

Acute Intraventricular Thrombosis of an Impella LP 5.0 Device in an ST-Elevated Myocardial Infarction Complicated by Cardiogenic Shock
Download a PDF of this article.
ABSTRACT: A 58-year-old male patient, suffering from an acute anterior ST-elevated myocardial infarction, developed cardiogenic shock, despite an optimal revascularization and hemodynamic support through the use of an intra-aortic balloon pump and inotropic pharmacological agents. Additional support was provided by a left ventricular assistance device Impella LP 5.0 (Abiomed, Europe GmbH). Device failure occurred 27 hours after implantation due to an acute thrombosis of the Impella inflow portion. This major adverse event might have occurred due to an inflammatory status in the cardiogenic shock context, a pre-existing intraventricular thrombus that could have been sucked up inside the Impella, and/or a subtherapeutic anticoagulation. There are very few data regarding this type of complication. Further studies are therefore needed to assess the frequency of such a complication and the means to avoid it.
J INVASIVE CARDIOL 2013;25(1):E1-E3
Key words: left ventricular assist, LVAD
_______________________________________________
The Impella LP, a percutaneous left ventricular assistance device (LVAD), is a recent development in cardiogenic shock management, which can facilitate patients’ recovery in addition to standard care. Very few adverse events related to the implantation and use of this device have been reported. This is partly due to its recent availability. Our report focuses on a case of an acute intraventricular thrombosis of an IMPELLA LP 5.0 device in a patient implanted for a severe cardiogenic shock complicating an acute myocardial infarction.
Case Report. A 58-year-old male patient with no prior medical history was admitted for primary percutaneous coronary intervention for an acute ST-elevated myocardial anterior infarction within 12 hours of symptoms. The coronary angiogram revealed an ostial left anterior descending (LAD) occlusion. A coronary thrombectomy followed by direct stenting using a 3.0 x 16 mm bare-metal stent (Titan; Hexacath) was performed. Optimal reperfusion in the LAD was obtained with a final TIMI 3 coronary flow at the end of the procedure. Despite optimal reperfusion, systolic blood pressure persisted below 90 mm Hg and an intra-aortic balloon pump (IABP) was inserted. The cardiogenic shock remained severe with clinical signs of multi-organ failure (mean blood pressure below 70 mm Hg, impaired diuresis <1 mL/kg/hr, confusion, metabolic acidosis). Inotropic support with continuous infusion of milrinone was started and the patient was transferred to our intensive care unit.
Transthoracic echocardiogram (TTE) on admission showed a left ventricular ejection fraction of 20% with diffuse akinesia of the antero-septo-apical walls. No intraventricular thrombus was noted. A Swan-Ganz catheter was inserted within 6 hours after admission and showed a cardiac output of 1.5 L/min/m², high left ventricular filling pressures with capillary wedge pressure of 30 mm Hg, and central venous and systolic pulmonary arterial pressures of 15 mm Hg and 52/33 mm Hg, respectively. The right ventricular systolic function assessed by echocardiography was preserved.
During the first 24 hours after admission, there was no improvement of the hemodynamic status. Despite adjustment and constant increase of the inotropic drugs and diuretic doses, Swan-Ganz measures remained unchanged.
Therefore, 24 hours after admission, an Impella LP 5.0 LVAD was surgically implanted via the right axillary artery. Preoperative transesophageal echocardiogram (TEE) showed no intracardiac thrombus. Postimplantation radiological controls showed optimal position of the device. Impella power was set at level 7 to obtain a device output of 3.5 L/min and further settings remained unchanged.
Hemodynamic and clinical status immediately improved. Cardiac output increased from 1.6 L/min/m² to 2.3 L/min/m², and pulmonary capillary wedge pressure decreased from 30 to 15 mm Hg. A significant increase of diuresis was observed, as well as an improvement of renal and hepatic functions. Within the next 24 hours, inotropic support was successfully weaned.
At the onset of acute MI, anticoagulation was provided by enoxaparin 1 mg/kg/12 hrs. During the surgical procedure, unfractionated heparin (UFH) was administered, and activated clotting times were measured at 302 s and 315 s, after a 50 UI/kg UFH bolus. After the insertion of the device, irrigation was performed using a continuous infusion of UFH (50 UI/mL) and 20% dextrose solution at 3.8 mL/hr, ie, 190 UI of UFH/hr according to the manufacturer’s recommendations. Enoxaparin was stopped, with the last injection performed 8 hours before surgery. Aspirin (75 mg/day) and prasugrel (10 mg/day) were also administered.
Despite heparin infusion, postoperative blood levels of activated cephalin times remained low (29 s at 12 hours post implantation and and 35 s at 20 hours post implantation). Consequently, UFH infusion speed was increased. Remarkably, device pressures were monitored as normal by the Impella system.
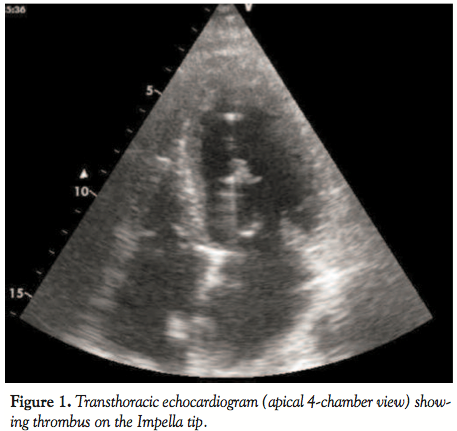 A sudden Impella dysfunction occurred 27 hours after implantation, consisting of a brutal stop with impossibility to restart the pump. Immediate TTE revealed a 12-mm long thrombus caught inside the pigtail tip of the device (Figure 1). TEE showed that the thrombus was trapped inside the pump (Figure 2). There was no evidence of additional intraventricular thrombus in the left ventricle.
A sudden Impella dysfunction occurred 27 hours after implantation, consisting of a brutal stop with impossibility to restart the pump. Immediate TTE revealed a 12-mm long thrombus caught inside the pigtail tip of the device (Figure 1). TEE showed that the thrombus was trapped inside the pump (Figure 2). There was no evidence of additional intraventricular thrombus in the left ventricle.
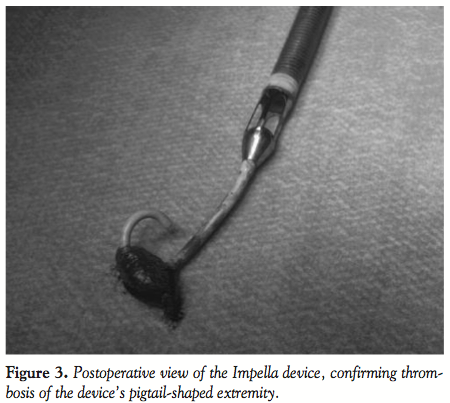
The patient underwent an emergent surgical device explantation with sternotomy and aortotomy (12 minutes of cardiac arrest protected by a crystalloid cardioplegia) under extracorporeal circulation assistance. As shown in Figure 3, an important thrombus was found rolled up inside the pigtail tip. A central extracorporeal membrane oxygenator was inserted for temporary circulatory support.
 After stabilization, a whole-body computed tomography scan showed no sign of peripheral embolism. ECLS was weaned after 5 days, without any further adverse events. The outcome was favorable and the patient was discharged from hospital.
After stabilization, a whole-body computed tomography scan showed no sign of peripheral embolism. ECLS was weaned after 5 days, without any further adverse events. The outcome was favorable and the patient was discharged from hospital.
Discussion. The Impella device is an intravascular rotational axial-flow pump designed to provide cardiac support during left ventricular failure. The device continuously aspirates blood from the LV cavity and pumps it into the ascending aorta, via an axial turbin. Thus, it provides a continuous cardiac output and reduces LV afterload. It also significantly improves coronary hemodynamics.1,2
 The Impella LP device’s safety and efficiency have been evaluated in the past few years mainly in high-risk percutaneous intervention3-6 and cardiogenic shock.7-13 Device-related adverse events were mostly related to vascular access, ie, dissections or acute thrombosis.1-13 In our center, these access-site complications have largely been reduced by a systematic device insertion through the axillary artery rather than femoral.14 Rare cases of functional mitral stenosis, due to the vacuum effect of the pump in the LV, have also been described by Toggweiler and colleagues.15
The Impella LP device’s safety and efficiency have been evaluated in the past few years mainly in high-risk percutaneous intervention3-6 and cardiogenic shock.7-13 Device-related adverse events were mostly related to vascular access, ie, dissections or acute thrombosis.1-13 In our center, these access-site complications have largely been reduced by a systematic device insertion through the axillary artery rather than femoral.14 Rare cases of functional mitral stenosis, due to the vacuum effect of the pump in the LV, have also been described by Toggweiler and colleagues.15
One specific issue is the irrigation of the device by continuous heparin and dextrose infusion to prevent blood from reaching the engine. Anticoagulation is needed to prevent clotting. To our knowledge, we are presenting the first documented case of massive thrombosis of an Impella device. The macroscopic aspect of the thrombus after device explantation (Figure 3) suggests that a pre-existing and unspotted intraventricular thrombus must have been sucked up inside the device, ie, a long clot trapped inside the pigtail tip of the inflow segment. The subtherapeutic anticoagulation levels obtained prior to this event and the large anterior and apical akinesia predisposing to thrombus formation further support this hypothesis.
In our case report, we suspect insufficient anticoagulation to have contributed to the pump failure. Indeed, the anticoagulation levels didn’t reach the therapeutic range, as activated clotting times were approximately 30 seconds. Moreover, anti-thrombin III levels were normal. No biological sign for haemolysis was found.
In our experience, we have observed that for most patients implanted with an Impella device, the heparin solution used for irrigation can achieve appropriate anticoagulation levels without additional heparin infusion. Since anticoagulation at the onset of the acute MI and during primary PCI was ensured by enoxaparin, UFH administration began only at the time of the Impella insertion. Low activated clotting times after surgery didn’t immediately raise concerns. Therefore, UFH infusion speed was increased, as generally performed in such circumstances, and switching to a different anticoagulation drug, such as bivalirudin or argatroban, wasn’t considered. During surgery, activated clotting time levels were optimal and their later decrease could not have been anticipated. Besides, thrombosis happened shortly after device implantation, leaving little time for physicians to consider an anticoagulation switch.
The important inflammatory syndrome (fibrinogen 8.4 g/L) present at the time of implantation and during the following hours could have been responsible for a high thrombotic status. This inflammatory response can be explained by the severity of the cardiogenic shock, as no evidence for systemic infection was found.
The most probable hypothesis is that the thrombus either developed or was already present in the LV at the time of the Impella insertion and then got trapped inside the device. Pre-operative TTE showed no intraventricular thrombus, which would have been a clear contraindication to such a procedure. The limits of TTE’s sensitivity for detecting intraventricular thrombi may be responsible for misdiagnosis. Moreover, intraventricular thrombus can be transient and be undiagnosable at the time of TTE performance. In our case, repeated TTE had been performed every 6 hours before the failure of the Impella, and no anomaly of the device or in the LV was reported. However, Impella devices induce important TTE imaging artefacts that can mask intraventricular thrombi.
The Impella is a circulatory support system that has interesting potential applications for the management of myocardial infarction related to cardiogenic shock and acute congestive heart failure. It is mostly used as a bridge to recovery for patients who remain in a critical hemodynamic state despite revascularization and IABP.16,17 Our case report suggests that a strong inflammatory syndrome and severe LV dysfunction with apical akinesia might expose patients to Impella thrombosis. It also suggests that appropriate anticoagulation therapy and monitoring are essential to avoid this type of adverse event.
References
- Remmelink M, Sjauw KD, Henriques JP, et al. Effects of left ventricular unloading by Impella Recover LP 2.5 on coronary hemodynamics. Cathet Cardiovasc Interv. 2007;70(4):532-537.
- Cyrus T, Mathews S, Lasala J. Use of mechanical assist during high-risk PCI and STEMI with cardiogenic shock. Catheter Cardiovasc Interv. 2010;75(Suppl 1):S1-S6.
- Dixon SR, Henriques JP, Mauri L, et al. A prospective feasibility trial investigating the use of the Impella 2.5 system in patients undergoing high-risk percutaneous coronary intervention (the PROTECT I trial): initial U.S. experience. JACC Cardiovasc Interv. 2009;2(2):91-96.
- Henriques JP, Remmelink M, Baan Jr J, et al. Safety and feasibility of elective high-risk percutaneous coronary intervention procedures with left ventricular support of the Impella Recover LP 2.5. Am J Cardiol. 2006;97(7):990-992.
- Sjauw K, Konorza T, Erbel R, et al. Supported high-risk percutaneous coronary intervention with the Impella 2.5 device: the Europella registry. J Am CollCardiol. 2009;54(25):2430-2434.
- Vechio S, Chechi T, Giuliani G, et al. Use of Impella Recover 2.5 left ventricular assist device in patients with cardiogenic shock or undergoing high-risk percutaneous intervention procedures: experience of a high-volume center. Minerva Cardioangiol. 2008;56(4):391-399.
- Engström A, Sjauw K, Baan J, et al. Long-term safety and sustained left ventricular recovery: long-term results of percutaneous left ventricular support with Impella LP2.5 in ST-elevation myocardial infarction. EuroIntervention. 2011;6(7):860-865.
- Seyfarth M, Sibbing D, Bauer I, et al. A randomized clinical trial to evaluate the safety and efficacy of a percutaneous left ventricular assist device versus intra-aortic balloon pumping for treatment of cardiogenic shock caused by myocardial infarction. J Am Coll Cardiol. 2008;52(19):1584-1588.
- Cheng JM, den Uil CA, Hoeks SE, et al. Percutaneous left ventricular assist devices vs. intra-aortic balloon pump counterpulsation for treatment of cardiogenic shock: a meta-analysis of controlled trials. Eur Heart J. 2009;30(17):2102-2108.
- Meyns B, Dens J, Sergeant P, Herijgers P, Daenen W, Flameng W. Initial experiences with the Impella device in patients with cardiogenic shock — Impella support for cardiogenic shock. Thorac Cardiovasc Surg. 2003;51(6):312-317.
- Thiele H, Smalling RW, Schuler GC. Percutaneous left ventricular assist devices in acute myocardial infarction complicated by cardiogenic shock. Eur Heart J. 2007;28(17):2057-2063.
- Lamarche Y, Cheung A, Ignaszewski A, et al. Comparative outcomes in cardiogenic shock patients managed with Impella microaxial pump or extracorporeal life support. J Thorac Cardiovasc Surg. 2010 Sep 27 [Epub ahead of print].
- Granfeldt H, Hellgren L, Dellgren G, et al. Experience with the Impella recovery axial-flow system for acute heart failure at three cardiothoracic centers in Sweden. Scand Cardiovasc J. 2009;43(4):233-239.
- Sassard T, Scalabre A, Bonnefoy E, et al. The right axillary artery approach for the Impella Recover LP 5.0 microaxial pump. Ann Thorac Surg. 2008;85(4):1468-1470.
- Toggweiler S, Jamshidi P, Erne P. Functional mitral stenosis: a rare complication of the Impella assist device. Eur J Echocardiogr. 2008;9(3):412-413.
- Babaev A, Frederick PD, Pasta DJ, Every N, Sichrovsky T, Hockman JS, NRMI Investigators. Trends in management and outcomes of patients with acute myocardial infarction complicated by cardiogenic shock. JAMA. 2005;294(4):448-454.
- Baughman KL, Jarcho JA. Bridge to life cardiac mechanical support. N Engl J Med.2007;357(9):846-849.











