

The Accuracy of Three-Dimensional Echocardiography With Multiplanar Reformatting in the Assessment of the Aortic Valve Annulus Prior to Percutaneous Balloon Aortic Valvuloplasty in Congenital Heart Disease
Abstract: Objective. To review the use of three-dimensional echocardiography (3DE) with multiplanar reformatting (MPR) in children with congenital aortic stensosis undergoing percutaneous balloon aortic valvuloplasty to assess its accuracy in measuring the aortic valve annulus and any influence it may have on balloon sizing. Methods. All percutaneous aortic balloon valvuloplasties performed from 01/01/2009 to 01/09/2011 were included in the study. All imaging performed for the procedure to determine the size of the aortic valve annulus and aid in balloon sizing was reviewed. The maximum diameter of the aortic valve annulus using two-dimensional echocardiography (2DE), 3DE with MPR, and angiography was recorded. The balloon size used in the procedure was recorded and the balloon to annulus ratio was calculated. Results. A total of 27 procedures were included in the study. Age varied from 1 day to 156 months (mean age, 53 months) and weight from 2.8-58 kg (mean weight, 18.6 kg). Fourteen patients had 3DE with MPR available for analysis. The 3DE with MPR measurement (13.36 ± 5.4 mm) was not different from angiography (13.54 ± 6.4 mm; P=.803).The 2DE measurement was significantly different from angiography (11.72 ± 5 mm; P<.005). The balloon to annulus ratio based on angiographic measurements did not differ significantly between the patients with 3DE MPR and those without (0.94 ± 0.095 vs 0.91 ± 0.1; P=.468). Conclusion. 3DE with MPR allows a more accurate assessment of the aortic valve annulus compared to 2DE, which may reduce the tendency to undersize balloon choice. 3DE with MPR did not significantly affect our balloon choice, which was largely based on angiographic measurements.
J INVASIVE CARDIOL 2012;24(11):594-598
Key words: aortic regurgitation, balloon sizing
________________________________________________
Percutaneous balloon valvuloplasty is a well-recognized technique for the management of aortic stenosis in children with congenital heart disease.1 Accurate measurement of the aortic valve annulus is important in determining balloon sizing for the procedure.2-4 Oversizing has been correlated with more significant aortic regurgitation, which has caused operators to err on the side of caution during balloon selection.5
The traditional measurements are made using two-dimensional echocardiography (2DE) and angiography; some authors suggest using the smaller of these measurements when a discrepancy arises, hence tending toward smaller balloon size selection.6,7
Three-dimensional echocardiography (3DE) with multi-planar reformatting (MPR) has been shown to be feasible in the assessment of children with congenital heart disease.8-11 MPR allows the measurement of the aortic annulus in different orthogonal planes, which may give a more accurate recording of the true annular size.
In this study, we sought to review the use of 3DE with MPR in children with congenital aortic stenosis undergoing balloon aortic valvuloplasty to determine the accuracy of the measurement when compared to 2DE and angiography and to assess any impact it may have on balloon choice.
Methods
 All pediatric balloon aortic valvuloplasties performed from 01/01/2009 to 30/09/2011 were included in the study. Our indications to treat were based on previously defined criteria for the procedure, ie, symptoms, left ventricular hypertrophy on electrocardiography or echocardiogram, Doppler gradient of >80 mm Hg or peak to peak gradient of greater than 50 mm Hg.2 All 2DEs and 3DE MPRs performed immediately prior to the procedure were reviewed and the maximum dimension of the aortic annulus recorded at the time was used for analysis. Initial 3DE images had been analyzed at the time of the procedure using Phillips QLAB
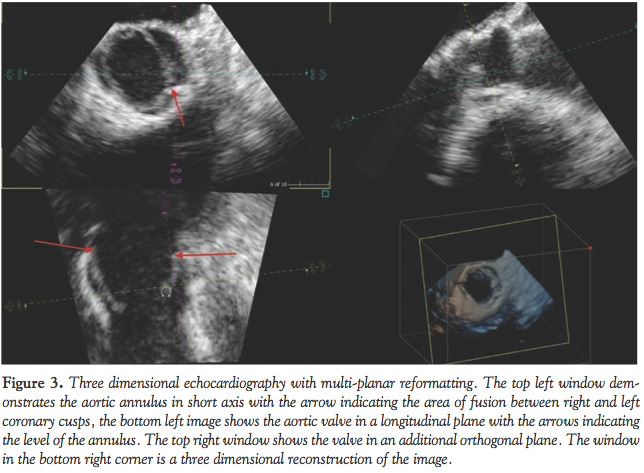
All pediatric balloon aortic valvuloplasties performed from 01/01/2009 to 30/09/2011 were included in the study. Our indications to treat were based on previously defined criteria for the procedure, ie, symptoms, left ventricular hypertrophy on electrocardiography or echocardiogram, Doppler gradient of >80 mm Hg or peak to peak gradient of greater than 50 mm Hg.2 All 2DEs and 3DE MPRs performed immediately prior to the procedure were reviewed and the maximum dimension of the aortic annulus recorded at the time was used for analysis. Initial 3DE images had been analyzed at the time of the procedure using Phillips QLAB  version 8.1 advanced three-dimensional quantification. The intraprocedural angiograms were reviewed in the anteroposterior and lateral projections and the maximum dimension of the aortic annulus recorded at the time of the procedure was used in analysis. The maximum balloon size as documented in the catheter report was recorded. Patients in whom 3DE images had been performed but no evidence was found of analysis using MPR were excluded from statistical analysis. We did not perform MPR on a retrospective basis. The degree of aortic regurgitation was assessed during angiography, on echocardiogram immediately post balloon, and at more than 3 months follow-up. The degree of aortic regurgitation was defined as mild, moderate, or severe using previously defined criteria (Figures 1-3).5
version 8.1 advanced three-dimensional quantification. The intraprocedural angiograms were reviewed in the anteroposterior and lateral projections and the maximum dimension of the aortic annulus recorded at the time of the procedure was used in analysis. The maximum balloon size as documented in the catheter report was recorded. Patients in whom 3DE images had been performed but no evidence was found of analysis using MPR were excluded from statistical analysis. We did not perform MPR on a retrospective basis. The degree of aortic regurgitation was assessed during angiography, on echocardiogram immediately post balloon, and at more than 3 months follow-up. The degree of aortic regurgitation was defined as mild, moderate, or severe using previously defined criteria (Figures 1-3).5
 Statistics. All data were analyzed using SPSS version 18. Data were compared using an independent samples student’s t-test (two-tailed) and Spearman’s rank correlation coefficient. A Bland Altman plot was constructed for different annular measurements. P-values <.05 were considered statistically significant. All values are quoted as means ± standard deviations.
Statistics. All data were analyzed using SPSS version 18. Data were compared using an independent samples student’s t-test (two-tailed) and Spearman’s rank correlation coefficient. A Bland Altman plot was constructed for different annular measurements. P-values <.05 were considered statistically significant. All values are quoted as means ± standard deviations.
Results
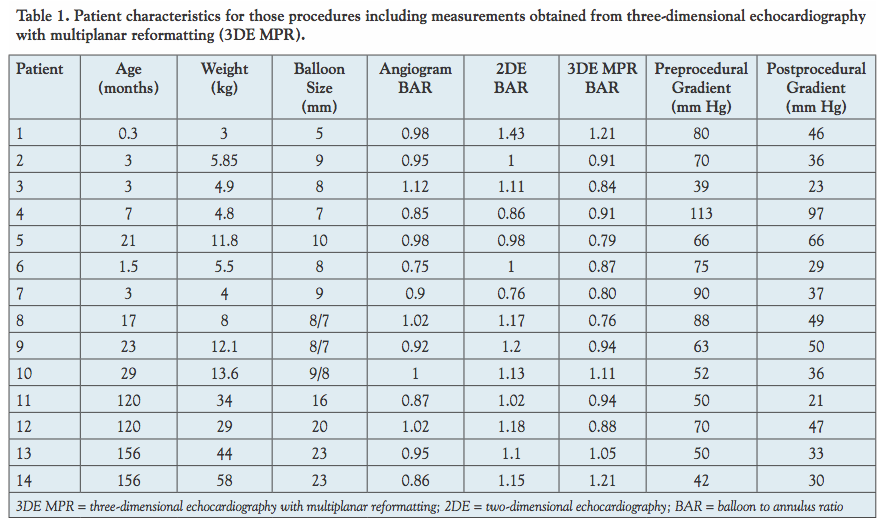 Patient characteristics. A total of 27 procedures were performed on 25 patients during the study period from January 2009 to September 2011.The patients varied in age from 1 day to 156 months (mean age, 53 months) and weight from 2.8 kg to 58 kg (mean weight, 18.6 kg). Of the 27 procedures, 14 had 3DE with MPR available for analysis, 6 had 3DE without evidence of MPR, and 7 had only 2DE (Table 1).
Patient characteristics. A total of 27 procedures were performed on 25 patients during the study period from January 2009 to September 2011.The patients varied in age from 1 day to 156 months (mean age, 53 months) and weight from 2.8 kg to 58 kg (mean weight, 18.6 kg). Of the 27 procedures, 14 had 3DE with MPR available for analysis, 6 had 3DE without evidence of MPR, and 7 had only 2DE (Table 1).
Previous procedures. Fifteen patients had not undergone any prior interventions at time of percutaneous balloon valvuloplasty. Surgical valvotomy had been performed in 6 patients. Previous percutaneous balloon valvuloplasty had been performed on 8 patients, one of whom was as a fetus at 22 weeks gestation.
Valve morphology. Within the cohort, there were 20 bicuspid (12 true and 8 functionally bicuspid) aortic valves. Three procedures were carried out on a bicuspid neo-aortic valve in a patient with TGA post arterial switch. One valve was tricuspid and 3 were unicuspid.
Details of procedures performed
Gradient reduction. The preprocedural peak to peak gradient was greater than 50 mm Hg in 20 patients, with a range of 39-113 mm Hg (mean, 60 mm Hg). Postprocedural gradients fell significantly to 18-97 mm Hg (mean, 39 mm Hg). Six patients remained at 50 mm Hg or greater following procedure.
The average gradient reduction when using a double balloon technique was from 58 mm Hg to 40.5 mm Hg versus using a single balloon technique of 60.7 to 38 mm Hg. This was not statistically significant.
Aortic regurgitation. Only 1 patient in the study had moderate aortic regurgitation (AR) on follow-up echocardiogram. In this patient, the AR had progressed from trivial during angiography to mild on initial echocardiogram. In this patient, the measurements of the valve annulus were 15.7 mm, 17.1 mm, and 18.43 mm on 2DE, 3DE with MPR, and angiogram, respectively, with a balloon size of 16 mm chosen for the procedure and a balloon to annulus ratio (BAR) of 0.87 based on the angiographic measurement.
Twenty-one patients had nil to trivial AR on initial angiography. Seven patients who showed no initial AR on angiography were noted to have mild AR on initial echocardiogram and follow-up echocardiograms with no significant progression in the degree of AR. One patient demonstrated progression in the degree of AR from initial echocardiogram to follow-up echocardiogram, although this was from trivial to mild. In 6 patients, no follow-up echocardiogram was available on our system beyond 3 months, one of the patients died at 2 months of age, 2 patients are receiving follow-up elsewhere, and 3 patients had not had follow-up at the time of data collection.
Complications. Complications were documented in 6 patients. Two patients had minor complications related to vascular access, with 1 requiring multiple punctures (after failure to access the right femoral artery, the left femoral artery was successfully punctured). This patient did not have a history of previous interventions and had no postprocedural complications. One patient developed reduced limb perfusion with loss of pulses and required a heparin infusion overnight with a good response and normalization of perfusion. One patient encountered a problem when an Angio-Seal device malfunctioned while we tried to seal a puncture with an 8 Fr sheath; this resulted in a persistent arterial bleed that responded to pressure. The patient was reviewed by the vascular surgical team and has had no ongoing vascular issues. At induction in the anesthetic room, 1 patient developed complete heart block requiring cardiac massage, atropine, and adrenaline. This patient was noted to have moderate to severely depressed left ventricular function prior to the procedure. After 1 minute of resuscitation, the rhythm reverted to a sinus rhythm and the procedure was successfully completed with good postprocedure recovery in left ventricular function. Intraprocedural complications were experienced in 1 patient who developed a ventricular tachycardia on balloon inflation, which required electrical cardioversion. It was felt that this was due to the balloon milking into the left ventricle during inflation; on subsequent inflations, sinus rhythm was maintained and the procedure was successfully completed. Postprocedural complications were experienced by 1 patient who developed mild pulmonary edema, which responded to diuresis and resolved by the following day.
The screening time for the procedures ranged from 6 minutes to 59 minutes (mean, 19 ± 30 minutes).
Freedom from intervention. The freedom from intervention for the cohort was 86% at the time of the study.
3DE MPR
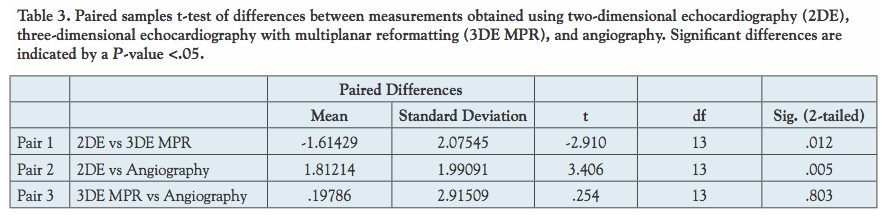
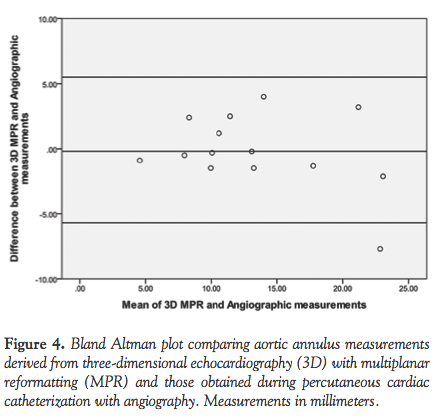
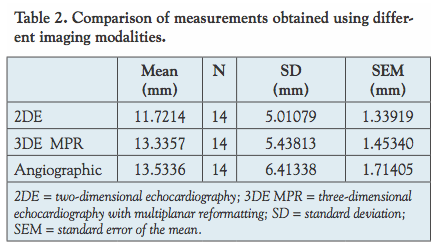 Accuracy in determining annulus size. The 3D measurement (13.36 ± 5.4 mm) was not statistically different from the angiographic measurement (13.54 ± 6.4 mm; P=.803), whereas the 2DE measurement was statistically different (11.72 ± 5 mm; P<.005) (Tables 2 and 3). Bland Altman plots confirmed these differences (Figures 4 and 5). Both the 2D (r = 0.96; P<.001) and 3D (r = 0.8; P<.001) measurements showed a strong linear correlation with angiographic measurements.
Accuracy in determining annulus size. The 3D measurement (13.36 ± 5.4 mm) was not statistically different from the angiographic measurement (13.54 ± 6.4 mm; P=.803), whereas the 2DE measurement was statistically different (11.72 ± 5 mm; P<.005) (Tables 2 and 3). Bland Altman plots confirmed these differences (Figures 4 and 5). Both the 2D (r = 0.96; P<.001) and 3D (r = 0.8; P<.001) measurements showed a strong linear correlation with angiographic measurements.
 Effect on balloon sizing. A single-balloon technique was used in 21 procedures and a double-balloon technique was used in 6 procedures. Combined diameter of double balloons was calculated using Yeager’s formula.12
Effect on balloon sizing. A single-balloon technique was used in 21 procedures and a double-balloon technique was used in 6 procedures. Combined diameter of double balloons was calculated using Yeager’s formula.12
Balloon sizes for the entire cohort varied from 4.5 mm to 23 mm (12.9 ± 7.5 mm). The balloon sizes in those patients with 3DE and MPR were not significantly different versus those without 3DE and MPR (12.6 ± 5.9 vs. 13.3 ± 5.1; P=.785).
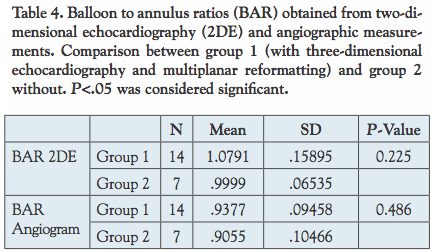 The BAR based on angiographic measurements did not differ significantly between the patients with 3DE and MPR versus those without (0.94 ± 0.095 vs 0.91± 0.1; P=.468). The BAR obtained using 2DE measurements did not show a significant difference between groups (1.08 ± 0.15 vs 1 ± 0.65; P=.225) (Table 4).
The BAR based on angiographic measurements did not differ significantly between the patients with 3DE and MPR versus those without (0.94 ± 0.095 vs 0.91± 0.1; P=.468). The BAR obtained using 2DE measurements did not show a significant difference between groups (1.08 ± 0.15 vs 1 ± 0.65; P=.225) (Table 4).
Discussion
 The aim of percutaneous balloon aortic valvuloplasty is to achieve the best gradient reduction possible with the least amount of postprocedural aortic regurgitation.1 Accurate measurement of the aortic valve annulus and balloon sizing are integral to this outcome.
The aim of percutaneous balloon aortic valvuloplasty is to achieve the best gradient reduction possible with the least amount of postprocedural aortic regurgitation.1 Accurate measurement of the aortic valve annulus and balloon sizing are integral to this outcome.
The relationship between oversized balloons and postprocedural aortic regurgitation is well known.5 A BAR of greater than 1.2 has been associated with damage of aortic and mitral valves, as well as the ventricular septum. The valvuloplasty and 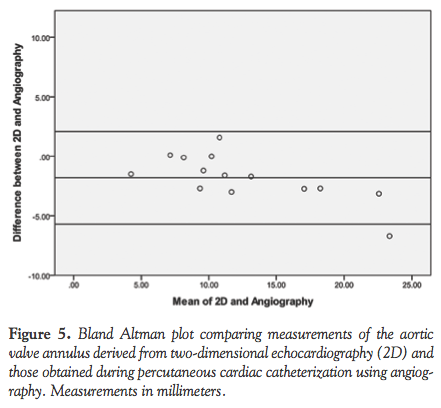 angioplasty of congenital anomalies (VACA) registry has reported an increase in aortic regurgitation with BAR of greater than 1.2 Evidence is unclear regarding the impact of balloon size on percentage gradient reduction following the procedure, and some suggest suboptimal relief of valve obstruction is achieved with BAR of 0.9 or less.2 A number of previous studies have been unable to demonstrate any correlation between percentage gradient reduction and balloon size.5,7 This highlights the importance of accurate valve annulus assessment.
angioplasty of congenital anomalies (VACA) registry has reported an increase in aortic regurgitation with BAR of greater than 1.2 Evidence is unclear regarding the impact of balloon size on percentage gradient reduction following the procedure, and some suggest suboptimal relief of valve obstruction is achieved with BAR of 0.9 or less.2 A number of previous studies have been unable to demonstrate any correlation between percentage gradient reduction and balloon size.5,7 This highlights the importance of accurate valve annulus assessment.
Traditionally, the measurement of the aortic valve annulus has been made using 2DE and angiography.1-3 Reich et al reported their results in 2004 and found almost perfect agreement between echocardiography and angiography in the annulus diameter dimensions (r = 0.978).6
We were able to confirm the strong linear correlation between 2DE and angiography, but found that the measurements differed significantly in terms of exact diameter. The 2DE measurements undersize the aortic valve annulus by assessing the valve in only one plane. 3DE with MPR allows the assessment of the aortic valve annulus in a number of orthogonal planes. Measurements of the aortic valve annulus using 3DE and MPR showed a strong linear correlation with angiographic measurements and did not differ in exact diameter.
The use of 3DE and MPR has not had a significant impact on our practice in terms of balloon sizing, which has largely been based on angiographic measurements. The measurements derived using 2DE were significantly smaller than both angiography and 3DE with MPR. Some authors suggest using the smaller of the measurements should a discrepancy arise;6,7 had this been our practice, we would have under-sized the balloon for the procedure. 3DE with MPR may allow more confidence in balloon choice.
MPR has been used in patients with congenital heart disease with a significant impact on patient management.8-11 In a study by Bharucha et al, MPR was used to assess patients for suitability of biventricular repair, to clarify the morphology of the atrioventricular valves, and to accurately demonstrate the anatomy of the aortic valve. They were able to demonstrate clinically important information that altered management or changed the principal diagnosis in 32 of 300 patients. The ability to assess the anatomy of the aortic valve in a number of orthogonal planes and determine the true diameter of the aortic valve annulus makes MPR important in the assessment of any patient undergoing percutaneous balloon aortic valvuloplasty.
Study limitations. This study discusses our initial experience in the use of 3DE and MPR. Although our total numbers are small, they are comparable to previous studies discussing balloon aortic valvuloplasty. To add strength to the findings, we would need to continue with the acquisition of 3DE and MPR in all patients undergoing the procedure. In some patients, there was evidence of 3D acquisition but not of MPR, this made it impossible to tell if this affected clinical decision making at the time of the procedure. These patients were, however, excluded from statistical analysis.
Conclusion
3DE with MPR is an important addition to the assessment of the aortic annulus prior to balloon aortic valvuloplasty in children with congenital heart disease. We feel that this allows a more accurate assessment of the aortic valve annulus, which may reduce the tendency to undersize balloon choice, and thus allow more appropriate balloon sizing for the procedure. Although the use of 3DE MPR has not significantly affected our balloon choice, which is largely based on angiographic measurements, we feel that with ongoing experience 3DE MPR will play a vital role. Further data acquisition is required to assess this role and its possible impact on outcomes.
References
- Lababidi Z. Aortic balloon valvuloplasty. Am Heart J. 1983 Oct;106(4 Pt 1):751-752.
- Feltes TF, Bacha E, Beekman RH 3rd, et al. Indications for cardiac catheterization and intervention in pediatric cardiac disease: a scientific statement from the American Heart Association. Circulation. 2011;123(22):2607-2652.
- Hijazi ZM, Awad SM. Pediatric cardiac interventions. JACC Cardiovasc Interv. 2008;1(6):603-611.
- Borghi A, Agnoletti G, Valsecchi O, Carminati M. Aortic balloon dilatation for congenital aortic stenosis: report of 90 cases (1986-98). Heart. 1999;82(6):e10.
- Balmer C, Beghetti M, Fasnacht M, Friedli B, Arbenz U. Balloon aortic valvoplasty in pediatric patients: progressive aortic regurgitation is common. Heart. 2004;90(1):77-81.
- Reich O, Tax P, Marek J, et al. Long-term results of percutaneous balloon valvoplasty of congenital aortic stenosis: independent predictors of outcome. Heart. 2004;90(1):70-76.
- Beekman RH, Rocchini AP, Crowley DC, et al. Comparison of single and double balloon valvuloplasty in children with aortic stenosis. J Am Coll Cardiol. 1988;12(2):480-485.
- Bharucha T, Anderson RH, Lim ZS, Vettukattil JJ. Multiplanar review of three-dimensional echocardiography gives new insights into the morphology of Ebstein’s malformation. Cardiol Young. 2010;20(1):49-53.
- Bharucha T, Ho SY, Vettukattil JJ. Multiplanar review analysis of three-dimensional echocardiographic datasets gives new insights into the morphology of subaortic stenosis. Eur J Echocardiogr. 2008;9(5):614-620.
- Bharucha T, Roman KS, Anderson RH, Vettukattil JJ. Impact of multiplanar review of three-dimensional echocardiographic data on management of congenital heart disease. Ann Thorac Surg. 2008;86(3):875-881.
- Bharucha T, Sivaprakasam MC, Roman KS, Vettukattil JJ. A multiplanar three dimensional echocardiographic study of mitral valvar annular function in children with normal and regurgitant valves. Cardiol Young. 2008;18(4):379-385.
- Yeager SB, Neal WA, Balian AA, Gustafson RA. Percutaneous balloon pulmonary valvuloplasty. W V Med J. 1986;82(6):169-171.
_________________________________________________________
From the Southampton University Hospital NHS trust, Congenital Cardiac Centre, Southampton, United Kingdom.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 5, 2012, provisional acceptance given May 11, 2012, final version accepted June 22, 2012.
Address for correspondence: David E. Black, MBBCH/MRCPCH/FCPaeds(SA), RCPCH/JRCPTB, Cardiothoracics, Southampton General Hospital, Tremona Road, Southampton, United Kingdom. Email: david.black@suht.swest.nhs.uk










