasive Cardiology, Pécsi u.4., Szeged, 6724, Hungary, kabandi81@hotmail.com
A 70-yr-old man was referred to cardiac catheterization due to NSTE-ACS. The Allen test proved to be positive before coronary angiography preformed from the right radial approach with a 6F introducer sheath and 5F diagnostic catheters. No intervention was done in lack of significant stenosis.
One month later, the patient was admitted again with serious ischemic symptoms of his right hand.Doppler ultrasound revealed a total occlusion of the radial artery, and a poor collateral circulation from the seriously sclerotic ulnar artery. Angiography confirmed the radial occlusion, and a POBA was done from an ispilateral axillary approach with good angiographic result and a complete recovery of the signs of ischemia.
After 6 month symptoms of hand ischemia recurred againeven with necrotic spots of the fingers. Angiography confirmed a reocclusion of the radial artery and a fast progression of the disease of the ulnar artery. Another radial balloon angioplasty was done with excellent angiographic result again. During the regular follow up the patient remained free of symptoms, and serial Doppler studies demonstrated a widely opened vessel.
Finally, after 4 years of the first catheterization hand ischemia recurred again. At that time a total occlusion of the ulnar and radial arteries was found. Surgery was refused again, therefore a catheter-based recanalization was performed again and the intervention was completed with a drug-eluting balloon angioplasty. The 6-month clinical and Doppler ultrasound follow- uprevealed an excellent medium-term result again.
This case demonstrates the feasibility of three repeated balloon angioplasties in the same radial artery, and the potential of DEB angioplasty as a last resort in chronic total occlusion of the radial artery.
Nothing to disclose / No conflicts of interest
HRO008 - Hemostasis & Radial Artery Occlusion
INCIDENCE AND PREDICTORS OF RADIAL FAILURE IN PATIENTS UNDERGOING PCI AT QUEBEC HEART-LUNG INSTITUTE, A TERTIARY HIGH-VOLUME RADIAL CENTRE
Abdelaal E., Brousseau-Provencher C., Montminy S., Plourde G., MacHaalany J., Bataille Y., Déry J.P., Larose E., Delarochellière R., Rinfret S., Roy L., Proulx G., Gleeton O., Rodés-Cabau J., Noël B., Barbeau G., Nguyen C., Costerousse O., and Bertrand O.F.
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
PURPOSE: To determine incidence and predictors of radial access failure, and procedural success rates in consecutive patients undergoing TR-PCI in a high volume tertiary cardiac center (12 staff cardiologists and 7 interventional fellows-residents).
BACKGROUND: Meta-analyses and randomized trials have shown that transradial access (TR), compared to transfemoral (TF), for percutaneous coronary intervention (PCI) and diagnostic procedures significantly reduces access site and bleeding complications. However, TR is associated with a steeper learning curve compared to TF, as well as potentially higher failure rate, resulting in access site crossover in 5-10% of cases.
METHODS: All consecutive patients admitted or referred to our centre for elective, ad-hoc, primary or rescue PCI, were prospectively included in current study. Baseline, procedural characteristics and clinical outcomes were prospectively recorded into institutional database. TR failure was defined as inability to complete PCI procedure via TRA route. Univariate and multivariate analysis were performed to determine independent predictors of TR-PCI failure.
RESULTS: A total of 751 patients underwent PCI during study period, and represents all comers. Mean age was 66 ± 12 years, 23% were females, 26% were diabetic, 32% had prior radial access, 28% had prior PCI, and 13% prior CABG. Of all 751 PCI cases performed during study period, 18 (2.4%) were performed via TF for clinical reasons (prior CABG with bilateral mammary grafts, known Takayasu arteritis, clinically occluded bilateral radial arteries) and 3 via ulnar artery (0.4%) due to clinical RA occlusion. TR was attempted in all remaining 730 (97.2%) cases, and procedure was successfully completed in 712 (97.5%) via initial TR. Eighteen cases (2.5%) required access site crossover, 5 (28%) to contralateral radial, and 13 (72%) to TF. Reasons for TR failure included absent radial pulse or inadequate puncture due to prior radial access (N=10), spasm (N=4), radial or subclavian tortiousity (N=3), and inadequate GC support (N=1). On multivariate analysis, prior PCI was an independent predictor of TR failure (odds ratio [OR] 2.91; 95% confidence interval [CI]: 1.10-7.87, p = 0.032).
CONCLUSION: In a default radial centre, 2.5% of all comers undergoing PCI are excluded from initial TRA on clinical grounds. In our case mix, including those performed by low-volume operators, access-site crossover is required in only 2.5% of the cases. Prior PCI was an independent predictor of TR-PCI Failure. With a team approach in an environment promoting radial as default, TR-PCI success approaches 100% and learning curve is less of an issue.
Nothing to disclose / No conflicts of interest
ACS001 – Radial PCI in ACS
OPTICAL COHERENCE TOMOGRAPHY OF THE RADIAL ARTERY – FIRST EXPERIENCE
Kanovsky J., Poloczek M., Bocek O., Ondrus T., Spinar J., Kala P.
Corresponding author : Jan Kanovsky, MD, Department of Internal Medicine and Cardiology, University Hospital Brno, Jihlavska 20, Brno, 62500, Czech Republic, jkanovsky@fnbrno.cz
PURPOSE: To study the feasibility and safety of the optical coherence tomography (OCT) imaging in the radial artery (RA), which is relatively often hurt or chronically changed after previous interventions.
METHOD: As the use of the Fourier-domain OCT (FD-OCT) for the radial artery imaging was never described in the literature, we tested several protocols how to standardize the RA imaging. There are options of manual vs. pump injection of contrast fluid, 100% contrast fluid vs. 50% diluted contrast fluid and several ways how to map the region of imaging, too.
RESULT: We examined RA in 5 patients with the FD-OCT imaging. We found the best way how to perform the examination in using 100% contrast fluid, injected manually with low pressure. The position of the catheter was adjusted by X-ray contrasting ruler under the right arm. With higher pressure, patients reported pain in the extremity. If diluted contrast fluid was used, the image quality was compromised. No patient suffered from any complication during the procedure. All patients were admitted to the hospital for a planned coronary angiography due to coronary artery disease.
CONCLUSION: We demonstrated the feasibility and safety of the FD-OCT imaging of the RA. The method can be very useful in the research of acute and chronic changes in the RA wall after one or even repeated interventions via the vessel in the past.
Grants / research support: supported by the Grant of the IGA Ministry of Health of the Czech Republic no. NT/13830.
ACS002 – Radial PCI in ACS
BAIL-OUT RADIAL STENTING AS A RESULT OF AN UNSUCCESSFUL CORONARY INTERVENTION – CASE REPORT
Miklik R., Jerabek P., Poloczek M., Bocek O., Kala P.
Corresponding author : Roman Miklik, MD PhD, Internal Cardiology Department, Faculty Hospital Brno, Jihlavska 20, Brno, 62500 Czech Republic. romanmiklik@yahoo.com
We present a case of a 65-year old man, having been treated with diabetes mellitus and hypertension so far, who was admitted with inferior non-STE MI and pulmonary oedema at presentation. The patient was reffered for elective coronary angiography 4 days later. Right radial access site and 6F sheath and catheters were used. The RCA with a series of significant leasions was treated by implantation of 2 DESs. Concerning the LCA, we found M1 to be occluded and decided to intervene this vessel at a time. JL4 6F guide catheter was our choice and hydrophilic Pilot 50 wire easily crossed the leasion.We predilated with 2.0/20 balloon but a biolimus-eluting stent 2.75/18 did not pass through the 90°angle from the main stem (with a calcified 40% distal stenosis) into the LCx. All our effort led to a damage of the proximal part of the stent that could not be pulled back into the guide catheter.We tried to pull back the entire system and almost reached the sheath but could not get any further. We decided to deploy the 2.75/18 stent in that location. The angiographical result of the coronary intervention as well as the X-ray picture of the forced radial stenting looked good.
Unfortunately, 4-hour bandage of the radial access site resulted in compression of the stent as seen on immediate as well as on the 24-month follow-up ultrasound recording. Despite the stent compression, a permeable stent with in-stent and para-stent flow was observed and no signs of stent thrombosis were present, possibly due to a long-period dual antiplatelet therapy. The patient is stable with no right hand movement or sensation consequencies.
Nothing to disclose / No conflicts of interest
ACS003 – Radial PCI in ACS
IS TRANSRADIAL ACCESS FOR PRIMARY PCI AN IMPORTANT BENEFIT IN THE REAL WORLD?
Ratib K(1), Routledge H.C(2), Mamas M.A(3), Arnous S(1), Fraser D(3), Ludman, P.F(4), Nolan J.(1)
1University Hospital of North Staffordshire, UK; 2Royal Worcestershire Hospital, UK; 3Manchester Royal Infirmary, UK; 4University Hospital Birmingham, UK
Corresponding author : Karim Ratib, BSc MB ChB, Cardiology Deoartment, University Hospital of North Staffordshire, Stoke-on-Trent, UK, kratib@mac.com
PURPOSE :Radial access has been shown to reduce mortality and bleeding complications following PCI for STEMI. Using observational data from a large contemporary UK database, real world outcomes of Primary PCI (PPCI) were examined according to access site.
METHODS :This study includes data collected by the British Cardiovascular Intervention Society (BCIS) under the auspices of the National Institute for Cardiovascular Outcomes Research (NICOR). The BCIS database aims to record every PCI procedure undertaken in the UK. All cases recording a single site of either transfemoral (TFA) or transradial (TRA) access, between January 2006 and December 2010, were included in this retrospective analysis. Multiple and other access sites, procedures for cardiogenic shock and those requiring intra-aortic balloon counter-pulsation were excluded. 30-day mortality was tracked using a central registry to which it is a legal requirement that every death in the UK is registered. Cox-hazards regression analysis was used to determine the influence of access site and other variables.
RESULTS : Over the 5-year period 42,134 PPCI procedures were recorded as using a single access site. Mortality at 30 days was 876/23,998 (3.5%) in the TFA group and 324/16936 (1.9%) in the TRA group (p<0.001). There were however significant differences in the baseline characteristics; in the TFA group patients were older (63.3±13.2 vs 62.4±14.5, p<0.001), had more prior by-pass grafts (3.8 vs 1.1%, p<0.001) and were more often ventilated before PCI (1.6 vs 0.8%, p<0.001). The TRA group more frequently received glycoprotein inhibitors (68 vs 73%, P<0.001) and thrombus aspiration (34 vs 48%, p<0.001). Blood transfusions and arterial complications were fewer in the TRA group (0.4% vs 0.1%, p<0.001 and 0.7% vs 0.4% p<0.001) respectively. Following cox-hazards regression, TRA was associated with a HR of 0.71 (95% CI 0.61-0.83, p<0.001) for death at 30-days.
CONCLUSION : In this large real world analysis of UK primary PCI, TRA when compared to TFA is associated with 29% fewer deaths even after adjustment for significant differences in baseline characteristics.
Nothing to disclose / No conflicts of interest
ACS004 – Radial PCI in ACS
EARLY AND LATE CLINICAL OUTCOMES IN ELDERLY PATIENTS AFTER TRANSRADIAL CORONARY STENTING AND MAXIMAL ANTIPLATELET THERAPY
Bagur R, Bertrand OF, Costerousse O, Larose E, Tizon-Marcos H, Nguyen CM, Déry JP, De Larochellière R, Roy L, Poirier P, Rodés-Cabau J
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND: Age is an important determinant of outcomes in acute coronary syndrome (ACS). No data are available on the impact of age on early and late clinical outcomes after transradial PCI and maximal antiplatelet therapy.
METHODS: In the EASY study, 1348 ACS patients underwent transradial PCI. All patients were pretreated with ASA and clopidogrel (90% ≥ 12h). After sheath insertion, 70 U/kg heparin was administered and a bolus of abciximab (0.25 mg/kg) was given prior to first balloon inflation. We compared MACE (death, MI, TVR), major bleeding and local hematomas in patients ≥ 70 and < 70 years at 30 days, 6 months and 12 months.
RESULTS: There were 259 patients (19%) ≥ 70 y in the study. Compared to patients < 70 y, older patients were more often males and smokers (p < 0.0001), had more dyslipidemia (p = 0.01), more hypertension (p = 0.027), more family Hx (p = 0.0003), and more previous CABG (p = 0.0017). In contrast, older patients received less often low molecular weight heparin (p = 0.052) and glycoproteins IIb-IIIa inhibitors (p = 0.01) prior to PCI. Procedure duration was longer in older patients (52 ± 27 vs 48 ± 25 minutes, p = 0.024).
Major bleeding according to REPLACE-2, moderate hematoma : > 5cm, severe thrombocytopenia : < 50,000/mm3
CONCLUSION: Despite more baseline co-morbidities in older patients, early and late outcomes were similar in patients < 70 and ≥ 70 years. Age is not an independent predictor of clinical outcomes after transradial PCI and maximal antiplatelet therapy.
Nothing to disclose / No conflicts of interest
ACS005 – Radial PCI in ACS
IMPACT OF GENDER ON EARLY AND LATE CLINICAL OUTCOMES AFTER TRANSRADIAL CORONARY STENTING AND MAXIMAL ANTIPLATELET THERAPY
H Tyzon, OF Bertrand, J Rodés-Cabau, É Larose, V Gaudreault, JP Déry, P Poirier, O Costerousse, R De Larochellière, L Roy
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND: Female gender has been associated with poorer outcomes after PCI and femoral approach. No data are available on the impact of gender on early and late clinical outcomes after transradial PCI and maximal antiplatelet therapy.
METHODS: In the EASY study, 1348 acute coronary syndrome patients underwent transradial PCI. All patients were pretreated with ASA and clopidogrel (90% ≥ 12h). After sheath insertion, 70 U/kg heparin was administered and a bolus of abciximab (0.25 mg/kg) was given prior to first balloon inflation. MACE (death, MI, TVR), major bleeding and local hematomas were evaluated at 30 days, 6 and 12 months.
RESULTS: Female patients were older (p < 0.0001), had more hypertension (p = 0.004), more family history (p=0.007), and more previous PCI (p=0.016) than males. The weight, baseline hemoglobin, platelets, and creatinine clearance (p<0.0001 for both) were significantly lower in females. The number of dilated sites, type B2/C lesions and procedure duration were similar but sheath size ≥ 6F was less frequent in females (43% vs 56%, p<0.0001). Activated clotting time (ACT) after PCI completion was higher in females (322 ± 71 vs 308 ± 64 seconds, p=0.003). By multivariate analysis, female gender was an independent predictor of moderate hematoma (OR=4.40, 95% CI 2.49-7.81,
p<0.0001).
CONCLUSION: After transradial PCI and maximal antiplatelet therapy, female gender was associated with higher risk of moderate hematoma. Despite more comorbidities female gender was not a predictor of late adverse clinical outcomes.
Nothing to disclose / No conflicts of interest
ACS006 – Radial PCI in ACS
TRANS-RADIAL APPROACH SHOWED FAVORABLE ONE YEAR CLINICAL OUTCOME COMPARED TO TRANS-FEMORAL APPROACH IN ACUTE ST ELEVATION MYOCARDIAL INFARCTION PATIENTS UNDERGOING PRIMARY PERCUTANEOUS CORONARY INTERVENTION
Kedev S, Kalpak O, Dharma S, Antov S, Kostov J, Pejkov H, Spiroski I
Corresponding author : Sasko Kedev, MD,PhD,FESC,FACC, University Clinic of Cardiology, Skopje, Macedonia, Skopje, 1000 Macedonia. skedev@mt.net.mk
BACKGROUND: Vascular access choice is important for acute ST elevation myocardial infarction (STEMI) patients undergoing primary percutaneous intervention (PPCI). The aim of the study was to compare the efficacy and safety of trans radial approach (TRA) with transfemoral approach (TFA) in acute STEMI patients that underwent PPCI in real world practice.
METHODS: All-comers of STEMI patients (N=1855) that underwent PPCI from October 2007 to December 2010 were enrolled and divided to TRA (N=1185) and TFA groups (N=670). The primary outcome was major adverse cardiac event (MACE) defined as composite of death, re-infarction and target vessel revascularization at 30 days and at one year. Major vascular access site complications and non-CABG major bleeding at 30 days were the secondary end points.
RESULTS: At 30 days follow up, MACE occured in 6% of TRA patients and 11% in TFA patients (hazard ratio [HR] 0.53, 95% CI 0.38-0.74; p< 0.001). The lower MACE rate was remained after 1 year follow up in favor for TRA compared to TFA group (10% vs 19%) with HR of 0.55, 95% CI 0.43-0.70; p<0.001. The rate of major vascular access site complications at 30 days were significantly decreased in TRA group compared to TFA group (0.7% Vs 8.2%, p<0.001). The non-CABG bleeding at 30 days was 1.1 % in TRA patients and 4.3% in TFA patients (HR 0.25, 95% CI 0.13-0.48; p<0.001).
CONCLUSIONS:Trans-radial intervention showed favorable clinical outcome with a marked decreased of major vascular access site complications and non-CABG related bleeding rates compared to trans-femoral intervention in Acute STEMI patients undergoing PPCI.
Nothing to disclose / No conflicts of interest
ACS007 – Radial PCI in ACS
ADEQUATE SCREENING CAN REDUCE RADIAL ACCESS FAILURE RATES IN ST-ELEVATION MYOCARDIAL INFARCTION PATIENTS UNDERGOING PRIMARY PERCUTANEOUS CORONARY INTERVENTION
Dery JP, Dery U, Bouchard MP, Roy M, Rodes-Cabau J, Rinfret S, Larose E, Barbeau G, Rouleau J, Roy L, Noel B, Nguyen CM, Gleeton O, Proulx G, Boudreault JR, DeLa Rochellière R, Rao S, Bertrand OF.
Corresponding author : J.P. Dery, Quebec Heart and Lung Institute, Quebec City, Canada.
BACKGROUND: Use of the radial artery (RA) can lower bleeding rates and improve clinical outcomes in STEMI patients undergoing primary PCI. However, cross-over to femoral artery (FA) is often needed to complete the intervention which can lead to longer reperfusion time. We sought to investigate the incidence and reasons for RA failure in a high volume primary PCI center where the RA is the default arterial access.
METHODS: We prospectively collected data on 2502 patients undergoing primary and rescue PCI at a single academic center between May 2006 and June 2011. We excluded 138 (8.6%) patients for whom the FA was the initial access site attempted. Factors associated with cross-over to FA to perform PCI (RA failure) were identified using logistic regression. Use of the FA solely for intra-aortic balloon pump placement was not considered RA failure.
RESULTS: RA failure occurred in 2.4% of patients. Female sex, older age, Killip 4 and need for IABP were factors associated with RA failure. In patients<75 and killip class <4, RA failure was rare (1.6%). Patients with RA failure had 8 min median increase in total arterial access time. The FA was the most popular access site after RA failure (89.2%).
CONCLUSION: In a high-volume transradial center, crossover to femoral approach during primary PCI is lower than reported in the literature and is higher in females, older patients, and those with Killip class 4.
Nothing to disclose / No conflicts of interest
ACS008 – Radial PCI in ACS
IMMEDIATE TRANSRADIAL PERCUTANEOUS CORONARY INTERVENTION ON CULPRIT LESION IN ST-ELEVATION MYOCARDIAL INFARCTION COMPARED TO DIAGNOSTIC ANGIOGRAPHY FOLLOWED BY PRIMARY PERCUTANEOUS CORONARY INTERVENTION IS ASSOCIATED WITH REDUCED DOOR-TO-BALLOON TIMES
Plourde G, Abdelaal E, Bataille Y, MacHaalany J, Déry JP, Déry U, De Larochellière R, Gleeton O, Barbeau G, Roy L, Costerousse O, Bertrand OF.
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
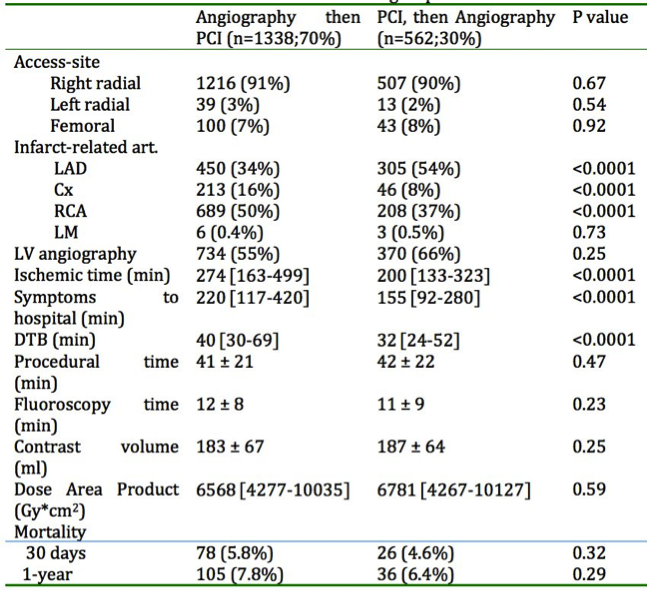 BACKGROUND: Door-to-balloon (DTB) time is an important metric parameter in primary percutaneous coronary intervention (PCI) for acute ST-elevation myocardial infarction (STEMI) to optimize clinical outcomes. Thus, all efforts should be made to reduce it.
BACKGROUND: Door-to-balloon (DTB) time is an important metric parameter in primary percutaneous coronary intervention (PCI) for acute ST-elevation myocardial infarction (STEMI) to optimize clinical outcomes. Thus, all efforts should be made to reduce it.
OBJECTIVE: The aim of this study is to compare the impact of immediate PCI on culprit lesion in STEMI patients versus diagnostic angiography followed by PCI on DTB times and procedural data.
METHODS: Using the catheterization laboratory STEMI database, all patients who underwent primary PCI for an ECG-diagnosed STEMI without prior coronary artery bypass grafting (CABG) surgery were retrospectively considered for inclusion. Procedural data as well as 1-year all cause mortality were assessed in all patients. The primary outcome was DTB time.
RESULTS: From January 2006 to June 2011, we identified 1900 patients. Age and cardiovascular risk factors were similar in the 2 groups.
CONCLUSION: In this study, a strategy of direct PCI of infarct-related artery prior complete coronary angiography was associated with a benefit of 8 minutes in DTB. Further study is required to determine whether this strategy should be preferred, especially in early presenters with acute ST-elevation MI.
Nothing to disclose / No conflicts of interest
LC001 – Learning Curve & Radial Approach
COMPARISON OF RADIATION EXPOSURE BETWEEN EXPERIENCED RADIAL AND FEMORAL OPERATORS : A PROSPECTIVE STUDY.
Faurie B., Abdellaoui M., Bourlard P.
Corresponding author : Benjamin Faurie, MD, Groupe Hospitalier Mutualiste, Grenoble, France. faurieb@gmail.com
PURPOSE: The aim of this study is to compare the level of patient and operator irradiation exposure for coronary angiography (CA)and ad’hoc percutanneous coronary intervention (PCI) between an experienced radial operator and an experienced femoral operator.
METHODS: The two operators are full time senior interventionnal cardiologists. Both have there radioprotection accreditation mandated by the French Society of Cardiology (CATS). The radial operator achivied his learning curve 2 years before this study and performs more than 90% of the procedure throught transradial approach (TRA). The femoral operator is a very experienced operator doing more than 80% of procedure throught transfemoral approach (TFA). Both perform more than 250 PCI per year. We consecutivly analysed 172 all-coming CA and PCI exepted STEMI. 117 cases by TRA and 55 trought TFA. All cases were performed in the same interventionnal room with the same radiation protections for patient and operator. Radiation exposure was assessed by electronic personnal dosimeters for operator exposure and by ionisation chamber for patient exposure.
RESULTS: Patient radiation exposure was the same between TRA and TFA for CA and PCI : 28.2 [7-100.5] Gy/cm2 vs 36.4 [10.4-90.5] Gy/cm2 and 43.2 [12.7-134.6] Gy/cm2; p=0.45 vs 57.1 [12.7-110.5] Gy/cm2; p=0.48, respectively. Similarly, operator exposure was the same between TRA and TFA for CA and PCI : 6.8 [1-45] vs 6.7 [1-18] uSv; p=0.5 and 12.9 [2-51] vs 15.1 [2-64] uSv; p=0.5, respectively.
CONCLUSION: Transradial CA and PCI performed by radial operator lead to same patient and operator radiation exposure as Transfemoral CA and PCI performed by a femoral operator.
Radiation exposure of patient and operator is more influenced by operator way of working than by radial or femoral route for experienced operator.
Nothing to disclose / No conflicts of interest
LC002 – Learning Curve & Radial Approach
IS RADIAL APPROACH APPROPRIATE FOR BEGINNING INTERVENTIONAL CARDIOLOGISTS?
Jaworski L.,Hrabos V.,Sembera Z.,Polasek R. and Horak D.
Corresponding author : Lukas Jaworski, MD, Cardiology Department, District Hospital Liberec, Husova 10, 460 63 Liberec, Czech Republic, Jaworski@seznam.cz
Advantages of radial access (AR) compared to femoral access (AF) were demonstrated in many clinical trials. Larger experience with training of new interventional cardiologists using primarily radial access is still missing. The present work compares both approaches in the hands of beginning interventional cardiologists performing diagnostic cardiac catheterizations. Retrospective analysis of data suggests benefit of radial access.
Fluoroscopic times were comparable (AR vs. AF 5,56 ± 0,24 min/examination vs. 5.75 ± 0.27 min/examination; P=0.699), total times of examinations were significantly shorter (AR vs. AF 21.18 ± 0.59 min/examination vs. 28.06 ± 0.76 min/examination; P≤0.001), contrast consumption was also lower (AR vs. AF 113.95 ± 2.09 ml/examination vs. 145.08 ± 2.83 ml/examination; P≤0.001). The most important difference was in the number of vascular complications (0.5 % in transradial group). Outcomes of analysis indicate that benefit of radial access is apparent even hen performed by interventionalist in training.
Nothing to disclose / No conflicts of interest
LC003 – Learning Curve & Radial Approach
WHAT IS THE PATIENT’S PREFERENCE FOR ARTERIAL ACCESS IN AN ANGIOGRAPHY?
Goldsmit A., Sztejfman C., Chiminela F., Sztejfman M., Bettinotti M.
Corresponding author : Alejandro Goldsmit, MD, Sanatorio Guemes, Fco Acuña de Figueroa 1240 2do sub suelo, Hemodinamia, Buenos Aires, 1180, Argentina. ale.goldsmit@gmail.com
INTRODUCTION : To avoid vasospasm Nalbuphine “N” is the key for the patient (P) not to feel pain when Trans Radial Intervention (TRI) is performed. I conducted a registry to know what the real election of (P) in angiography access is.
METHODS : Registry performed in the first 100 (P), was prospective and consecutive. By single experienced operator during 2012. Before starting TRI all patient received 5 mg “N” I.V. After that, I made the radial puncture by usual techniques (Radiofocus Intro II Terumo Corp. Japan). I never used NTG or verapamil.
Definitions : No spasm: (P) did not experience any pain or discomfort during and immediately after the TRI. Mild: Minimal local pain and discomfort during catheter movement. Moderate: Significant local pain and discomfort during catheter movement. Movement was possible to complete the TRI. Severe: Severe local pain and discomfort during catheter movement compelling the operator to stop the TRI and cross-over to the other route. Very severe: Severe local pain and discomfort associated with catheter trapping. Contraindication for TRI: absence of radial pulse, renal failure, the necessity to use >7 Fr, previous unsuccessful TRI.
RESULTS : 100 (P): Angiography: 5 carotids, 68 coronary, 14 lower limbs, Angioplasty:12 coronary, 1 renal. Left TRI was made in 4 (P), right TRI in 95 and right ulnar in 1. Left TRI for undergone CABG with LIMA and 1 ulnar; radial artery was not palpable.
Patients were divided in two groups, A= 5 Fr introducer with 45 (P), B= 6Fr with 55 (P) Clinical spasm: 5fr group; No=41, mild=2, moderate=1, severe=1, very severe=0. 6 fr group No=53, mild=0, moderate=2, severe=0, very severe=0.
65 (P) were first time in cath lab. 35 (P) had at least 1 previous intervention. TRI=9, femoral=26, TRI and femoral=5. When TRI was done we made a question, whether he had or did not have a previous procedure by femoral or TRI. If you needed a new procedure would you prefer it by TRI or other access? 100% (P) demanded TRI. Every (P) who had already have a femoral access rejected this approach and chose TRI.
CONCLUSION : N reduces spasm and discomfort in the (P). 100% (P) with previous ANG by femoral prefer TRI. 100% of (P) demand TRI. None chooses other access than TRI.
Nothing to disclose / No conflicts of interest
LC004 – Learning Curve & Radial Approach
PROSPECTIVE COMPARISON OF PALPATION VERSUS ULTRASOUND GUIDED RADIAL ACCESS FOR CARDIAC CATHETERIZATION IN AN EXPERIENCED OPERATOR
Zaremski L., Quesada R., Kovacs M., Uthoff H.
Corresponding author : Lynn Zaremski, BA, Division of Clinical Research & Outcomes, Baptist Cardiac & Vascular Institute, Baptist Hospital of Miami, 8900 North Kendall Drive, Miami, Florida, 33176, USA. lzare002@fiu.edu
PURPOSE: To prospectively compare ultrasound vs. palpation guided radial catheterization performed by an experienced cardiac interventionalist.
METHOD: In this prospective single center study, 183 consecutive patients scheduled for transradial cardiac catheterization by an experienced interventionalist were assigned 1:1 to either palpation or ultrasound guided radial access. Demographic and procedure parameters were prospectively recorded.
RESULTS: Baseline demographic and clinical parameters did not differ significantly between the ultrasound (n=92) and palpation (n=91) groups. The initial radial catheterization success rate and time to access did not differ between the ultrasound and palpation groups (87% vs. 86.8%, p=0.977; 47s[interquartile range 20s-90s] vs. 31s[20s-75s], p=0.532, respectively). Pulse quality (absent, weak, strong) was independently associated with access failure in both groups (p< 0.001). Obesity was associated with access failure in the palpation (p=0.005), but not in the ultrasound group (p=0.544). In 3/12 (25%) cases in the ultrasound and 2/6 (33%) cases in the palpation group, the operator was able to establish radial access using the alternative method (p=0.710). If palpation guided radial access failed, an additional ultrasound guided attempt before cross-over to femoral access was associated with a shorter overall time to access (525s[462-567s] vs. 744s[722-788], p=0.016).
CONCLUSION: For an experienced interventionalist, ultrasound guided radial access seems to provide no substantial additional benefit over palpation guided access alone. If palpation guided radial access fails, an ultrasound guided attempt seems to be reasonable before cross-over to femoral access.
Nothing to disclose / No conflicts of interest
LC005 – Learning Curve & Radial Approach
A NOVEL TECHNIQUE TO CROSS ARM TORTUOSITY DURING TRANSRADIAL CATHETERIZATION : THE TWISTING CATHETER.
Faurie B., Abdellaoui M.
Corresponding author : Benjamin Faurie, MD, Groupe Hospitalier Mutualiste de Grenoble, 8 rue Docteur Calmette, 38000 Grenoble, France. faurieb@gmail.com
PURPOSE: Radial or brachial loops and tortuosity are the main cause of transradial approach failure despite high experience. Moreover, crossing these anatomical variations are time consuming, increase contrast volume, radiation exposure, number of wires and costs. We describe here the safety and efficacy of a simple technique to cross tortuosity with a 4Fr or 5Fr diagnostic catheter.
METHODS: Between November 2009 and June 2012, the authors consecutively reported every failure of .035’ J wire progression in the arm and forearm. Then, after withdrawing the .035’ wire from the catheter, we advanced gently a Cordis 4Fr or 5Fr JR4 or a 5Fr Barbeau catheter by turning it clockwise rapidly (twisting technique). If this technique failed, we performed a forearm angiogram through the catheter and then we advanced under fluoroscopy an hydrophylic .035‘ wire or in case of failure, a .014‘ wire.
RESULTS: 80 consecutive patients were involved in this registry. This method was succefull in 49 cases (61%) without any vascular complication. There was 31 failures (39%) of this technique wich were caused by either a moderate tortuosity (90%) in 13 cases (42%); 360° loops in 8 cases (26%) and a radial hypoplasia in 4 cases (13%).These identified tortuosity were successfully crossed with .035’ hydrophilic wire in 13 cases (42%) or with .014’ wire in 13 cases (42%) but couldn’t be crossed in 5 cases (16%): three of these because of a 360° loop and two due to a radial artery hypoplasia. The overall rate of cross-over is 6%. We didn’t encountered any complication in the twisting catheter group. We had only one local hematoma in the «failure group» in a case of a 360° loop wich was succefully crossed after multiple and intense attempt with an .035’ hydrophilic wire. We did not encounter artery dissection or perforation.
CONCLUSION: The twisting catheter technique is a safe and efficacy technique to cross radial and brachial tortuosity without any fluoroguidance or contrast media injection. Important tortuosity and loops are a limitation of this technique.
Nothing to disclose / No conflicts of interest
CO001 – Complex PCI by Radial Approach
SHEATHLESS GUIDE CATHETER IN COMPLEX TRANSRADIAL CORONARY INTERVENTION
Valdesuso R.M., Lacunza F.J., Gimeno J.R.,Garcia J., Hurtado J.A., Pinar E., Valdes M.
Corresponding author : Raul M Valdesuso, MD, PhD, Hospital Universitario Virgen de la Arrixaca, Murcia, 30120, Spain. ravaag@gmail.com
PURPOSE: The Sheathless Guiding Catheter (SGC) (Sheathless Eaucath, Asahi Intecc Co, Japan) has hydrophilic coatings and higher inner lumen than conventional Guiding Catheter, enhancing catheter tractability through tortuous vessels, allowing dealing with radial spasm and performing Coronary Intervention (CI) by radial approach in complex cases. We reported the results of using SGC in complex transradial approach
METHODS: Of a total of 1718 PCI (1423 pts, aged 68 ± 4 years old; 62% males) performed in our catheterization laboratory from January the 1st to February the 29th 2011; 1239 (70%) were performed via radial and 479 (30%) via femoral (229 definitively scheduled for femoral by operator criteria).
RESULTS: Of the 250 cases in which a possible cross-over to femoral was initially planned, 159 were finally performed via femoral approach (109 following operator preferences and 47 for no appropriate Sheathless shape available). In 94 pts, radial approach was performed by using a SGC. Reasons for SGC use were: moderate to severe radial spasm in 29, tortuosity and/or subclavian elongation in 16, proximal radial take-off in 8, insufficient backup or difficulties to coronary engage in 12, and in 26 due to unbalance between radial artery diameter and guide catheter Fr needed for PCI. 99 SGC were employed (44 of 6.5 Fr and 55 of 7.5 Fr.), being Super Power Backup with 58%, the most common curve used, followed by Amplatz left (11%). Successful rate was 100%. 75 left and 31 right coronary (RC) were engaged with SGC. There were 3 left main coronary (LMC), one RC ostium and one coronary sinus (that affected LMC) iatrogenic dissections (5,2%), all resolved with stent implantation. In 8 (8.3%) cases there was an insufficient backup due to back slip of the catheter at radial insertion point that led to the need to active fixation at the wrist.
CONCLUSION: Due to the larger inner calibre and its tractability the SGC diminishes the need to radial to femoral cross over with a high successful rate. The risk of coronary dissection with SGC is not insignificant, technical improvements in order to diminish the stiffness of the catheter tip should be considered seriously by the manufacturers. In complex procedures (chronic occlusions, rotablator, etc) SGC active fixation at the wrist should be considered to avoid back slip of the catheter at the insertion point at the radial artery.
Nothing to disclose / No conflicts of interest
CO002 – Complex PCI by Radial Approach
SIMULTANEOUS RECANALISATION OF CORONARY AND RADIAL ARTERY CHRONIC TOTAL OCCLUSION FROM ULNAR ACCESS – CASE REPORT
Balazs E., Morvay Z., Hausinger P., Ungi I.
Corresponding author : Erika M Balázs, MD, University of Szeged, Department of Cardiology, Szeged, Hungary, Szeged, 6725, Hungary, erika.balazs.szte@gmail.com
Demography, case history: A 59-year-old male patient was suffering from effort angina for 2 years. Echocardiography detected no abnormality. Scintigraphy revealed transient ischaemia in the anterior wall. Risk factors: hypertension, type 2 diabetes mellitus and hyperlipidemia. A positive family history for coronary artery disease was revealed.
Diagnostic coronary angiography: Elective coronary angiography was performed in December 2011 from right radial access revealing proximal LAD occlusion with Rentrop grade 2 retrograde filling from the right coronary artery. The first diagonal branch and the circumflex artery showed non-significant lesions.
LAD CTO recanalisation: The patient was admitted to undergo elective LAD CTO recanalisation in March 2012. Between the two catheterizations his cardiac status did not change, however he complained of right arm numbness and weakness. Allen test was normal but with a faint radial pulse. Due to unsuccessful puncture of the radial artery, the ipsilateral ulnar access was selected for the procedure with a 6F introducer sheath. Angiography demonstrated a 45 mm length of radial artery occlusion with collaterals to the distal cap of the occlusion.
LAD antegrade recanalisation with two drug-eluting stents and kissing balloon dilation of the 1st diagonal branch was performed with good angiographic result.
At this phase, recanalisation of the radial artery was decided considering the symptomatic occlusion.
From the same ulnar access the radial occlusion was successfully passed by a Pilot150 guidewire and with support of an OTW balloon catheter followed by tip contrast injection for proving the intraluminal position. After predilation with a non-compliant balloon, a drug eluting balloon inflation was performed. The final angiogram demonstrated TIMI3 flow in the radial artery. Hemostasis was achieved using manual ulnar compression.
At clinical follow-up the patient is free of cardiac symptoms. His right arm responds well to exertion.
CONCLUSIONS: In case of a chronic radial occlusion, recanalisation from the ipsilateral ulnar artery is feasible in the same setting with a complex coronary intervention. Switching to femoral access is not absolutely justified in case of radial occlusion.
Nothing to disclose / No conflicts of interest
CO003 – Complex PCI by Radial Approach
SAFETY AND EFFICACY OF RADIAL APPROACH DURING ROTATIONAL ATHERECTOMY
Szabó G., Nardai S., Berta B., Édes I., Ruzsa Z., Gellér L., Jambrik Z., Merkely B.
Corresponding author : György Szabó, MD, Heart Center of Semmelweis Univ. of Budapest, Budapest 1122, Hungary. szabogeorgester@gmail.com
PURPOSE: The widespread use of DES stents has initiated a new era of rotational atherectomy, creating a very effective treatment modality for the management of heavily calcified coronary lesions. Rotablations are generally performed via the femoral artery however the use of radial approach may offer important advantages in the prevention of bleeding complications. The aim of our current retrospective analysis is to investigate the safety and feasibility of radial approach during rotational atherectomy.
METHODS: Between 1 January 2008 and 30 June 2010 altogether 92 high risk CAD patients were treated by rotablation at our clinic. During the intervention we have applied the radial approach in 40 patients and in the remaining 52 patients femoral access was used based on the operator’s decision. Follow up information was gathered through outpatient control visits and phone interviews. We compared the overall mortality and ischemia-driven TLR rates of the two patient subgroups. The incidence of cumulative MACE, defined as death, myocardial infarction (MI) and target lesion revascularization (TLR) was assessed. The mean of the clinical follow up time was 9 months, and we have extended the mean mortality follow up to 15.3 months by accessing the patient database of the Hungarian National Health Insurance Fund. The baseline characteristics were assessed by Mann-Whitney U Test, while the follow up information was analyzed by Kaplan-Meier Product Limit Analysis and Log Rank Test.
RESULTS: We found no significant difference in the baseline patient characteristics of the two patient subgroups: the mean age was r:65 vs.f:72 yrs, incidence of diabetes was r:45.0% vs. f:45.1%. The angiography revealed severe coronary artery disease in both subgroups: r:47.5% vs. f:51.6% had three vessel disease. We found no significant difference between the survival rates (p=0.214) of patients treated from different approaches, neither did we find any significant difference in the 9.3 months TLR (p=0.66) and MACE (P=0.09) rates of the two patient groups.
CONCLUSION: Our findings indicate that the efficacy and safety of rotablation from radial puncture is comparable to the use of traditional femoral approach, therefore it may be applied to reduce access-related procedural complications in patients with higher risk of bleeding.
Nothing to disclose / No conflicts of interest
CO004 – Complex PCI by Radial Approach
TRANSRADIAL APPROACH DECREASES IN-HOSPITAL MORTALITY IN PATIENTS WITH CARDIOGENIC SHOCK. A SINGLE-CENTRE EXPERIENCE
Rodriguez-Leor O, Fernandez-Nofrerias E, Carrillo X, Mauri J, Oliete C, Rivas C, Bayes-Genis A
Corresponding author : Oriol Rodriguez-Leor, MD, Unitat Cardiologia Intervencionista, Hospital Universitari Germans Trias i Pujol, Carretera de Canyet s/n, Badalona, 8916, Spain. oriolrodriguez@hotmail.com
Transradial approach (TRA) in percutaneous coronary intervention (PCI) has increased over the past few years. Its use has been shown to decrease mortality compared with the transfemoral approach (TFA) in patients with acute coronary syndrome (ACS). Comparative studies have systematically excluded patients with cardiogenic shock (CS).
METHOD : We carried out a prospective, observational registry study of consecutive patients undergoing emergent revascularization between Feb 2007 and Jan 2012. An analysis of the clinical evolution of patients with CS during hospitalization was performed according to the approach used in the PCI.
RESULTS : Of 1,400 emergency procedures, 122 had CS, 80 underwent PCI by TRA (65.6%) and 42 by TFA (34.3%). The main reason for choosing TFA was the absence of radial pulse (54.9%).
Mortality (64.3% vs. 32.5%, p=0.001), serious access site complications (11.9% vs. 2.5%, p=0.03) and MACE (combination of death, infarction, stroke, serious bleeding, and postanoxemic encephalopathy) (73.8% vs. 43.8%, p=0.001) were greater in TFA patients. In the multivariate analysis, TRA was a independent predictor of mortality (OR 0.39[0.15-0.97]); other independent predictive factors were age ≥ 75 (3.47[1.35-8.92]), previous treatment with diuretics (3.67[1.21-11.12]) and the success of the procedure (0.08[0.02-0.24]).
CONCLUSIONS :In centers with experience, TRA approach for PCI is possible and safe in patients with CS in up to two thirds of the patients. The main cause that prevented the use of TRA was the absence of radial pulse. In the multivariate analysis, TRA was associated with a lower risk of mortality.
Nothing to disclose / No conflicts of interest
CO005 – Complex PCI by Radial Approach
TRANSRADIAL LASER ATHERECTOMY TO REVASCULARIZE COMPLEX CORONARY ARTERY DISEASE
Desai H., Sanghvi K.
Corresponding author : Kintur A Sanghvi, MD FACC FSCAI, Deborah Heart & Lung Institute 200 Trentron Road, Browns Mills, NJ, 8015, USA. sanghvik@deborah.org
PURPOSE : Our objective was to evaluate the feasibility of LASER atherectomy through transradial approach.
METHODS : We retrospectively evaluated all the percutaneous coronary intervention (PCI) performed with intention to treat via transradial approach and, had LASER atherectomy used to cross or debulk a complex CAD.
RESULTS : Out of 730 transradial PCI performed at our institute in last year, 19 patients had LASER atherectomy attempted. Excimer LASER atherectomy was used to cross and debulk complex CADs, including heavily calcified, densely fibrotic and severely stenosed coronary lesions not crossable with smallest profile balloon. Eighteen (94%) of those patients had their procedure completed through same radial access. One elderly female patient could not tolerate the upsizing to a 6 Fr sheath because of severe spasm and was switched to a femoral access. Sixteen of the eighteen patients (88.8%) had successful revascularization (<30% residual stenosis and TIMI III flow in all branches) of their CAD. In two patients despite use of LASER, the target lesion could not be crossed with a smallest profile balloon. Two of the eighteen patients had distal coronary spasm responding to the intra-coronary nitroglycerine injection. There was no other major adverse event.
CONCLUSION : Excimer LASER catheter can be used for transradial PCI of complex CAD with high success rate.
Nothing to disclose / No conflicts of interest
CO006 – Complex PCI by Radial Approach
ROTATIONAL ATHERECTOMY FOR LEFT MAIN CORONARY ARTERY DISEASE BY TRANSRADIAL APPROACH IN OCTOGENARIANS
Dahdouh Z. , Roule V. , Dugué AE. , Sabatier R , Lognoné T. ,Grollier G
Corresponding author : Ziad Said Dahdouh, MD, CHU de Caen/ Cardiology Department/ Avenue cote de nacre, Caen 14000, France. ziad_dahdouh@hotmail.com
PURPOSE: Conventional surgery is still considered the preferred management for left main coronary artery (LMCA) disease; but, when severely calcified which is common in elderly, and the patient is unsuitable for surgery, the interventional cardiologist faces a complex percutaneous coronary intervention (PCI) traditionally approached by femoral access. The aim of this study was to appreciate the safety and effectiveness of transradial PCI with rotational atherectomy (RA) for highly calcified LMCA disease in octogenarians unsuitable for surgical revascularization.
METHODS: The study included 13 consecutive patients ≥80 years of age primary denied by our center's heart team for surgical revascularization and who had undergone stenting with RA for LMCA disease (Rota group) between June 2004 and December 2010. The other group with no need for RA included 29 consecutive octogenarians who were also forbidden for surgery (without Rota group).
RESULTS: In the Rota group, mean age was 83.1 ± 2.3 years. Mean Euroscore was 18.1±12.6 and mean Syntax score was 29.7 ± 7.5. Procedural success was met in 92.3%. Mean follow-up time was 25.7 ± 21.4 months. Overall mortality at the end of follow-up was 23.8%. In the without Rota group, the procedural success was met in 96.6%. There was a percutaneous target lesion revascularization (TLR) in 25% and 11.1% in the two groups with and without Rota, respectively. No difference was detected in terms of overall in-hospital or long term mortality or major adverse cerebral and cardiovascular event (MACCE) including death, non-fatal myocardial infarction, TLR, or stroke during long term follow up. In the univariate Cox regression analysis (which included variables such as sex, diabetes mellitus, previous myocardial infarction, renal insufficiency, left ventricular ejection <40%, distal left main disease, right coronary artery occlusion, and the use of Rotablator), no variable was predictive of the in-hospital and long term all-cause mortality or the long term MACCE.
CONCLUSION: RA followed by stent implantation by transradial approach, when applied to heavily calcified lesions demonstrates to be a safe and effective strategy for the treatment of LMCA disease in octogenarians who were refused for surgery and who represented a high risk population. Indeed, it seems able to preserve durability of vessel patency reducing the risk of death and myocardial infarction for this specific population with heavy basal state.
Nothing to disclose / No conflicts of interest
CO007 – Complex PCI by Radial Approach
TRANSRADIAL VS FEMORAL PERCUTANEOUS CORONARY INTERVENTION FOR LEFT MAIN DISEASE IN PATIENTS > 80 YEARS OF AGE
Bertrand OF, Bagur R, Costerousse O, Rodés-Cabau J.
Corresponding author : Olivier F. Bertrand, MD, PhD, Interventional Cardiology Laboratories, IUCPQ, 2725, Chemin Sainte-Foy, Quebec, Canada, G1V 4G5. olivier.bertrand@crhl.ulaval.ca
BACKGROUND: Little data are available on the immediate and late results of transradial percutaneous coronary intervention (PCI) compared to standard femoral approach in high-risk patients. Our objective was to compare our experience in > 80 years old patients undergoing left main PCI with transradial and femoral approach.
METHODS: This was a retrospective analysis of octogenarians patients treated for left main PCI in our center. In-hospital and late results were assessed.
RESULTS: From 2002 to 2008, one hundred and three > 80 years old patients underwent PCI for left main disease. As per our default practice, 90 (87%) patients were treated by transradial approach and 13 (13%) by femoral approach. Patients were older in the radial group (85 ± 3 years vs 82 ± 3 years, p = 0.0067). All patients were preatreated with aspirin and clopidogrel. Patients received heparin in 90 % of transradial cases and 85% of femoral cases (p = 0.63), bivalirudin in 10% vs 15% (p = 0.63) and glycoproteins platelets inhibitors in 33% vs 23% (p = 0.54), respectively. Patients received 3 ± 2 stents in both groups with no difference in the rate of drug eluting stents (44% vs 69%, p = 0.14). Angiographic success was obtained in 98% vs 92% (p = 0.34) respectively with identical fluoroscopic time (23 ± 15 min vs 23 ± 13 min, p = 0.34) and similar procedure duration and contrast volume. Procedures were performed in 5-6Fr in 93% of radial cases and 85% of femoral cases (p = 0.14). At 30 days, death (6% vs 15%, p = 0.21), myocardial infarction (12% vs 15%, p = 0.67) and revascularization ( 1% vs 0%, p = 1.00) were similar in transradial and femoral cases, respectively. Bleeding requiring transfusion occurred in 14% of radial cases compared to 23% in femoral cases (p = 0.42). At follow-up, cardiac death (17% vs 15%, p = 1.00), MI (23% vs 23%, p = 1.00) and revascularization (11% vs 0%, p = 0.35) remained similar in both groups.
CONCLUSIONS: The majority of high-risk > 80 years old patients with left main disease can be treated by transradial approach with similar acute and long-term results than femoral approach but with less risk of bleeding.
Nothing to disclose / No conflicts of interest
CO008 – Complex PCI by Radial Approach
IS RIGHT RADIAL ACCESS AN ACCEPTABLE APPROACH FOR CORONARY ANGIOGRAPHY IN PATIENTS WITH AN IN SITU LEFT MAMMARY GRAFT?
Y. Louvard, T. Lefevre, T. Unterseeh, H. Benamer, T. Hovasse, O. Tavolaro, P. Garot.
Corresponding author: ICPS, Massy, Quincy, ICV-GVM, Aubervilliers, France. y.louvard@angio-icps.com
PURPOSE: left mammary graft angiography from right radial access is a difficult technique which can be perform safely and quickly after a large experience.
METHODS: from a prospective database of 557 coronary angiographies in patients with at least one mammary graft between Jan 2009 and Oct 2011, we extracted 30 coronary angiography including injection of the Left Mammary graft from right radial access performed by a single operator using this technique for more than ten years. This group was compared to a population of Femoral approaches in the same subset performed by 14 operators (n= 183). Quality of mammary graft angio was attested by an independent reviewer: 1 or 2 respectively for selective or subselective completely diagnostic angio (graft, anastomosis and all distal vessels), 3 for non selective good visualization of graft and partial analysis of distal bed, 4 for graft patency or not diagnosis only.
RESULTS: There are only few differences between the two populations.
CONCLUSIONS: In experienced hands a right radial approach to coronary angiography in patients with an in situ Left Mammary graft seems an acceptable alternative to femoral approach regarding potential reduction of vascular complications.
Nothing to disclose / No conflicts of interest
CO009 – Complex PCI by Radial Approach
WHAT IS THE BEST APPROACH FOR ANGIOGRAPHY OF DOUBLE IN SITU MAMMARY GRAFTS?
Y. Louvard, H. Benamer, P. Garot, T. Unterseeh, C. Gaultier, T. Lefevre.
Corresponding author: ICPS, Massy, Quincy, ICV-GVM, Aubervilliers, France. y.louvard@angio-icps.com
PURPOSE: To compare different vascular access for angiographic assessment of double in situ mammary grafts.
METHODS: from a prospective database of 557 coronary angiographies in patients with at least one mammary graft between Jan 2009 and Oct 2011, we extracted 166 procedures in 153 patients with 2 in situ mammary grafts, in order to compare different approaches (14 operators). Quality of mammary graft angio was attested by an independent reviewer: 1 or 2 respectively for selective or subselective completely diagnostic angio (graft, anastomosis and all distal vessels), 3 for non selective good visualization of graft and partial analysis of distal bed, 4 for graft patency or nt diagnosis only.
RESULTS: we identified 4 approches: systematic double radial approach (n= 4), left radial approach (LR)(n= 12), femoral (F)(n= 105) and right radial (n= 39) approaches. As the quality of right mammary angio was very poor from left radial (11.1% diagnostic), we compared femoral and right radial approaches.
CONCLUSIONS: Regarding its potential advantages, right radial approach is an acceptable alternative to femoral approach for coronary angiography in patients with 2 in situ mammary grafts.
Nothing to disclose / No conflicts of interest
CO010 – Complex PCI by Radial Approach
WHAT IS THE BEST ACCESS FOR ANGIOGRAPHY IN PATIENTS WITH A SINGLE IN SITU LEFT MAMMARY ARTERY GRAFT?
Y. Louvard, G. Ferrante, T. Hovasse, T.Unterseeh, P. Garot, O.Tavolaro, H. Benamer, T. Lefevre.
Corresponding author: ICPS, Massy, Quincy, ICV-GVM, Aubervilliers, France. y.louvard@angio-icps.com
PURPOSE: to compare different vascular access for coronary angiography in patients with a single in situ Left Mammary graft.
METHODS: from a prospective database between Jan 2009 and Oct 2011 of 557 coronary angiography in patients treated with at least one mammary graft, we extracted 341 angiography in patients with one Left Mammary graft (14 operators). Quality of left mammary angiography was assessed by one independent reviewer: 1 or 2 respectively for selective or subselective truly diagnostic angio (graft, anastomosis and distal bed), 3 for non selective good visualization of graft and partial analysis of distal vessels, 4 for graft patency or not diagnosis only. Continuous variables are described as median and interquartile ranges (25th/75th), comparisons are done using non parametric statistics.
RESULTS: we compared Femoral (F)(n= 85), Right (n= 35) and Left Radial (LR)(n= 223) approaches.
CONCLUSIONS: left radial access is the best approach to coronary angiography in patients with a single in situ Left Mammary graft for angiography quality and potential reduction of vascular complications, with the same procedural time and contraste volume as Femoral approach. Right radial approach seems a poor access in this multi operator registry.
Nothing to disclose / No conflicts of interest
CO011 – Complex PCI by Radial Approach
RADIAL VERSUS FEMORAL ACCESS FOR PERCUTANEOUS CORONARY INTERVENTIONS IN PATIENTS WITH CHRONIC TOTAL OCCLUSIONS
G. Ferrante, Y. Louvard, K. Hayashida, H. Benamer, T. Hovasse, T. Unterseeh, P. Garot, T. Lefevre.
Corresponding author: ICPS, Massy, Quincy, ICV-GVM, Aubervilliers, France. y.louvard@angio-icps.com
PURPOSE: Femoral access (FEM) is usually employed in Percutaneous coronary intervention (PCI) for chronic total occlusions (CTO) because this is considered to provide better support, and allows the use of larger diameter guiding catheters.
The aim of this study was to assess whether the use of radial access (RAD), which is typically 6Fr catheter compatible, is comparable to FEM with respect to procedural success for CTO.
METHODS: The study included all consecutive patients undergoing PCI for CTO at 3 tertiary cardiac centres between January 2004 and December 2011. CTO lesions were graded as easy (score of 0), intermediate (1), difficult (2), and “very difficult” (≥3), according to the angiographic J-CTO score. A multivariable mixed effect logistic regression for clustered data was used to assess the impact of RAD on PCI success after adjustment for patient characteristics, lesion difficulty graded by angiographic score, vessel site, procedural techniques.
RESULTS: A total of 1249 patients, median 63 yrs-old (55-72, 25th-75th percentile) undergoing PCI for 1402 CTO were included. RAD was used in 848 (60.5%) lesions. The use of 7Fr (0.8% vs. 6.7%, p
CONCLUSIONS: The use of radial access for PCI of CTO is feasible in the vast majority of lesions and it is associated with a comparable success rate to that achieved using the femoral access.
Nothing to disclose / No conflicts of interest
CO012 – Complex PCI by Radial Approach
BILATERAL TRANSRADIAL APPROACH FOR PERCUTANEOUS CORONARY LNTERVENTION OF CHRONIC TOTAL OCCLUSIONS.
Giusepge Ferrante, Thierry Lefevre, Thomas Hovasse, Hakim Benamer, Yves Louvard.
Corresponding author: ICPS, Massy, Quincy, ICV-GVM, Aubervilliers, France. y.louvard@angio-icps.com
BACKGROUND. Chronic total occlusions (CTOs) are challenging percutaneous coronary intervention (PCI) procedures. Few data is available on the use of transradial approach for PCI of CTOs.
METHODS. From 2007 to 2011 consecutive patients with CTO admitted to a single tertiary cardiac center with operators skilled in transradial PCI were screened. CTO was defined as coronary occlusion of duration > 3 months. Only CTOS requiring a strategy of intentional planned double catheter technique, i.e. controlateral injection and/or retrograde approach, were considered for inclusion in the study. All patients with palpable right and left radial artery were considered eligible and were finally included. Procedural success was defined as the achievement of artery patency after stent implantation with final Thrombolysis in Myocardial Infarction (TIMI) flow 2 or 3. Continuous variables were described as mean and standard deviation or median and 25th-75th percentiles, as appropriate.
RESULTS. A total of 85 patients, 62.6±10.9 yrs-old, 76 (89.4%) males, were enrolled. The occluded vessel was left descending anterior artery in 20 (23.5%) patients, left circumflex-obtuse marginal in 16 (18.8%), right coronary artery/interventricular posterior artery in 49 (57.6%). The guiding catheter size was 7F in 2 cases; in the remainder a 6F guiding catheter was used. No switch to femoral approach for PCI occurred. Retrograde approach was performed in 22 (25.9%) patients, via septal collaterals or epicardial collaterals. Median duration of procedure was 100 min (71-124 min) and median volume of contrast administered was 260 ml (177-356 ml). Procedural success was achieved in 63 (74.1%) patients. In all successful cases a final TIMI flow of 3 was achieved. There were 3 cases of coronary perforation, of which 1 requiring pericardiocentesis. No in-hospital death or major bleeding occurred.
CONCLUSION. Bilateral transradial approach for PCI of CTOs is an effective and safe technique. Transradial PCI training programs should be encouraged.
Nothing to disclose / No conflicts of interest
CO013 – Complex PCI by Radial Approach
GASTROEPIPLOIC GRAFT PCI THROUGHT TRANSRADIAL APPROACH WITH A HYPERSELECTIVE INTUBATED 5FR GUIDING CATHETER : A CASE REPORT.
Faurie B., Abdellaoui M., Voguet S.
Corresponding author : Benjamin Faurie, MD, Groupe Hospitalier Mutualiste, Grenoble, France. faurieb@gmail.com
PURPOSE: We describe here the case of a 70 years old man with severe three vessel disease who underwent a bypass with a LIMA on second diagonal and LAD, a SVG on Marginal and a gastroepiploic on distal RCA. He is also under Warfarin for hypersplenism. He’s hospitalized in ICU for ACS with troponin elevation. EKG showed a RBB and ST depression in inferolateral leads.
We performed the CA through left radial approach as usual for unique left mammary graft. We found a totaly occluded mid-LAD with a good patency of the LIMA graft; a long and calcified stenosis of LCX and first marginal branch. The SVG on this vessel was occluded. RCA was occluded at the proximal part. We then catheterized the coeliac tronk with a 125cm long 5Fr Multipurpose catheter to do a non selective injection of the GE graft that we were able to canulate selectively over a 0.025’ hydrophilic guidewire. The angiogram revealed a short and thight stenosis at the distal anastomosis of this graft. The distal bed was big and dominant and without signicant disease on the PDA and PLA branchs. A 300cm long 0.014’ BHW guidewire was advanced in the diagnostic catheter and through the lesion quite easily leaning in the PLA. Then we exchange the diagnostic catheter for a Cordis 5Fr XB4 guiding catheter over the 300cm BHW. It was the very easy to predilate the lesion and implant a 2.75 by 13mm bare metal stent. A high pressure post-dilatation was performed with a 3mm diameter NC balloon. An excellent angiographic was obtained.
4 days after an intensive medical therapy, we performed a complex intervention with rotational atherectomy and two drug eluting stents on the LCX and marginal through right radial approach.
CONCLUSION: Gastroepiploic graft PCI is feasible and safe through radial approach. Hyperselective canulation with conventional 5Fr guiding catheters can be used to facilitate the procedure.
Nothing to disclose / No conflicts of interest
CO014 – Complex PCI by Radial Approach
FEASIBILITY AND SECURITY OF TRANSRADIAL CORONARY INTERVENTION USING 6.5 FRENCH SHEATHLESS GUIDING CATHETER IN PATIENTS WITH SMALL RADIAL ARTERY: A MULTI CENTER STUDY
Cheaito Radi, M.D., Benamer Hakim, M.D., Louvard Yves, M.D., Mustafic Hazrije, M.D., Derraz Youssef, M.D., Tavolaro Oscar, M.D., Hovasse Thomas, M.D., Gaultier Cedric, M.D., Garot Philippe, M.D., Lefevre Thierry, M.D., Marie Claude Morice, M.D.
1: Europeen Hospital of Paris, La Roseraie, Aubervilliers, France; 2: Private Hospital Jacques Cartier, Massy, France; 3: Private Hospital Claude Galien, Quincy sous senart. France
OBJECTIVES: Radial access is associated with lower major vascular access site complications. However, the small size of the radial artery is a technical limitation. A sheathless hydrophylic coated guiding catheter has recently been introduced which diameter is 1 to 2 French smaller than corresponding sheath. The aim of this study is to investigate the feasibility and the security of using a 6.5 French sheathless guide catheter in patients who have small radial arteries.
METHODS: From March 2009 to February 2012, in 3 French hospitals, 148 consecutive patients were enrolled in this study who underwent transradial approach (TRA) for percutaneous coronary interventions (PCIs) using the 6.5 French sheathless guiding catheter because of small radial artery caliber.
RESULTS: Among the 148 patients enrolled, 252 lesions were treated. There were more female patients in the study (64%). Procedural success using the 6.5 French sheathless guide catheter system was 100% with no cases requiring conversion to a conventional guiding catheter. Multi-vessel interventions for the right and the left coronary arteries in the same procedure were performed in 13 patients (9%). During procedures, adjunctive devices used in this cohort included IVUS (2 patients), 36 bifurcated lesions were treated with a kissing balloon technique among 46 patients undergoing bifurcation PCIs, 1 patient had a saphenous vein bypass graft lesion requiring filter wire placement prior to intervention, 9 patients required rotational atherectomy, thrombus-aspiration catheters has been used in 19 patients, FFR-guided angioplasty in 10 patients, alcohol septal ablation in 3 patients. 9 cases of chronic total occlusion were successfully treated among 10 patients using this hydrophilic catheter. There were no radial artery site complications.
CONCLUSION: The use of sheathless guiding catheter system is a safe and effective method for TRA PCIs in case of small radial artery caliber.
Nothing to disclose / No conflicts of interest
SDD001 – Radial Approach & Same-Day Discharge
RADIAL APPROACH VS FEMORAL WITH 4 FRENCH CATHETERS IN OUTPATIENT DIAGNOSTIC PROCEDURES.
Valdesuso R.M., Gimeno J. R., Lacunza F. J., Garcia J., Hurtado J.A., Pinar E., Valdes M.
Corresponding author : Raul M Valdesuso, MD PhD, Hospital Universitario Virgen de la Arrixaca, Murcia, 30120, Spain. ravaag@gmail.com
PURPOSE: Due to the low rate of vascular complications, it is safe to perform outpatient procedures (less than 4 hours of observation) by Radial approach (Rap) However, not all cardiologists are familiar with Rap. We compare the safety and success rate of outpatient diagnostic procedures (ODP) with 4 Fr catheters via femoral (4Frvf) vs. Rap.
METHODS: We analyzed all procedures performed by Rapp and 4Frvf performed from Jan 2009 to Dec 2011. Patients (pts) with PTCA "ad hoc" were excluded. In the 4Frvf any closure device was used. Outlook 4Fr catheter were used (Terumo® Tokyo, Japan), and contrast injections were performed by flow injection system variable (ACIST CMS System, ACIST Medical Systems, Inc, Minneapolis, MN). Failure was consider the need to change to a higher Fr catheter (in 4Frvf), "cross over" of the initial approach, and major vascular complications (MVC) was consider bleeding with transfusion requiring or/and surgical treatment. ODP was considering whenever the Pts were discharged during 4 hours post procedure.
RESULTS: Of the 4972 procedures performed, 1099 (22%) were included in 4Fvf and 1473 (29%) by Rap (93% with 5 Fr catheters). The success rate was 90% 4Frvf vs 92% Rap (p = ns). The main cause of failure was the crossover by anatomical difficulties in both groups (p = n/s). The MVC were uncommon in both groups (0.03% Rap vs 0.1% 4Frvf (p = n / s). Incidence of Hematoma > 6 cm was higher with 4Frvf (1.27% vs. 0.18% (p<0,01). There were no significant differences in terms ODP between the two groups (99.9% Rap vs 99.8% 4Frvf).
CONCLUSION: ODP with 4Frvf have the same success rate and as low incidence of MVC as Rap and could be a safe alternative in ODA.
Nothing to disclose / No conflicts of interest
SDD002 – Radial Approach & Same-Day Discharge
QUALITY OF LIFE AFTER SAME-DAY DISCHARGE OR OVERNIGHT HOSPITALIZATION AFTER TRANSRADIAL CORONARY STENTING AND MAXIMAL ANTIPLATELET THERAPY. RESULTS OF THE RANDOMIZED EASY TRIAL.
Bertrand OF, Courtis J, Costerousse O, Rinfret S, Larose E, Nguyen CM, De Larochellière R, Roy L, Bagur R, Tizon H, Rodés-Cabau J.
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND : It is unknown whether same-day home discharge after PCI impacts differently health-related quality of life (HRQOL) measures compared to standard overnight hospitalisation.
Objective : To compare early and late HRQOL in acute coronary syndrome (ACS) patients discharged home the same-day (SD) or after overnight hospitalisation (OH) after transradial coronary stenting and maximal antiplatelet therapy in the randomized EASY trial.
METHODS : We administered the Medical Outcomes Study Short-Form Survey (SF-36) at baseline, 1, 6, and 12 months after uncomplicated transradial PCI in patients randomized to SD (n =504) or OH (n = 501). The questionnaire contains 36 items that, when scored, yields 8 domains (physical functioning, role physical, bodily pain, general health, vitality, social functioning, role emotional, and mental health). All patients were pretreated with ASA and clopidogrel (90% > 12h) and received abciximab bolus prior the first balloon inflation.
RESULTS : At baseline, no differences were noted between the 2 groups. After 1 month, significant improvement was observed in 7 domains in both randomized groups (P < 0.05) but no change was detected in the general health domain. The amplitude of improvement was similar in both groups. Between, 1 month and 6 months, further significant (P < 0.05) and similar improvement was observed in role-physical and –emotional and social-functioning domains whereas other domains remained stable until 12 months. There was no change in any domain between 6-months and 12-months.
CONCLUSION: After transradial PCI and maximal antiplatelet therapy in ACS patients, several dimensions of health status improve during the first 6 months of follow-up and remained stable up to 1 year after PCI. The duration of hospitalization after uncomplicated trans-radial PCI has no impact on health recovery.
Nothing to disclose / No conflicts of interest
CR001 – Radial Approach & Controversies
INCREASED RADIATION EXPOSURE IN TRANSRADIAL APPROACH. A REAL DRAWBACK OR AN OBSOLETE PROBLEM?
Skvaril J., Kockova R., Jarkovsky P., Danickova K.
Corresponding author : Jan Skvaril, MD, Department of Cardiology. Catheterization Unit. Military University Hospital Prague, U Vojenske nemocnice 1200, Prague 6-Stresovice, Prague, 16000, Czech Republic. skvaril.jan@tiscali.cz, jan.skvaril@uvn.cz
OBJECTIVE: Transradial approach (TRA) in cardiac catheterization has become increasingly popular. Beside many advantages (reduction of bleeding complications, early ambulation, lower costs), it contains the controversy concerning possibly increased radiation exposure. This statement, however, has significant flaws. Without beeing a method of choice and practiced by transfemoral specialists or physicians without sufficient learning curve only as an alternative approach, it may be associated with prolonged fluoroscopy time. This, however, is neither comprehensive nor a decisive indicator. In our cathlab, we use TRA as a method of choice since 2006 with preference of left side (TRA-L). The objective of the study was to compare left radial (TRA-L), right radial (TRA-R) and femoral (TFA) approaches concerning total time, fluoroscopy time, radiation exposure of patients as well as of physicians.
METHODS: 456 patients were prospectively randomized to TRA-L (154) , TRA-R (159) or TFA (143). 5 physicians of different levels of erudition participated in the study. Procedural time, fluoroscopy time, dose-area product (DAP) as patient´s exposure and physician´s equivalent dose, measured with personal electronic dosemeter, were evaluated. Separately for diagnostic procedures and interventions.
RESULTS: TRA-L diagnostic procedures were performed in the same time as TFA precodures (15.5±7.0 min vs. 15.0±9.0 min) and in the same fluoroscopy time (3.56±2.6 min vs. 4.9±6.53 min) without any differnces in PCIs as well. Similarly, no differences between TFA, TRA-R and TRA-L were found in patients´ exposure either in diagnostics (24.49±25.4 Gy.cm2 vs. 27.46±28.86 Gy.cm2 vs. 27.30±19.59 Gy.cm2 , p = 0.210), or PCIs (35.18±63.35 Gy.cm2 vs. 45.75±70.11 Gy.cm2 vs. 47.05±48.66 Gy.cm2, p= 0.990). The physician´s exposure was then the lowest in TRA-L both in diagnostics (19.01±23.85 uSv vs. 22.21±29.84 uSv vs. 14.95±17.01 uSv, p
CONCLUSION: Radial access is safe and effective. As a method of choice, performed routinely with sufficient learning curve and in view of radiation safety it is not associated with increased radiation exposure either of patients or of performing physicians. Established TRA-L provides the optimal results.
Nothing to disclose / No conflicts of interest
CR002 – Radial Approach & Controversies
CATHETERIZATION OF LEFT MAMMARY ARTERY VIA RIGHT RADIAL ARTERY – NEW METHODOLOGY
Coufal Z.
Corresponding author : Zdenek Coufal, MD, Cardiology department, Internal Clinic, Bata Regional Hospital, Inc., Havlickovo nabrezi 600, Zlin, 762 75, Czech Republic. dr.zdenek.coufal@gmail.com
Transradial access is more and more widespread. Sometimes there are cases to display left internal mammary artery (LIMA) catheterization artery used as bypass when no transfemoral access is possible and left radial access is disabled (no radial pulsation, left radial artery used as aterial graft etc.) or patient refuse transfemoral accress. We describe a method for safe LIMA cathetrization via right radial access.
In patients with common left subclavian artery take off (from summit of aortic arch) is easy to reach left subclavian artery ostium and cathetrization of LIMA by JR4 or IMA shape catheter inserted to left subclavian artery by using of 0.025“ wire.
In case of caudal (inferior) ostium of left subclavian artery wire sinks to descending aorta. At this case we use mother-and-child technique: left subclavian artery take-off is reached by 6F guiding catheter XB3,5 or XB4 (extra back up). Conector of standart long guiding catheter is cut by scalpel of approx. 20 cm (8“). Through this guiding support is very easy to insert 0.025“ wire to deep left brachial artery. Over this wire is very easy to insert 4F diagnostic IMA of JR4 catheter up to LIMA take off.
Time to reach LIMA ostium via right radial artery is very short. This technique is alternative to left radial approach or to unfeasible left radial approach.
This method was 100% successfull in our cathlab.
Nothing to disclose / No conflicts of interest
CR003 – Radial Approach & Controversies
SAFETY OF TRANSRADIAL LEFT-HEART CARDIAC CATHETERIZATION IN PATIENTS WITH END-STAGE LIVER DISEASE
Singh V., Jacobs E., Damluji A., Martin P., Alfonso C.E., Moscucci M., Cohen M.G.
Corresponding author : Vikas Singh, MD, University of Miami Miller School of Medicine, Miami, Florida, 33136 USA. vikas.dr.singh@gmail.com
BACKGROUND: Patients with end-stage liver disease (ESLD) are at increased bleeding risk due to coagulopathy and thrombocytopenia. Pre-transplant workup frequently requires cardiac catheterization. Transradial access is associated with less bleeding than femoral access. We sought to investigate the safety of transradial cardiac catheterization in patients with ESLD.
METHODS: Consecutive patients with ESLD who underwent cardiac catheterization via transradial access between 2/08 and 7/10 were included in this study. The primary outcome measure was major bleeding, defined as a decrease in hemoglobin of more than 3 g/dL, or a bleed associated with the need for transfusion of 2 or more units of packed red blood cells within 24 hours of the procedure.
RESULTS: A total of 81 patients were enrolled in the study. The mean age was 59 ± 8 years, and 58% were male. The average MELD score was 18.6 ±7 and baseline hemoglobin was 10.8 ± 1.74 g/dL. The mean baseline INR was 1.53 ± 0.43 and platelets were 93,000 ± 62,000. Major bleeding occurred in 4 patients (4.9%). Procedural related major bleeding occurred in 3 patients (3.6%), however none of these were related to the radial arterial site. There were two venous access site bleeds, and one genitourinary bleeding event during the post-procedural period. One patient developed a hemoglobin drop > 3 g/dL without a specific bleeding site. Out of the entire cohort, four patients (4.9%) expired during hospitalization due to progression of liver disease, and none of these deaths were attributable to complications of catheterization.
CONCLUSIONS: Transradial cardiac catheterization is feasible and appears to be safe in a severely ill population of patients with high bleeding risk and ESLD awaiting transplant.
Nothing to disclose / No conflicts of interest
CR004 – Radial Approach & Controversies
PATIENT SATISFACTION: COMPARING RADIAL VERSUS FEMORAL CATHETERIZATIONS
Speiser B and Bochenek-Cobb L
Corresponding author : Bernadette S Speiser, MSN CCRN CMS, Jesse Brown VA Medical Center/ 820 South Damen Avenue, Chicago, Illinois, 60612 USA. Bernadette.Speiser@va.gov
PURPOSE : Completing the heart catheterization through the arm offers immense satisfaction for the patient. Patients have identified the radial approach decreases back pain, provides prompt mobility, assists in decreasing respiratory effort and allows them to view their access site. The purpose of our study was to compare patients who had both femoral and radial catheterizations, subsequently identify preferences over access sites.
METHODS : At the Jesse Brown VAMC we conducted a questionnaire survey for all catheterization patients. Data was collected to identify patients who had received their catheterization via the femoral approach in the past. Those who had femoral catheterizations were placed in our study group. The study group was sent for catheterization and if a radial approach was utilized, the patients completed the survey. A total of 112 patients participated in the questionnaire.
 RESULTS : Of the 112 that participated in the questionnaire, 93% preferred the radial approach over the femoral approach (7%). The variable most commonly stated as the rationale for the preferred radial approach stemmed around the ability for the patient to immediate sit up after the procedures (66%) (See figure 1). Also the varibles of less pain (22%) and a simpler procedure (11%) were selected as positive radial rationales/ An overpowering number (95%) of patients stated they would recommend this approach to others (See figure 2). If you combined comfort variables for radial vs. femoral, it is an overwhelming 89% in favor of the radial approach
RESULTS : Of the 112 that participated in the questionnaire, 93% preferred the radial approach over the femoral approach (7%). The variable most commonly stated as the rationale for the preferred radial approach stemmed around the ability for the patient to immediate sit up after the procedures (66%) (See figure 1). Also the varibles of less pain (22%) and a simpler procedure (11%) were selected as positive radial rationales/ An overpowering number (95%) of patients stated they would recommend this approach to others (See figure 2). If you combined comfort variables for radial vs. femoral, it is an overwhelming 89% in favor of the radial approach
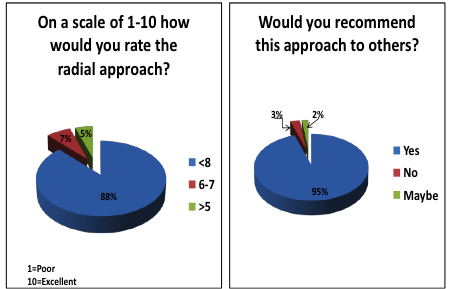 CONCLUSIONS : Increased comfort and mobility are the driving forces for radial access. Patient satisfaction can drive patients toward facilities that perform more progressive radial catheterization and interventions. Communities vie for patients and therefore the radial option may persuade patients to seek one hospital center that does radial angiography over the facility that only offers femoral angiography. Hospitals are measured by national patient satisfaction surveys. If a patient perceives their comforts were addressed, this may skew satisfaction scores toward facilities performing radial procedures.
CONCLUSIONS : Increased comfort and mobility are the driving forces for radial access. Patient satisfaction can drive patients toward facilities that perform more progressive radial catheterization and interventions. Communities vie for patients and therefore the radial option may persuade patients to seek one hospital center that does radial angiography over the facility that only offers femoral angiography. Hospitals are measured by national patient satisfaction surveys. If a patient perceives their comforts were addressed, this may skew satisfaction scores toward facilities performing radial procedures.
Nothing to disclose / No conflicts of interest
CR005 – Radial Approach & Controversies
DOES A NATIONWIDE CHANGE IN ACCESS SITE FOR PCI INFLUENCE NEUROLOGICAL COMPLICATIONS?
Ratib K(1), Routledge H.C(2), Mamas M.A(3), Arnous S(1), Fraser D(3), Ludman, P.F(4), Nolan J.(1)
1University Hospital of North Staffordshire, UK; 2Royal Worcestershire Hospital, UK; 3Manchester Royal Infirmary, UK; 4University Hospital Birmingham, UK
Corresponding author : Karim Ratib, BSc MB ChB, Cardiology Department, University Hospital of North Staffordshire, Stoke-on-Trent, UK. kratib@mac.com
PURPOSE : To assess the incidence of neurological complications following PCI during a 5-year period during which radial access became the major access route across the UK. METHODS : This study includes data collected by the British Cardiovascular Intervention Society (BCIS) under the auspices of the National Institute for Cardiovascular Outcomes Research (NICOR). The BCIS database aims to record every PCI procedure undertaken in the UK. A retrospective analysis was performed between January 2006 and December 2010. Cases recording a single access site, either transfemoral (TFA) or transradial (TRA) were included. Multiple and other access sites, procedures for cardiogenic shock and those requiring intra-aortic balloon pump (IABP) were excluded. We compared the two cohorts of TRA or TFA and used stepwise multivariate analysis to adjust for measured confounding factors. A neurological complication (NC) was defined as a haemorrhagic stroke, ischaemic stroke or transient ischaemic attack.
RESULTS : During the 5-year period a total of 370,238 procedures were recorded. After excluding shock, IABP use and other or multiple access sites, there were 338,214 procedures with 122,818 procedures in the TRA only group and 215,396 in the TFA only group. TRA use increased from 17.3% in 2005 to 51.7% in 2010. Incidence of recorded NC increased from 0.06% in 2006 to 1.1% in 2010 with increases in PCI for ACS from 46.7% 2006 to 60.5% in 2010. There were significant differences between the two cohorts in demographics and clinical factors. Following multivariate analysis independent predictors of a NC were; Previous stroke (OR 3.43, 95% CI 2.30-5.13, p
CONCLUSIONS : Over a period of rapid change in national access site practice, TRA was not associated with an increased risk of NC.
Nothing to disclose / No conflicts of interest
CR006 – Radial Approach & Controversies
CAN WE SAFELY SWITCH FROM THE RADIAL TO IPSILATERAL ULNAR ARTERY APPROACH AND VICE VERSA IN THE SAME SETTINGS AFTER THE PRIMARY FOREARM APPROACH HAS FAILED? REPORT OF TWO CASES FOR “PRO”
Stajic Z., Dincic D., Romanovic R., Tavciovski D., Mijailovic Z., Vucinic Z.
Corresponding author : Zoran S Stajic, MD, Military Medical Academy, Clinic of Cardiology, Belgrade, Serbia, Belgrade, Serbia, 11070. zoran0312@yahoo.com
PURPOSE: To support the evidence that an ipsilateral forearm artery approach may be the safe and effective in the same settings in cases when the primary forearm approach has failed.
METHODS: Report of two cases of successful coronary angiographies performed through the secondary ipsilateral forearm approach in the same setting after the failure of primary ipsilateral forearm attempt.
RESULTS: Case No 1. A 49-year-old patient was referred to our hospital for coronary angiography due to the dynamic ST-T changes recorded on ambulatory ECG. After both modified Allen’s tests were assessed as positive, we decided to perform coronary angiography through the right radial artery approach which is the standard access site in our Cath Lab. Radial artery was easily cannulated but there was a resistance felt during the advancement of the diagnostic catheter, so we performed angiography of the forearm which revealed that the right radial artery was of a small-diameter and the right ulnar artery was a dominant one. The procedure was continued with the right ulnar artery cannulation and successful completion of coronary angiography through this approach.
Case No 2. A 46-year-old patient was admitted due to the symptoms of new-onset pectoral angina. He was allergic to Aspirin. The right ulnar pulse was stronger than the radial so we chose the right ulnar artery as the primary access site for coronary angiography. Although it was easily cannulated, introduction of the sheat caused strong diffuse spasm of the right ulnar artery that did not relieve even after application of vasodilators. So we immediately switched to the right radial artery cannulation and successfully completed the coronary angiography through this approach.
In both cases sheats were removed immediately after completion of the procedure and hemostasis was secured with two TR-bands placed over cannulation sites for 4 hours. Radial and ulnar pulses were regularly checked overnight and they were normal. Control Doppler-echosonography confirmed normal flow patterns in both arteries 24 hours later. No signs of hand ischemia were noted during one month follow-up.
CONCLUSION: In both reported cases secondary ipsilateral forearm approach during the same settings after the failure of the primary ipsilateral forearm approach was safe and effective alternative option which maintained the advantages of the forearm approach. There were no signs of hand ischemia during one month follow up.
Nothing to disclose / No conflicts of interest
CR007 – Radial Approach & Controversies
RIGHT UPPER EXTREMITY POSITION AND OPERATOR RADIATION EXPOSURE DURING RIGHT RADIAL ACCESS CORONARY ANGIOGRAPHY?
Pancholy SB, Boruah P, Ahmed I, Patel TM
Corresponding author : Samir B Pancholy, MD, The Wright Center for Graduate Medical Education, North Penn Cardiovascular Specialists, 401 N State Street, Clarks Summit, PA 18411, USA. pancholys@gmail.com
PURPOSE: The objective of this study was to compare operator radiation exposure using two commonly used positions of the right upper extremity while preparing the patient for right radial access coronary angiography.
METHODS: 117 consecutive patients undergoing diagnostic coronary angiography were randomized to Group I whose right arm was placed in an abducted position at 90 degree angle to the trunk, and Group II whose right arm was placed parallel to the patients trunk, while performing coronary angiography. Demographic, morphologic and radiographic data were recorded which included age, gender, height, weight, number of angiogram runs, air kerma, and dose-area product. Operator radiation exposure was measured using Instadose ion-chamber personal dosimeter worn by the operator outside the lead apron on the vest.
RESULTS: No significant differences between age, gender, and height were noted between group I and II. Weight and number of angiogram runs were significantly higher in Group I. Air Kerma, Dose area product and Operator exposure were “normalized” by dividing each of these variables by number of angiograms and body weight, generating “adjusted air kerma”, “adjusted DAP” and “adjusted operator exposure”. No significant differences were noted between Group I and II in adjusted Air Kerma (Group I: median = 0.47 mGy/run/Kg, IQR 0.31-0.60 vs Group II: median = 0.41 mGy/run/kg, IQR 0.29-0.66, P = 0.56 ), adjusted dose-area product (Group I: median = 38.19 mGy*cm2/run/kg IQR 27.88-51.86, Group II: median = 32.75 mGy*cm2/run/kg, IQR 24.23-52.27, P = 0.28), and fluoroscopy time (Group I: median = 4.5 minutes, IQR 2.05-9.0, Group II: median = 3.4 minutes, IQR 2.2-5.9, P = 0.35). Adjusted operator radiation exposure was significantly higher in Group II compared to Group I (Group I: median 0.15 mREM/run/kg, IQR 0.11 – 0.19, Group II: median = 0.45 mREM/run/kg, IQR 0.37 – 0.54, P = 0001).
CONCLUSION: The position of right upper extremity during right radial access coronary angiography, has a significant independent impact on operator radiation exposure, with the abducted position increasing operator exposure by nearly three-fold.
Nothing to disclose / No conflicts of interest
NC001 – Radial & Non-Coronary Intervention
THE EFFECTIVENESS AND SAFETY OF ALCOHOL SEPTAL ABLATION PERFORMED TRANSRADIALY
Brtko M., Polansky P., Stasek J., Bis J., Vojacek J., Dusek J., Tuna M., Praus R., Jakl M.
Corresponding author : Miroslav Brtko, MD PhD, University Hospital, Dept. of Cardiac Surgery, Sokolska street 581, Hradec Kralove, 500 05, Czech Republic. brtkom@seznam.cz
PURPOSE: Alcohol septal ablation (ASA) is together with septal myectomy respected method of treatment in patients with hypertrophic obstructive cardiomyopathy (HOCM). There are only scarce experiences using transradial approach in ASA. The purpose of the study was to evaluate acute and mid-term results of ASA performed transradially.
METHOD: ASA was performed from the right radial artery, pacemaker lead was inserted using subclavian approach, the left ventricle pressure was measured by pigtail catheter inserted transfemoraly. Actual changes in ultrasonography (US) and catetherization parameters as well as changes in clinical status were observed and the patients were followed-up.
RESULTS: From 2006 to 2011 48 ASA were performed in 43 patients (27 male, 16 female). In 5 patients (11.6%) ASA was repeated because of persisting gradient and significant symptoms. Primary success was achieved in 95.8% of patients. Maximal US gradient decreased after ASA from 61.7 mmHg to 30.9 mmHg (p=0.001), US provoked gradient from 120.7 mmHg to 44.7 mmHg (p<0.001), peak catheterization gradient from 40.0 mmHg to 12.6 mmHg (p<0.0001), provoked peak catheterization gradient from 117.8 mmHg to 43.8 mmHg (p<0.0001) and systolic pressure in arteria pulmonalis (AP) from 35.9 mmHg to 28.7 mmHg (p<0.0001). The interventricular septum (IVS) thickness decreased after 3 months from 19.4 mm to 17.3 mm (p<0.001) and at the site of ablation to 10.5 mm (p<0.0001). There were no changes neither in the thickness of left ventricle posterior wall (LVPW) nor in the left atrium (LA) diameter. After 3 months there was additional decrease of US gradient to 28.1 mmHg (p=0.002), decrease of NYHA class from 2.6 to 1.5 (p<0.0001), the severity of mitral regurgitation was diminished from 2.2 to 1.4 degree (p<0.0001) and ejection fraction (EF) of the left ventricle decreased from 70.4% to 68.2% (p=0.0001). During mid-term follow-up (29.6 months in average) additional significant decrease of US gradient and thickness of IVS were seen. During follow-up a positive clinical effect of ASA lasted in all patients. The patient survival was 90.7%.
CONCLUSION: ASA performed transradialy is effective and safe method of treatment in patients with HOCM. Significant reduction of gradient, pulmonary pressure, symptoms and severity of mitral insufficiency were seen after this procedure. The IVS thickness and EF significantly decreased 3 months post procedure. There were no changes in LVPW thickness and LA diameter during mid-term follow-up and a positive clinical effect persisted in all patients.
Nothing to disclose / No conflicts of interest
NC002 – Radial & Non-Coronary Intervention
THE TRANSRADIAL APPROACH FOR CAROTID ARTERY STENTING
Etxegoien N., Rhyne D., Kedev S., Sachar R., Mann T.
Corresponding author : Nikki Etxegoien, BS, Wake Heart & Vascular, 3000 New Bern Ave Suite G-100, Raleigh NC, 27610, Raleigh, NC 27610, USA. netxegoien@wakeheartresearch.com
PURPOSE: Carotid artery stenting(CAS) is an alternative to carotid endarterectomy(CEA) for revascularization of the internal carotid artery(ICA). CAS from the femoral approach may be problematic due to peripheral vascular disease, anatomical variations of the aortic arch, and access site complications. The purpose of the present study was to evaluate the right radial approach(RRA) for CAS.
METHODS: A retrospective analysis of all pts who had undergone transradial (TR) CAS at two centers was performed. Demographics, the technique used to deploy the sheath in the common carotid, procedural aspects, results, and complications were evaluated.
RESULTS: CAS was attempted from TR in 382 pts(mean age 68, 70% male). Comorbid conditions increasing the risk of CEA were present in 302(79%) and 172(49%) were symptomatic. CAS was successful in 347/382 (91%) pts; 201/216 (93%) right CA, 14/16 (88%) bovine left CA, 132/150 (88%) left CA. The initial diagnostic catheter for RCA was Simmons 1 (39%) or Simmons 2(more acute angle) (39%); for bovine left CA an Amplatz R2 (36%) or Simmons (more vertical takeoff) (29%); and for non-bovine left CA a wire-braided Simmons 2 or 3 (77%). The diagnostic catheter was then exchanged for a 5F (26%) or 6F (69%) sheath or 7F guide (5%) over an .035” standard (17%) or Amplatz superstiff guidewire (73%). In more recent cases, a one-step method advancing a TAD II guidewire directly into the external for shuttle sheath exchange was utilized (6%). Seven different carotid artery stents (51% Xact) and 7 different distal embolic protection devices were used. Adverse events included 2 major strokes (0.6%) one of whom died, 3 minor strokes (1%), and no myocardial infarction at 30 days. No bleeding complications occurred although 23 (6%) of patients had asymptomatic post-procedure radial occlusion. Inadequate catheter support at the origin of the CCA was the technical cause of failure in the unsuccessful cases which were then completed from femoral access as part of the same procedure.
CONCLUSION: The present study describes a consistent TR technique for successful CAS. The transradial approach is an alternative for CAS in the presence of factors that increase the risk or difficulty of femoral access.
Nothing to disclose / No conflicts of interest
WW001 – Radial Approach in the World
DOES ACCESS SITE INFLUENCE MORTALITY FOLLOWING PCI - A RETROSPECTIVE ANALYSIS OF THE BRITISH CARDIOVASCULAR INTERVENTION SOCIETY PCI DATABASE.
Ratib K(1), Routledge H.C(2), Mamas M.A(3), Arnous S(1), Fraser D(3), Ludman, P.F(4), Nolan J.(1); 1University Hospital of North Staffordshire, UK; 2Royal Worcestershire Hospital, UK; 3Manchester Royal Infirmary, UK; 4University Hospital Birmingham, UK
Corresponding author : Karim Ratib, Cardiology Department, University Hospital of North Staffordshire, Stoke-on-Trent, UK. kratib@mac.com
PURPOSE : Transradial access (TRA) for PCI may be associated with lower mortality, however constructing appropriately powered randomised studies to investigate this further is fraught with difficulties. Using real world data from the UK national database, differences in mortality between TRA and transfemoral access (TFA) were examined.
METHODS : This study includes data collected by the British Cardiovascular Intervention Society (BCIS) under the auspices of the National Institute for Cardiovascular Outcomes Research (NICOR). The BCIS database aims to record every PCI procedure undertaken in the UK. A retrospective analysis was performed for cases undertaken between January 2006 and December 2010, including every procedure using either radial or either femoral access. Mixed access, other access sites and missing data were excluded. 30-day mortality was tracked using a national central registry to which it is a legal requirement that every death in the UK is registered. Cox-hazards regression analysis was used to assess influence of access site and other recorded factors.
RESULTS : Over the 5-year period, 370,238 procedures were recorded. 223,476 (60.4%) used TFA and 124,616 (33.7%) TRA. Data were missing or excluded in 22,146 (6%). Between 2006 and 2010 use of TRA increased from 17.1% to 50.8%. 30-day mortality was 1.9% in the TFA group and 1% in the TRA group (p < 0.001). The number of patients presenting with cardiogenic shock was significantly higher in the TFA group (2.1% vs 0.9%, p<0.001). In PCI for stable patients there was no statistically significant benefit observed for TRA (HR 0.83, CI 0.65-1.05; p=0.11). In non-primary acute coronary syndrome and Primary-PCI procedures TRA was associated with a reduction in 30-day mortality (HR 0.69 CI 0.62-0.77, p<0.001 and HR 0.59 CI 0.53-0.67, p<0.001). With shocked and intra-aortic balloon pump (IABP) treated patients excluded, TRA remained independently associated with a reduction in 30-day mortality (HR 0.73, CI 0.67-0.80: p<0.001).
CONCLUSION : TRA for PCI is associated with a reduction in 30-day mortality. The greatest effects are observed following PCI in the acute setting.
Nothing to disclose / No conflicts of interest
WW002 – Radial Approach in the World
DOES CENTRE VOLUME OF TRANSADIAL ACCESS INFLUENCE OUTCOME? DATA FROM THE BRITISH CARDIOVASCULAR INTERVENTION SOCIETY
Ratib K(1), Routledge H.C(2), Mamas M.A(3), Arnous S(1), Fraser D(3), Ludman, P.F(4), Nolan J.(1)
1University Hospital of North Staffordshire, UK; 2Royal Worcestershire Hospital, UK; 3Manchester Royal Infirmary, UK; 4University Hospital Birmingham, UK
Corresponding author : Karim Ratib, BSc MB ChB, Cardiology Department, University Hospital of North Staffordshire, Stoke-on-Trent, UK. kratib@mac.com
PURPOSE : Transradial access (TRA) for PCI may be associated with lower mortality than transfemoral access (TFA) but randomised studies have not demonstrated this consistently. The expertise with TRA at each centre is likely to exert an important influence. We investigated the difference in mortality between hospitals that use majority TRA with those that use mainly TFA for PCI.
METHODS : This study includes data collected by the British Cardiovascular Intervention Society (BCIS) under the auspices of the National Institute for Cardiovascular Outcomes Research (NICOR). The BCIS database aims to record every PCI procedure undertaken in the UK. A retrospective analysis was performed including procedures undertaken between January 2006 and December 2010 where a single access, either radial or femoral were recorded. Multiple or brachial access sites, procedures for cardiogenic shock and those requiring intra-aortic balloon counter-pulsation were excluded. We compared procedures undertaken at hospitals with >50% TRA to those performed at hospitals with >50% TFA. 30-day mortality was tracked using a national central registry; it is a legal requirement in the UK that all deaths are registered. Multivariate logistic regression was used to adjust for measured confounding factors.
RESULTS : 338,214 procedures from 111 hospitals were included in the analysis. 38/111 hospitals used TRA for >50% of procedures. In these mainly TRA hospitals 98,545 procedures were recorded with an overall 70.1% TRA rate. In the mainly TFA hospitals (73/111 institutions), 239,669 procedures were recorded with a 22.4% TRA rate. 30-day mortality following TRA procedures in mainly TRA hospitals was 447/69045 (0.6%) and 514/5773 (1%) for TRA procedures in mainly TFA hospitals (p<0.001). Following multivariate analysis TRA in a mainly TRA hospital remained associated with a reduction in mortality (OR 0.81, 95% CI 0.70-0.92, p=0.002). 30-day mortality for TFA procedure in mainly TFA hospitals was 2105/185896 (1.1%) and 276/29500 (0.9%) for TFA procedures in mainly TRA hospitals (p=0.003). Following multivariate analysis TFA in a mainly TRA hospital was associated with a reduction in mortality (OR 0.86, 95% CI 0.76-0.99, p=0.032).
CONCLUSION : In this retrospective observational study, one third of all UK hospitals use predominantly TRA. TRA procedures performed in these hospitals are associated with a 19% lower 30-day mortality than that observed for TRA procedures in predominantly TFA hospitals. TFA procedures performed in mainly TRA institutions were not associated with worse outcomes.
Nothing to disclose / No conflicts of interest
WW003 – Radial Approach in the World
THE CURRENT EXPERIENCE WITH RADIAL APPROACH IN MACEDONIA
Kedev S, Antov S, Kalpak O
Corresponding author : Sasko Kedev, MD,PhD,FESC,FACC, University Clinic of Cardiology; University St Cyril and Methodius – Skopje, Macedonia, Skopje 1000, Macedonia. skedev@mt.net.mk
Republic of Macedonia is located in Southeastern Europe with population of approximately two million inhabitants. There are four active PCI centers with six cath labs performing overall 3200 PCI’s annually (1600 PCI per million people). Two of them are public (one academic and one non-academic) and 2 are non-academic private centers. Most of the procedures (78%) are performed at the University Clinic of Cardiology in Skopje. That is the only academic center with three cath labs facility where 7 interventional cardiologists are performing 2500 PCI’s out of 4800 diagnostic coronary angiographies per year. Private centers are with low volume due to the no reimbursement policy for private interventional cardiology centers from the National Insurance.
Transradial approach was introduced in Macedonia in 2003 mainly for diagnostic catheterization and simple elective PCI procedures. However, 65% of elective PCI and 25% of primary PCI procedures were performed by transradial access in 2007. Furthermore, almost 99% of all PCI procedures were performed by the wrist approach (radial and ulnar) in 2011 at the University Clinic of Cardiology in Skopje. Although low volume centers, almost 90 % of all coronary procedures at the private centers are performed by TRA.
Presently, there are 13 certified interventional cardiologists and 12 in training fellows in Macedonia. Current curriculum encompasses four years of residency in internal medicine after medical school, two years of general cardiology fellowship and two years of subspecialty in interventional cardiology.
Same day discharge strategy could be applied in only 5% of TRA procedures due to the policy of no-reimbursement for outpatient DRG procedures from the National Insurance. Despite the low volume of peripheral angioplasties, most of the SFA and iliac artery stenting procedures are performed by transfemoral access.
However, approximately 150 carotid artery stenting and subclavian artery angioplasties annually are performed by TRA only by experienced operators.
One of the most important challenges we are facing nowadays is the insufficient exposure to the femoral access of young interventional cardiology fellows. The lack of appropriate size and length of devices precludes TRA in most of peripheral angioplasties.
CONCLUSION: Almost all of coronary procedures in Macedonia are performed by the wrist access. Transradial become the preferred approach for carotid and subclavian artery stenting as well. Nevertheless, most of peripheral angioplasties are still performed by femoral access.
Nothing to disclose / No conflicts of interest
WW004 – Radial Approach in the World
COMPARISON OF TRANSRADIAL AND FEMORAL APPROACHES FOR PERCUTANEOUS CORONARY INTERVENTIONS: A HIERARCHICAL BAYESIAN META-ANALYSIS
Olivier F. Bertrand, Patrick Belisle, Dominique Joyal, Olivier Costerousse, Sunil V. Rao, Sanjit Jolly, David Meerkin, Lawrence Joseph
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND: Transradial approach (TRA) for percutaneous coronary interventions (PCI) has been performed since 1994. Despite lower risks of access-site related complications compared to the femoral approach (FA), the clinical benefit of TRA is uncertain. We undertook a systematic review and meta-analysis comparing TRA and FA for PCI.
METHODS: A literature search aimed at identifying all clinical trials and observational studies comparing TRA with FA for PCI with reports of clinical outcomes was performed. Odds ratios (OR) were estimated by a hierarchical Bayesian random-effects model with prespecified stratification for observational and randomized designs. The primary outcomes examined were rates of death, combined incidence of death or myocardial infarction (MI), bleeding and transfusions, early (≤ 30 days) and late after PCI.
RESULTS: We collected data from 73 studies (14 randomized, 59 observational) involving a total of 1,022,123 patients. There was a strong association between TRA and mortality early after intervention (OR 0.52, 95% credible interval (CrI) 0.43-0.62), although the effect was mainly due to observational studies (OR 0.49, 95% CrI 0.39-0.59), with an OR 0.74 (95% CrI 0.38-1.40) in randomized trials. An association between TRA and death or MI was observed over short-term follow-up (OR 0.66, 95% CrI 0.51-0.82), with an OR of 0.72 (95% CrI 0.41-1.14) for long-term follow-up. Compared with FA, TRA was associated with a major reduction in bleeding (OR 0.22, 95% CrI 0.16-0.29) and in transfusions (OR 0.20, 95% CrI 0.10-0.31). These findings were consistent in both randomized and observational studies.
CONCLUSIONS: Our results suggest that PCI performed by TRA is associated with lower risks of death, death or MI, bleeding and transfusions when compared to FA. While an adequately powered randomized trial for ischemic and bleeding outcomes is required to definitively establish the superiority of TRA over FA for PCI, our results suggest that greater adoption of TRA has the potential to substantially improve outcomes among patients undergoing PCI.
Nothing to disclose / No conflicts of interest
WW005 – Radial Approach in the World
TRANSRADIAL APPROACH FOR CORONARY ANGIOGRAPHY AND INTERVENTIONS: RESULTS OF THE FIRST INTERNATIONAL TRANSRADIAL PRACTICE SURVEY
OF Bertrand, S Rao, S Pancholy, S Jolly, J Rodés-Cabau, É Larose, M Hamon, O Costerousse, T Mann
Corresponding author : Olivier F Bertrand, MD PhD, IUCPQ, 2725 chemin Sainte-Foy, Quebec (QC) Canada G1V 4G5; olivier.bertrand@criucpq.ulaval.ca
BACKGROUND:Transradial approach has been adopted as an alternative access site for coronary diagnostic angiography and interventions. However, there is considerable variability in practice pattern and technique around the world.
METHODS and RESULTS : Using a web-based software, a questionnaire was distributed worldwide. The survey was conducted from August 2009 to January 2010 among 1,107 interventional cardiologists in 75 countries (107 in Canada). Although pre-transradial approach (TRA) dual hand circulation testing is not uniform in the world, 94.7% in Canada perform Allen or oxymetry testing. Right radial artery is used in almost 90% (99% in Canada). Judkins catheters are the most popular for left coronary artery (LCA) angiographies (66.5%), and right coronary artery (RCA) angiographies (58.8%). For diagnostic angiography, 5Fr and 6Fr catheters are the most popular catheter sizes whereas for percutaneous coronary intervention (PCI), 6Fr is now standard. For PCI of LCA, operators use standard extra back-up guiding catheters in > 65% and, for RCA 70.4% use right Judkins catheter. Although heparin remains the routine antithrombotic agent in the world, bivalirudin is used in >15% in Canada for PCI. The incidence of radial artery occlusion prior to hospital discharge is not assessed in >50% (72.3% in Canada). Overall, ∼50% responded that their TRA practice will increase in the future (35.1% in Canada).
CONCLUSION: Although its penetration varies, TRA is already widely used for coronary diagnostic angiography and intervention. Diagnostic and guiding-catheters used for TRA remain similar to those used for traditional femoral approach suggesting that specialized radial catheters are not frequently used. However, there is substantial variation in practice as it relates to specific aspects of TRA suggesting that more data are needed to determine the optimal strategy to facilitate TRA and optimize radial artery patency post-catheterization.
Nothing to disclose / No conflicts of interest
CT001 – Ongoing Clinical Trials
NEW COCKTAIL TO PREVENT CLINICAL SPASM IN TRANSRADIAL INTERVENTION
Goldsmit A., Sztejfman C., Chiminela F., Sztejfman M., Bettinotti M.
Corresponding author : Alejandro Goldsmit, MD, Sanatrorio Guemes, Fco Acuña de Figueroa 1240, Servicio de Hemodinamia, C.A.B.A., Buenos Aires, 1180, Argentina. ale.goldsmit@gmail.com
OBJECTIVES: We sought to evaluate Nalbuphine Chloridrate (NC) safety and efficacy in preventing vasospasm during coronary angiography (CA), elective carotid angiography (ECA) and percutaneous coronary intervention (PCI) via the radial artery.
METHODS: 500 consecutive patients scheduled to have CA, ECA and PCI via radial artery were enrolled in a prospective fashion. The same experienced (more than 1000 cases) operator performed all procedures, to eliminate technical failure. Prior to initiation of each procedure, 3 mg of iv NC were given. 1 ml of Lidocaine 2% was utilized for local anesthesia sub cutaneous. A 6 Fr Terumo radial introducer was used followed by 5000 U of un-fractionated heparin (UFH) in all diagnosis cases. Clinical vasospasm was defined as trapping/difficulty to mobilize the catheter and or local access site pain. Exclusion criteria were defined as patients with positive Allen test, arterio-venous (AV) fistula, cardiogenic shock, patients anticipating hemo-dyalisis, need for a 5, 7 o 8Fr system or not palpable radial pulse.
RESULTS: Patients were enrolled in a single center between January 2007 and October 2008. 78% were male, the mean age was 60 ± 23, 82% of patients underwent elective CA or ECA and 18% of patients had PCI. Severe local pain was present only in 1.2% of patients, which resolved after 2mg IV of NC. 14% of patients referred only mild pain at the access site. None of the case experienced catheter trapping or manipulation difficulties. There was no evidence of acute local complications, defined as local hematomas > 5 cms, bleeding, pseudoaneurysms, AV fistulas, neuralgias, local ischemia or distal embolic events.
CONCLUSIONS: The utilization IV NALBUPHINE is safe and efficacious to prevent vasospasm in trans radial intervention to perform CA, ECA and PCI. Only 1.2% of patients in our cohort had severe local pain or vasospasm, but resolve with extra doses of NC.
Nothing to disclose / No conflicts of interest










