

Adoption of the Hybrid CTO Approach by a Single Non-CTO Operator: Procedural and Clinical Outcomes
Abstract: Background. The feasibility of adopting the “hybrid” approach by a single operator without prior experience in percutaneous coronary intervention (PCI) of chronic total occlusions (CTOs) has not been described. Methods. Consecutive patients who underwent CTO-PCI by a single operator using the “hybrid” approach between 2012 and 2013 formed the analytic cohort. No patient was declined on the basis of angiographic findings. Clinical and angiographic characteristics together with procedural and hospital outcomes are described. Results. During the study period, a total of 48 consecutive patients underwent PCI of 50 CTOs. Mean age was 63.4 ± 9.4 years and most patients (83%) were men. The right coronary artery (RCA) was the most commonly treated CTO vessel (54%) and mean J-CTO score was 2.3 ± 1.1. A primary retrograde approach was chosen for 33% of lesions and 40% required use of an epicardial collateral vessel. The primary strategy was effective in 65% of successful cases, 35% required one change in strategy, and 15% requiring two strategy changes. Procedural success rate was 92%. The median number of stents used was 3 (interquartile range [IQR], 2-4] and the total stent length was 73 mm [IQR, 38-96 mm). Mean contrast volume was 356.4 ± 148.3 mL and the mean air kerma radiation exposure was 3.5 ± 2.0 Gy. No patient experienced a major periprocedural complication. Conclusion. The “hybrid” approach to CTO-PCI can be successfully adopted by a single operator with excellent early procedural success and low complication rates, despite a lack of prior CTO-PCI experience.
J INVASIVE CARDIOL 2015;27(3):139-144
Key words: percutaneous coronary intervention, chronic total occlusion, hybrid approach
_________________________________
Editor's note: View related video at "A Video Demonstration of the Hybrid CTO Approach."
Coronary artery chronic total occlusions (CTOs) are commonly found during catheterization of patients with coronary artery disease, but rates of attempted percutaneous revascularization have historically been low, in part due to high rates of procedural failure using standard percutaneous coronary intervention (PCI) techniques.1,2 Nevertheless, successful percutaneous revascularization of CTOs has been associated with improvements in left ventricular function, quality of life, and mortality.3-5 However, CTO-PCI remains challenging and is often considered the “final frontier” of coronary interventions.6 Recently, there has been growing interest in CTO-PCI as illustrated by the proliferation of procedural and technological advancements in the field.7
Given its constant rapid evolution, it can be quite overwhelming for a non-CTO operator to start and stay abreast of the CTO-PCI field. The absence of a standardized teaching method has also hindered interventional cardiologists’ development as CTO-PCI operators, limiting their ability to rapidly become efficient at CTO-PCI with high success and low complication rates. For most cardiac interventionalists, the learning curve for CTO-PCI is rather daunting, often requiring 200-300 CTO-PCIs before achieving a high success rate.7
The “hybrid” approach is revolutionizing CTO-PCI by providing a systematic, reproducible, and teachable approach to CTO crossing based on coronary anatomy (Figure 1).8 This approach increases efficacy, 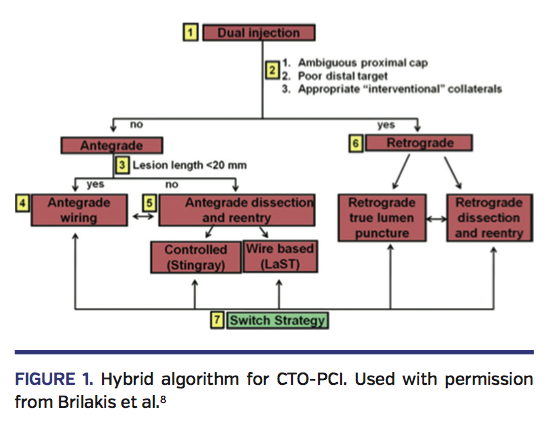 efficiency, and safety of CTO-PCI in centers with experienced CTO operators, as demonstrated in four recent case series.9-12 Adoption of this approach among inexperienced CTO-PCI operators has not previously been described and some interventional cardiologists may still feel that CTO-PCI remains beyond their capacity. To this end, this report describes the first 50 CTO-PCI attempts by a single operator without prior CTO-PCI experience following adoption of the “hybrid” approach.
efficiency, and safety of CTO-PCI in centers with experienced CTO operators, as demonstrated in four recent case series.9-12 Adoption of this approach among inexperienced CTO-PCI operators has not previously been described and some interventional cardiologists may still feel that CTO-PCI remains beyond their capacity. To this end, this report describes the first 50 CTO-PCI attempts by a single operator without prior CTO-PCI experience following adoption of the “hybrid” approach.
Methods
Study design. We retrospectively examined the procedural characteristics and outcomes of the first 50 consecutive CTO-PCI cases performed by a single operator (MV) who did not have prior CTO-PCI experience, but had performed over 800 PCIs. These procedures were performed over a 6-month period in 2012-2013. Prior to initiating a CTO-PCI program, the operator attended one live CTO case course on 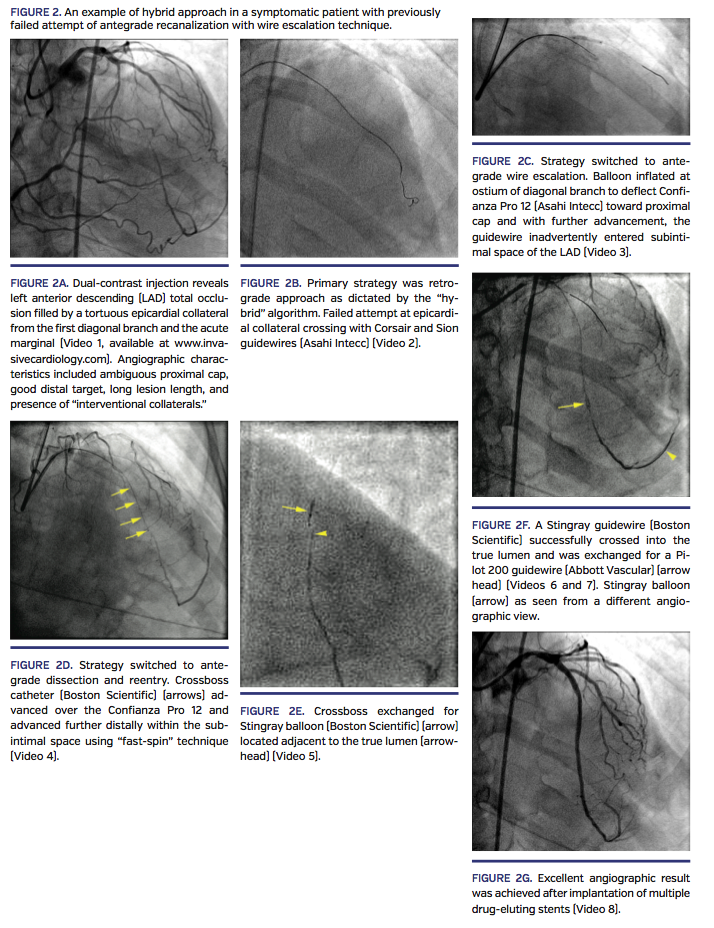 the “hybrid” approach and had two separate full-day on-site proctorships, during which 4 patients were treated and were included in the present analysis. All cases were treated using the “hybrid” approach.8 An example of such an approach is illustrated by Figure 2.
the “hybrid” approach and had two separate full-day on-site proctorships, during which 4 patients were treated and were included in the present analysis. All cases were treated using the “hybrid” approach.8 An example of such an approach is illustrated by Figure 2.
Baseline clinical and angiographic characteristics, procedural techniques, and in-hospital outcomes were examined.
Study endpoints and definitions. Chronic total occlusion was defined as a coronary occlusion with an estimated duration of at least 3 months based on previous angiogram, perfusion study, symptom onset, and previous myocardial infarction (MI). Technical success was defined as achievement of a patent vessel with <30% residual stenosis and TIMI 3 flow. Procedural success was defined as technical success without in-hospital MI, urgent repeat revascularization, or death. The J-CTO score was estimated as described by Morino et al.13 Post-PCI myocardial infarction was defined as two out of the three following criteria: (1) ischemic symptoms; (2) an increase in creatine kinase (CK) >3 times the upper limit of normal; and (3) ischemic changes on an electrocardiogram. Cardiac enzymes were routinely performed 12 hours post procedure. In-hospital efficacy endpoints included major adverse cardiac events, defined as a composite of in-hospital death, MI, repeat coronary revascularization, or stroke. Significant coronary perforation was defined as perforation requiring pericardiocentesis, embolization, or stent graft placement. Stent thrombosis was defined using the Academic Research Consortium standards.14 Vascular complications were defined as >5 cm hematoma and/or retroperitoneal bleed.
Statistical methods. Summary statistics were reported as mean ± standard deviation for normally distributed continuous variables or median and interquartile range (IQR) for non-normally distributed data. Discrete variables were presented as counts and percentages. All analyses were performed according to the intention-to-treat principle.
Results
Patient and lesion characteristics. Between 2012 and 2013, a total of 48 patients underwent 50 consecutive CTO-PCI procedures by a single operator (MV). No patients were refused based on angiographic 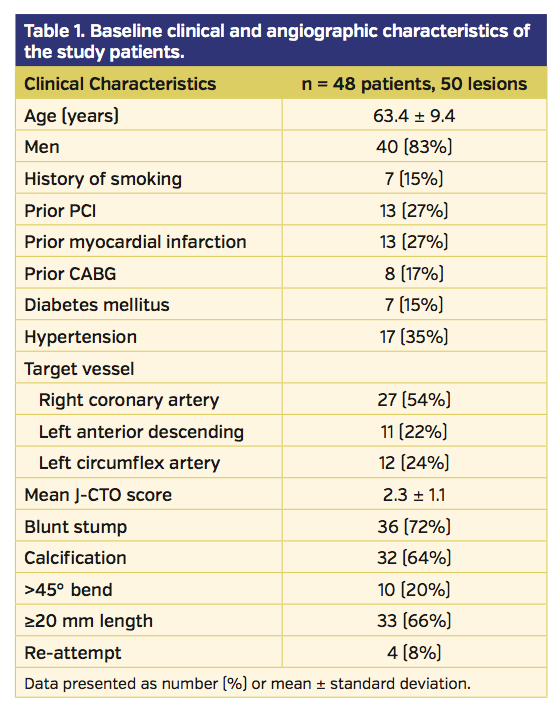 findings. The clinical and angiographic characteristics of the study patients and lesions are presented in Table 1. Most patients were men (83%), with a mean age of 63.4 ± 9.4 years. The indications for CTO-PCI included symptoms, large ischemic burden, and significant ventricular arrhythmia. Of the study patients, 17% had a history of coronary artery bypass surgery (CABG). The right coronary artery was the most common CTO target vessel (54%). Attempted CTOs were highly complex (mean J-CTO score, 2.3) with high prevalence of calcification (64%), blunt stump (72%), and ≥20 mm length (66%).
findings. The clinical and angiographic characteristics of the study patients and lesions are presented in Table 1. Most patients were men (83%), with a mean age of 63.4 ± 9.4 years. The indications for CTO-PCI included symptoms, large ischemic burden, and significant ventricular arrhythmia. Of the study patients, 17% had a history of coronary artery bypass surgery (CABG). The right coronary artery was the most common CTO target vessel (54%). Attempted CTOs were highly complex (mean J-CTO score, 2.3) with high prevalence of calcification (64%), blunt stump (72%), and ≥20 mm length (66%).
Procedural characteristics and outcomes. Procedural details and outcomes are detailed in Table 2. Overall, technical success (successful recanalization) was achieved in 92% of cases; procedural success was also 92%. A retrograde approach was the primary strategy in 33% of successful cases, while the antegrade strategy was used in 67% of cases. The most traversed collateral vessels were septals (47%), epicardials (40%), and saphenous vein bypass grafts (13%). Utilizing the hybrid algorithm, the primary strategy was effective in 65% of cases. Thirty-five percent of cases required one change in strategy and 15% required two strategy changes. There was an average of 7 guidewires used per case (IQR, 4-8 guidewires) and an average of 5 balloons used (IQR, 4-7.5 balloons). The median number of drug-eluting stents implanted was 3 (IQR, 2-4 stents) with a median length of 73 mm (IQR, 38-96 mm). Mean total procedure time was 146.1 ± 65.7 minutes and the mean iodinated contrast volume was 356.4 ± 148.3 mL. Mean total fluoroscopy time and air kerma radiation exposure were 63.0 ± 36.9 minutes and 3.5 ± 2.0 Gy, respectively.
required two strategy changes. There was an average of 7 guidewires used per case (IQR, 4-8 guidewires) and an average of 5 balloons used (IQR, 4-7.5 balloons). The median number of drug-eluting stents implanted was 3 (IQR, 2-4 stents) with a median length of 73 mm (IQR, 38-96 mm). Mean total procedure time was 146.1 ± 65.7 minutes and the mean iodinated contrast volume was 356.4 ± 148.3 mL. Mean total fluoroscopy time and air kerma radiation exposure were 63.0 ± 36.9 minutes and 3.5 ± 2.0 Gy, respectively.
Procedural complications and in-hospital outcomes. There were no in-hospital deaths, MIs, or urgent repeat revascularizations. Procedural complications and in-hospital outcomes are detailed in Table 3. There were 2 significant perforations requiring treatment, each of which occurred with retrograde approach. Both were treated successfully (1 with a covered stent and the other with contour embolization particles). No patients developed cardiac tamponade. No patients required emergent CABG or cardiac surgery. There were 3 cases of vascular site complication, including 2 hematomas and 1 bilateral retroperitoneal bleed. All of these cases were treated conservatively and no blood transfusions or vascular procedures were required. There was 1 case of left main dissection during a left anterior descending CTO-PCI treated with stenting without adverse outcome. During a retrograde approach, there was 1 case of aortic dissection that did not require any treatment once the target CTO vessel was 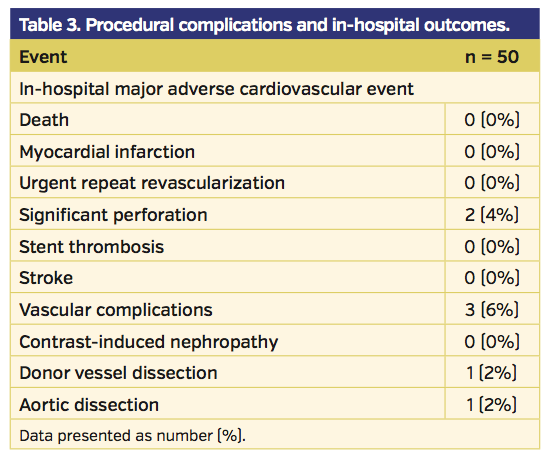 revascularized.
revascularized.
Discussion
The main finding of our study is that the “hybrid” approach to CTO-PCI can be safely adopted by a new CTO operator over a short period of time with high success and low complication rates. In fact, the overall success rate was 92% with 0% in-hospital MACE rate despite treating complex CTO lesions, as evidenced by an average J-CTO score of 2.3. Success rate for CTO-PCI has traditionally been low (60%-70%), especially early in the CTO-PCI learning curve and in lesions with unfavorable characteristics, such as calcification, long length, and blunt proximal cap.15-17 Experienced CTO operators have acknowledged the steep learning curve of approximately 200-300 CTO-PCI procedures before achieving high success rate, with recommendation of a minimum of 50 procedures per year to maintain competency.7,15 Recent advances in CTO crossing techniques, including the retrograde approach,7,18 coupled with antegrade dissection/reentry devices,19,20 have significantly increased contemporary success rates.9,10,13,21,22 However, adoption of CTO-PCI remains low due to lack of an effective standardized method of transmitting and teaching the needed CTO-PCI skillsets until recently.23 The “hybrid” approach is an algorithmic approach designed to systematically integrate all available techniques and technologies to provide a standardized approach to CTO-PCI (Figures 1 and 2). This approach focuses on safety, reproducibility, efficiency, and success. Recent studies have shown the adoption of this approach to yield high success rates, high efficiency, and low complication rates.9-12 These studies involved highly experienced operators with many years of experience in CTO devices and techniques. To date, there are no published studies on feasibility of adoption of the “hybrid” approach by an operator without prior CTO-PCI experience. In this study, we were able to achieve a high success rate in the first 50 procedures with no case-selection bias. All these were consecutive cases referred based on angina symptom or large ischemic burden, and no cases were rejected based on clinical or anatomical features. There was a high number of patients with prior CABG, which has been shown to be associated with lower technical success rates.24 The lesions encountered were rather complex, with the majority of lesions treated having characteristics associated with failure such as calcification, long lesion length, and non-tapered proximal cap.25 Despite these challenges, we were able to accomplish high success rates by adopting the “hybrid” strategy.
Becoming a CTO operator requires significant motivation, dedication, and commitment to long-term ongoing training in CTO-PCI techniques. Since these techniques are not taught during fellowship and are not used in routine coronary interventions, the operator and participating catheterization laboratory staff must learn new techniques that are not widely available. Therefore, education is mandatory in the form of both formal didactic educational programs and on-site proctorship. Our CTO operator spent a significant amount of time reading CTO literature to become familiar with CTO equipment, techniques, and practice patterns from expert centers. More time was then committed to completing teaching modules and watching numerous live-recorded cases on www.ctofundamentals.org. This website also provided a means of interaction with world experts in the form of a discussion forum and case sharing. Our operator subsequently attended a live “hybrid” CTO case course followed by two separate on-site proctorship visits. Prior to these visits, we adopted the concept of a dedicated CTO day, where one day a week was dedicated to performing CTO procedures only. Therefore, no ad hoc CTO-PCIs were performed and this allowed time for proper patient and procedure preparations. Ongoing education involved attending international meetings and establishing a close relationship with both proctor and CTO experts. Mentoring from world experts cannot be overemphasized and is a critical component in becoming an expert CTO operator. We also established a local database for quality assurance and to ensure our practice pattern was similar to expert centers.
Consistent with prior studies, we used the retrograde approach in approximately one-third of cases, with the septal collateral being most commonly used for retrograde access; however, our use of epicardial collaterals was higher.12,17,21,26 Epicardial collaterals are more prone to catastrophic perforation. We had 2 significant perforations without clinical tamponade; 1 perforation was treated with a single covered stent and the other was treated with embolization particles. Although there is no guideline, the general consensus from CTO experts is to avoid using epicardial collaterals until an operator has completed at least 50 retrograde procedures. However, this requirement may be individualized and our operator felt comfortable using epicardial collaterals after several retrograde procedures utilizing septal collaterals. It should be emphasized that prior to attempting epicardial collateral crossing, an operator must be extremely familiar with equipment and treatments for perforation. There are concerns that CTO-PCI is associated with higher periprocedural major complications, especially with the retrograde approach.22,27 However, registries and meta-analyses have shown that complication rates remain low.4,13,16,22 In our series, despite the high use of retrograde approach and epicardial collaterals, major procedural complications were very low and were comparable to recently published studies. We had no deaths, MIs, or urgent repeat revascularizations. Most of our complications were vascular complications, all of which were treated conservatively without adverse outcomes.
The numbers of wires, balloons, and stents used were higher compared to non-CTO PCI, illustrating higher resource utilization confirmed by a recent cost-utilization outcome study.12 Therefore, support from hospital administration is required and can be achieved by emphasizing the clinical benefit of CTO-PCI. Moreover, CTO-PCI has been shown to be cost effective.28 Our procedure times, fluoroscopy times, total radiation doses, and average contrast volumes compare favorably with a recent study from an established CTO center.12 Prior to starting CTO-PCIs, we established general local guidelines related to radiation exposure, contrast utilization, and anticoagulation use and monitoring. The procedure is aborted if the lesion is not crossed by 6-8 Gy of radiation or if 10-12 Gy is reached. If the patient has received >5 Gy radiation, education on radiation injury is provided and a letter is sent to the primary care physician. During the CTO procedure, heparin is used for anticoagulation and activated clotting time is checked every 30 minutes along with verbal reporting on total contrast volume and cumulative radiation dose.
Study limitations. This study is an observational, single-operator study and may not be applicable to all PCI operators. This is a highly experienced operator with high volume and experience in advanced PCI techniques. Both didactic (live case course) and hands-on (proctoring) training were performed during initiation of the CTO-PCI program, along with tireless support and mentoring from world CTO experts. There is potential case-selection bias with other confounding factors that may influence clinical outcomes. Furthermore, procedural outcomes were not independently adjudicated. Regarding selection bias, this report represents consecutive patients who were referred for CTO-PCI, with no patients excluded due to either unfavorable angiographic or clinical characteristics. Our analysis did not allow outcome comparisons between CTO and non-CTO cohorts. Lastly, since the single operator in the present study did not perform any significant amount of CTO-PCIs prior to adoption of the hybrid approach, it is not possible to compare outcomes before and after program adoption.
Conclusion
CTO-PCI is technically challenging and requires dedication, commitment, and adequate early training to achieve high success rates.29 One significant reason why it has been difficult to disseminate CTO-PCI techniques is the lack of a structured and standardized teaching method. The “hybrid” algorithm has been designed to fill this void in the CTO sphere. The algorithm offers a systematic approach to CTO-PCI that is teachable and reproducible, and focuses on effectiveness, efficiency, and safety. Our findings suggest that the “hybrid” approach to CTO-PCI can facilitate achievement of excellent clinical outcomes not only among experienced centers and operators, but also among novice CTO operators who are dedicated and committed and have mentoring and on-going support from world CTO experts.
Acknowledgment. We would like to thank the “hybrid” CTO community for its significant support and contribution to this manuscript.
References
- Fefer P, Knudtson ML, Cheema AN, et al. Current perspectives on coronary chronic total occlusions: the Canadian Multicenter Chronic Total Occlusions Registry. J Am Coll Cardiol. 2012;59(11):991-997.
- Khan MF, Wendel CS, Thai HM, Movahed MR. Effects of percutaneous revascularization of chronic total occlusions on clinical outcomes: a meta-analysis comparing successful versus failed percutaneous intervention for chronic total occlusion. Catheter Cardiovasc Interv. 2013;82(1):95-107.
- Grantham JA, Jones PG, Cannon L, Spertus JA. Quantifying the early health status benefits of successful chronic total occlusion recanalization: results from the FlowCardia’s Approach to Chronic Total Occlusion Recanalization (FACTOR) trial. Circ Cardiovasc Qual Outcomes. 2010;3(3):284-290.
- Suero JA, Marso SP, Jones PG, et al. Procedural outcomes and long-term survival among patients undergoing percutaneous coronary intervention of a chronic total occlusion in native coronary arteries: a 20-year experience. J Am Coll Cardiol. 2001;38(2):409-414.
- Sirnes PA, Myreng Y, Molstad P, Bonarjee V, Golf S. Improvement in left ventricular ejection fraction and wall motion after successful recanalization of chronic coronary occlusions. Eur Heart J. 1998;19(2):273-281.
- Stone GW, Kandzari DE, Mehran R, et al. Percutaneous recanalization of chronically occluded coronary arteries: a consensus document: part I. Circulation. 2005;112(15):2364-2372.
- Lombardi WL. Retrograde PCI: what will they think of next? J Invasive Cardiol. 2009;21(10):543.
- Brilakis ES, Grantham JA, Rinfret S, et al. A percutaneous treatment algorithm for crossing coronary chronic total occlusions. JACC Cardiovasc Interv. 2012;5(4):367-379.
- Pershad A, Eddin M, Girotra S, Cotugno R, Daniels D, Lombardi W. Validation and incremental value of the hybrid algorithm for CTO PCI. Catheter Cardiovasc Interv. 2014;84(4):654-659. Epub 2014 Feb 4.
- Michael TT, Mogabgab O, Fuh E, et al. Application of the “hybrid approach” to chronic total occlusion interventions: a detailed procedural analysis. J Intervent Cardiol. 2014;27(1):36-43.
- Christopoulos G, Karmpaliotis D, Alaswad K, et al. The efficacy of “hybrid’’ percutaneous coronary intervention in chronic total occlusions caused by in-stent restenosis: insights from a US multicenter registry. Catheter Cardiovasc Intervent. 2014;84(4):646-651. Epub 2014 Jul 4.
- Karmpaliotis D, Lembo N, Kalynych A, et al. Development of a high-volume, multiple-operator program for percutaneous chronic total coronary occlusion revascularization: procedural, clinical, and cost-utilization outcomes. Catheter Cardiovasc Interv. 2013;82(1):1-8.
- Morino Y, Kimura T, Hayashi Y, et al. In-hospital outcomes of contemporary percutaneous coronary intervention in patients with chronic total occlusion insights from the J-CTO Registry (Multicenter CTO Registry in Japan). JACC Cardiovasc Interv. 2010;3(2):143-151.
- Cutlip DE, Windecker S, Mehran R, et al. Clinical end points in coronary stent trials: a case for standardized definitions. Circulation. 2007;115(17):2344-2351.
- Di Mario C, Werner GS, Sianos G, et al. European perspective in the recanalisation of Chronic Total Occlusions (CTO): consensus document from the EuroCTO Club. EuroIntervention. 2007;3(1):30-43.
- Patel VG, Brayton KM, Tamayo A, et al. Angiographic success and procedural complications in patients undergoing percutaneous coronary chronic total occlusion interventions: a weighted meta-analysis of 18,061 patients from 65 studies. JACC Cardiovasc Interv. 2013;6(2):128-136.
- Thompson CA, Jayne JE, Robb JF, et al. Retrograde techniques and the impact of operator volume on percutaneous intervention for coronary chronic total occlusions an early US experience. JACC Cardiovasc Interv. 2009;2(9):834-842.
- Surmely JF, Katoh O, Tsuchikane E, Nasu K, Suzuki T. Coronary septal collaterals as an access for the retrograde approach in the percutaneous treatment of coronary chronic total occlusions. Catheter Cardiovasc Interv. 2007;69(6):826-832.
- Whitlow PL, Burke MN, Lombardi WL, et al. Use of a novel crossing and re-entry system in coronary chronic total occlusions that have failed standard crossing techniques: results of the FAST-CTOs (Facilitated Antegrade Steering Technique in Chronic Total Occlusions) trial. JACC Cardiovasc Interv. 2012;5(4):393-401.
- Whitlow PL, Lombardi WL, Araya M, et al. Initial experience with a dedicated coronary re-entry device for revascularization of chronic total occlusions. Catheter Cardiovasc Interv. 2012;80(5):807-813.
- Yamane M, Muto M, Matsubara T, et al. Contemporary retrograde approach for the recanalisation of coronary chronic total occlusion: on behalf of the Japanese Retrograde Summit Group. EuroIntervention. 2013;9(1):102-109.
- Galassi AR, Tomasello SD, Reifart N, et al. In-hospital outcomes of percutaneous coronary intervention in patients with chronic total occlusion: insights from the ERCTO (European Registry of Chronic Total Occlusion) registry. EuroIntervention. 2011;7(4):472-479.
- Smith EJ, Strange JW, Hanratty CG, Walsh SJ, Spratt JC. Percutaneous intervention for chronic total occlusion: integrating strategies to address an unmet need. Heart. 2013;99(20):1471-1474.
- Michael TT, Karmpaliotis D, Brilakis ES, et al. Impact of prior coronary artery bypass graft surgery on chronic total occlusion revascularisation: insights from a multicentre US registry. Heart. 2013;99(20):1515-1518.
- Morino Y, Abe M, Morimoto T, et al. Predicting successful guidewire crossing through chronic total occlusion of native coronary lesions within 30 minutes: the J-CTO (Multicenter CTO Registry in Japan) score as a difficulty grading and time assessment tool. JACC Cardiovasc Interv. 2011;4(2):213-221.
- Lee NH, Seo HS, Choi JH, Suh J, Cho YH. Recanalization strategy of retrograde angioplasty in patients with coronary chronic total occlusion —analysis of 24 cases, focusing on technical aspects and complications. Int J Cardiol. 2010;144(2):219-229.
- Patel VG, Michael TT, Mogabgab O, et al. Clinical, angiographic, and procedural predictors of periprocedural complications during chronic total occlusion percutaneous coronary intervention. J Invasive Cardiol. 2014;26(3):100-105.
- Gada H, Whitlow PL, Marwick TH. Establishing the cost-effectiveness of percutaneous coronary intervention for chronic total occlusion in stable angina: a decision-analytic model. Heart. 2012;98(24):1790-1797.
- Stojkovic S, Sianos G, Katoh O, et al. Efficiency, safety, and long-term follow-up of retrograde approach for CTO recanalization: initial (Belgrade) experience with international proctorship. J Intervent Cardiol. 2012;25(6):540-548.
______________________________________
From the 1Section of Cardiology, St. Boniface Hosipital, University of Manitoba, Winnipeg, Canada; 2Division of Cardiology, University of Washington, Seattle, Washington; 3 VA North Texas Healthcare System and University of Texas Southwestern Medical Center, Dallas, Texas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Vo reports speaking fees, travel, and honoraria from Boston Scientific. Dr McCabe reports personal fees from Abbott Vascular. Dr Lombardi reports consulting fees/speaker honoraria from Boston Scientific, Abbott Vascular, Medtronic CardioVascular, and Terumo Medical; spouse is an employee of Spectranetics. Dr. Brilakis reports consulting fees/speaker honoraria from St Jude Medical, Boston Scientific, Asahi, Janssen, Sanofi, Abbott Vascular, Elsevier, and Terumo; research support from Guerbet; spouse is an employee of Medtronic. The remaining authors report no disclosures.
Manuscript submitted July 10, 2014, provisional acceptance given September 11, 2014, final version accepted September 19, 2014.
Address for correspondence: Dr Minh N. Vo, Y3-409 Tache Ave, R2H 2A6, Winnipeg, Manitoba, Canada. Email: mvo@sbgh.mb.ca











