

Atresia of the Left Internal Mammary Artery Graft Following Percutaneous Intervention of the Left Main
ABSTRACT: Because of its durability and patency, the left internal mammary artery (LIMA) is preferentially used to bypass obstructive lesions in the left main coronary artery (LMCA) and/or the left anterior descending coronary artery (LAD). The long-term patency of the LIMA graft is determined by several factors, principal among them being the dynamic competition between flow through the internal mammary artery graft and the LAD. We report a patient with LMCA stenosis and a well-functioning and mature LIMA graft, who after percutaneous intervention of the LMCA and normalized antegrade flow in the LAD, developed atresia of a large caliber LIMA graft.
J INVASIVE CARDIOL 2011;23(12):E284-E287
Key words: internal mammary artery, saphenous vein graft, native coronary artery, patency, competitive flow
_________________________________________
 The left internal mammary artery (LIMA) has been shown to be an excellent conduit for grafting the left main coronary artery (LMCA) or left anterior descending coronary artery (LAD) in terms of its remarkably high patency rates and absence of graft atherosclerosis.1,2 After surgical implantation, initial blood flow intra-operatively through the LIMA graft is relatively low compared with saphenous vein graft (SVG) flow.3 There is progressive increase in LIMA blood flow over the next several months; this improvement is felt to be due to arterial remodeling. A mature LIMA graft can thus accommodate maximal blood flow to the LAD territory. It is less certain as to the fate of the LIMA graft if flow through a diseased LAD is restored as this clinical scenario is rarely seen.
The left internal mammary artery (LIMA) has been shown to be an excellent conduit for grafting the left main coronary artery (LMCA) or left anterior descending coronary artery (LAD) in terms of its remarkably high patency rates and absence of graft atherosclerosis.1,2 After surgical implantation, initial blood flow intra-operatively through the LIMA graft is relatively low compared with saphenous vein graft (SVG) flow.3 There is progressive increase in LIMA blood flow over the next several months; this improvement is felt to be due to arterial remodeling. A mature LIMA graft can thus accommodate maximal blood flow to the LAD territory. It is less certain as to the fate of the LIMA graft if flow through a diseased LAD is restored as this clinical scenario is rarely seen.
We describe the effect of percutaneous coronary intervention (PCI) performed on the LMCA on the internal mammary artery (IMA) graft in a patient who presented with new onset angina.
 Case Report. A 65-year-old male with hypertension and hyperlipidemia was admitted for worsening angina. Angiography showed an isolated 80% ostial left main stenosis (Figures 1A and 1B). He underwent coronary artery bypass graft surgery (CABG) with a sequential LIMA to the distal LAD and the first diagonal artery without SVG grafting to the circumflex. The patient was asymptomatic for 3 months, after which he developed progressive, exertional angina despite optimal medical management. Six months after CABG, angiography showed the
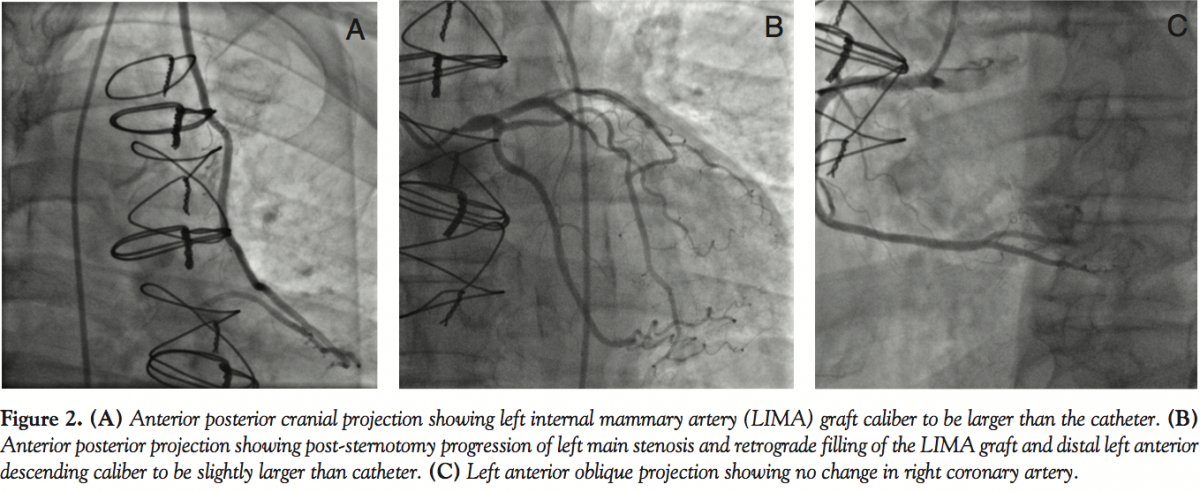
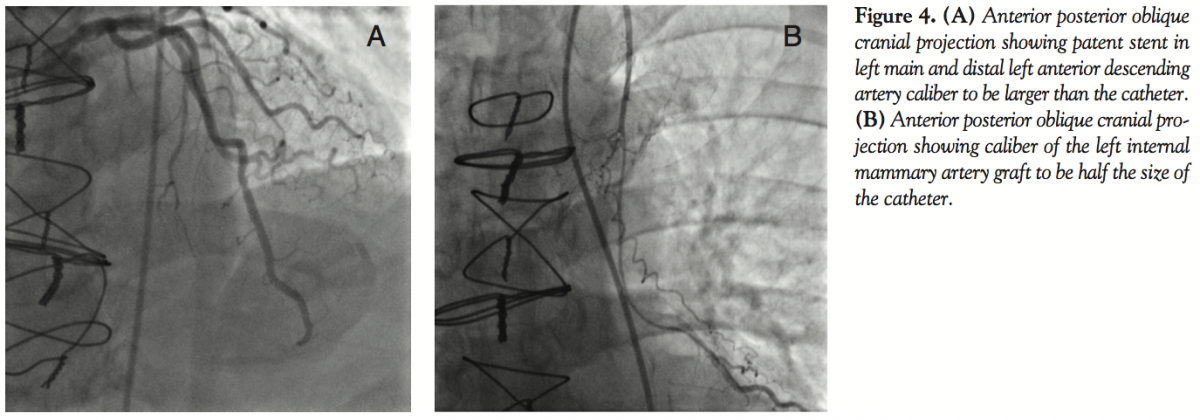
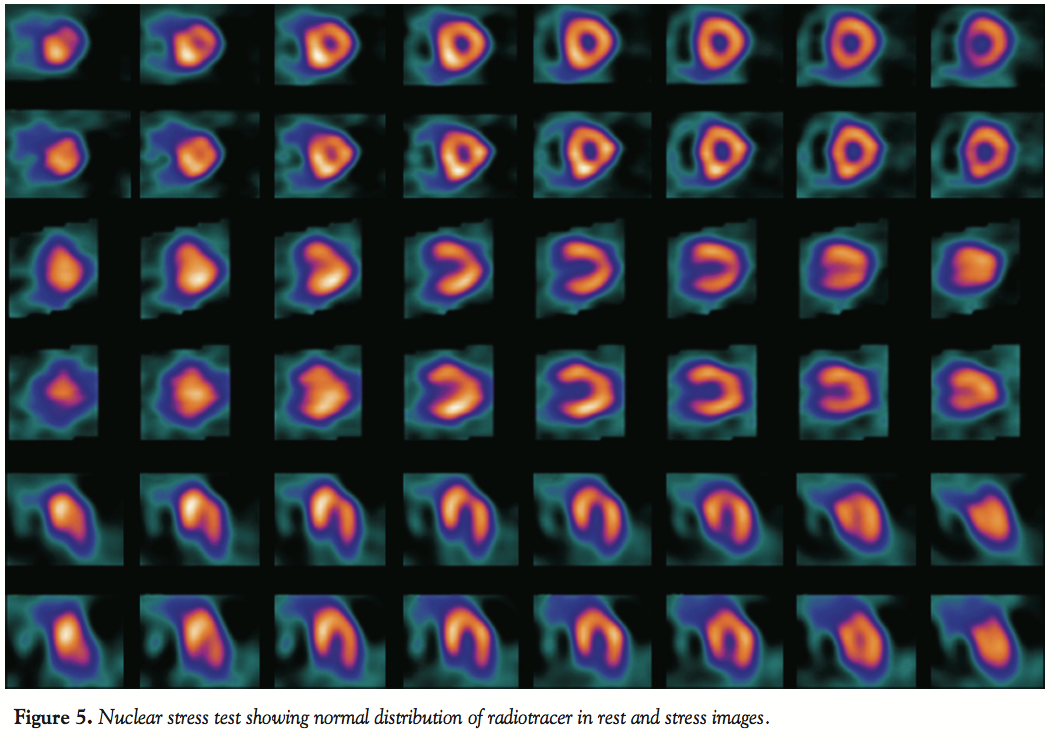
Case Report. A 65-year-old male with hypertension and hyperlipidemia was admitted for worsening angina. Angiography showed an isolated 80% ostial left main stenosis (Figures 1A and 1B). He underwent coronary artery bypass graft surgery (CABG) with a sequential LIMA to the distal LAD and the first diagonal artery without SVG grafting to the circumflex. The patient was asymptomatic for 3 months, after which he developed progressive, exertional angina despite optimal medical management. Six months after CABG, angiography showed the 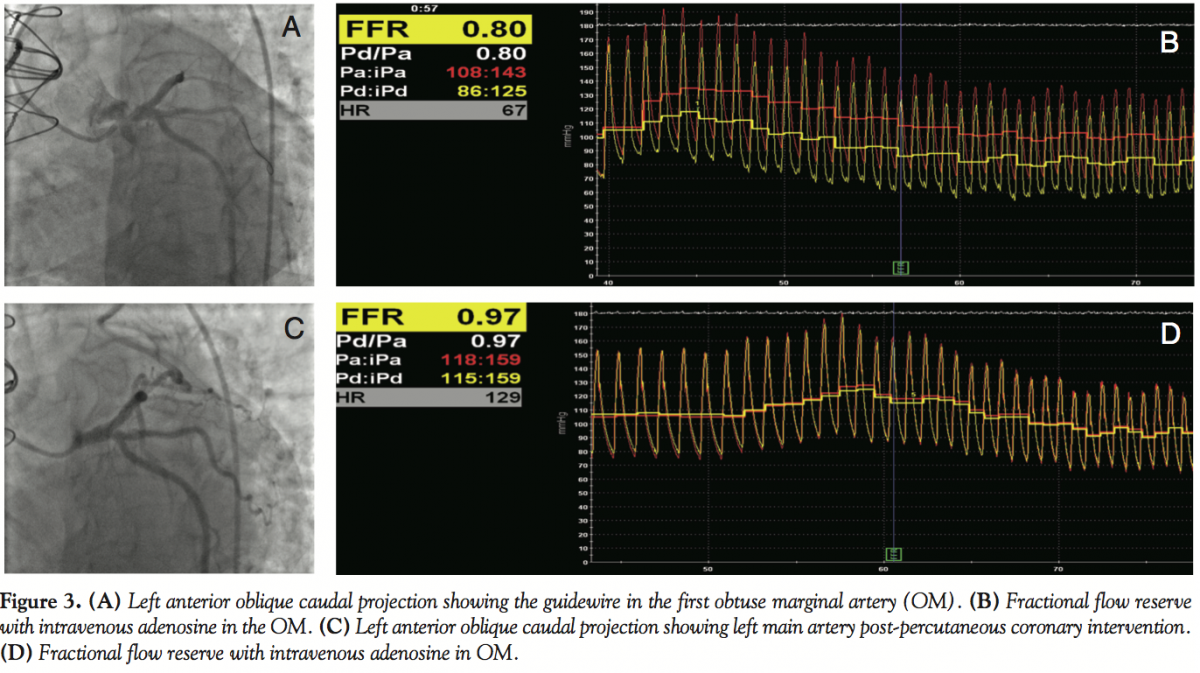 LIMA graft to be patent (Figure 2A). The ostial stenosis in the LMCA had progressed to 90% (Figure 2B) with no other new findings (Figure 2C). Because of worsening symptoms, increase in the LMCA stenosis and pressure dampening with catheter, fractional flow reserve (FFR) was performed to determine the physiologic significance of this lesion. With the pressure transducer in the obtuse marginal (OM) artery (Figure 3A), FFR using intravenous adenosine was 0.80 (Figure 3B). A bare-metal stent was implanted in the LMCA (Figure 3C). Postintervention FFR was 0.97 (Figure 3D). At 4-week follow-up, the patient was asymptomatic. The patient presented with atypical chest pain 3 months after PCI. Angiography showed a patent LMCA stent (Figure 4A) with significant atresia of the entire length of the LIMA graft (Figure 4B). He was maintained on aggressive medical management. Nuclear stress test done 6 months later showed no evidence of ischemia (Figure 5).
LIMA graft to be patent (Figure 2A). The ostial stenosis in the LMCA had progressed to 90% (Figure 2B) with no other new findings (Figure 2C). Because of worsening symptoms, increase in the LMCA stenosis and pressure dampening with catheter, fractional flow reserve (FFR) was performed to determine the physiologic significance of this lesion. With the pressure transducer in the obtuse marginal (OM) artery (Figure 3A), FFR using intravenous adenosine was 0.80 (Figure 3B). A bare-metal stent was implanted in the LMCA (Figure 3C). Postintervention FFR was 0.97 (Figure 3D). At 4-week follow-up, the patient was asymptomatic. The patient presented with atypical chest pain 3 months after PCI. Angiography showed a patent LMCA stent (Figure 4A) with significant atresia of the entire length of the LIMA graft (Figure 4B). He was maintained on aggressive medical management. Nuclear stress test done 6 months later showed no evidence of ischemia (Figure 5).
 Discussion. This patient illustrates the widely held notion that increasing competitive flow through a native artery grafted with LIMA leads to atresia and failure of the graft.4 Controversy exists in the literature with regard to long-term patency of the LIMA graft in the presence of patent, native coronary arteries. Competitive flow between a native coronary artery/a saphenous vein graft and the LIMA graft, is widely believed to be the major determinant of the long-term patency of the LIMA graft.5-7 Nordgaard et al reported the results of an experiment in a porcine model suggesting that the degree of competitive flow determines the patency of the LIMA graft.8 Their conclusion was based on the observation that wall shear stress is lowest in the model with high competitive flow. Retrospective analysis of approximately 2000 LIMA grafts by Sabik et al9 showed patency rates of 92% at 15 years of follow-up. LIMA occlusion was related to lesser degree of proximal, native artery stenosis. However, there was no “threshold” percent stenosis above which graft failure was clearly higher. It has also been reported that congenital fistulas draining flow from LIMA proximal to LAD anastomosis can contribute to diminished flow and subsequent shrinkage of the graft.10 Animal experiments also suggested that the anatomic location of the LIMA graft touchdown in relation to the length of the native vessel may be a determining factor in its patency rates.11
Discussion. This patient illustrates the widely held notion that increasing competitive flow through a native artery grafted with LIMA leads to atresia and failure of the graft.4 Controversy exists in the literature with regard to long-term patency of the LIMA graft in the presence of patent, native coronary arteries. Competitive flow between a native coronary artery/a saphenous vein graft and the LIMA graft, is widely believed to be the major determinant of the long-term patency of the LIMA graft.5-7 Nordgaard et al reported the results of an experiment in a porcine model suggesting that the degree of competitive flow determines the patency of the LIMA graft.8 Their conclusion was based on the observation that wall shear stress is lowest in the model with high competitive flow. Retrospective analysis of approximately 2000 LIMA grafts by Sabik et al9 showed patency rates of 92% at 15 years of follow-up. LIMA occlusion was related to lesser degree of proximal, native artery stenosis. However, there was no “threshold” percent stenosis above which graft failure was clearly higher. It has also been reported that congenital fistulas draining flow from LIMA proximal to LAD anastomosis can contribute to diminished flow and subsequent shrinkage of the graft.10 Animal experiments also suggested that the anatomic location of the LIMA graft touchdown in relation to the length of the native vessel may be a determining factor in its patency rates.11
 There are other data that are not consistent with the concept of diminished or competitive flow as a major factor in graft atresia. In a canine experimental preparation, no evidence of LIMA shriveling was seen when it was grafted to a completely patent coronary artery and flow in the graft was maintained above in situ levels.12 In another canine study examining the consequences of dynamic flow competition between the native vessel and the LIMA graft in a similar model followed for 2 months, LIMA graft flow was maintained above in situ levels. When the native artery was occluded, an increase in flow occurred, i.e., there was a recruitable flow reserve.13
There are other data that are not consistent with the concept of diminished or competitive flow as a major factor in graft atresia. In a canine experimental preparation, no evidence of LIMA shriveling was seen when it was grafted to a completely patent coronary artery and flow in the graft was maintained above in situ levels.12 In another canine study examining the consequences of dynamic flow competition between the native vessel and the LIMA graft in a similar model followed for 2 months, LIMA graft flow was maintained above in situ levels. When the native artery was occluded, an increase in flow occurred, i.e., there was a recruitable flow reserve.13
Compared with SVG, LIMA flow immediately after surgery is low and increases by approximately 30% over the next 3 months, and reaches comparable levels as SVG at about 10 months.3 The putative mechanism has been postulated to be endothelium-dependent vascular remodeling.3 If this were true, it is reasonable to speculate that any factor that interferes with the adaptability mechanism of the LIMA graft during its “maturation” phase, such as increase in blood flow through the native coronary artery because of intervention performed, as in our case, may affect its flow and consequently, its caliber. In our case, the first reported case in man that demonstrates atresia after full LIMA graft maturation, the stimulus for growth was diminished, as was the size of the vessel. We postulate that were LAD flow to decrease again as a result of a new lesion, the LIMA graft would have a further stimulus for growth and its size would enlarge.
In conclusion, this case illustrates the effect of increasing antegrade flow down the LAD, and suggests that the amount of flow is important in the size of the IMA graft.
References
- Kay EB, Naraghipour H, Beg RA, DeManey M, Tambe A, Zimmerman HA. Internal mammary artery bypass graft — long-term patency rate and follow-up. Ann Thorac Surg. 1974;18(3):269-79.
- Tatoulis J, Buxton BF, Fuller JA. Patencies of 2127 arterial to coronary conduits over 15 years. Ann Thorac Surg. 2004;77(1):93-101.
- Walpoth BH, Schmid M, Schwab A, et al. Vascular adaptation of the internal thoracic artery graft early and late after bypass surgery. J Thorac Cardiovasc Surg. 2008;136(4):876-883.
- Reddy PR, Bakhos M, Leya F. Regional variation in the reconstitution of flow in the internal mammary artery graft. J Card Surg. 2008;23(1):63-65.
- Berger A, MacCarthy PA, Vanermen H, De Bruyne B. Occlusion of internal mammary grafts: a review of the potential causative factors. Acta Chir Belg. 2004;104(6):630-634.
- Kawamura M, Nakajima H, Kobayashi J, et al. Patency rate of the internal thoracic artery to the left anterior descending artery bypass is reduced by competitive flow from the concomitant saphenous vein graft in the left coronary artery. Eur J Cardiothorac Surg. 2008;34(4):833-838.
- Bach RG, Kern MJ, Donohue TJ, Aguirre FV, Caracciolo EA. Comparison of phasic blood flow velocity characteristics of arterial and venous coronary artery bypass conduits. Circulation. 1993;88(5 Pt 2):II133-II140.
- Norgaard H, Swillens A, Nordhaug D, et al. Impact of competitive flow on wall shear stress in coronary surgery: computational fluid dynamics of a LIMA-LAD model. Cardiovasc Res. 2010;88(3):512-519.
- Sabik JF III, Lytle BW, Blackstone EH, Khan M, Houghtaling PL, Cosgrove DM. Does competitive flow reduce internal thoracic artery graft patency? Eur J Cardiothorac Surg. 2008;34(5):833-838.
- Reiss FC, Lehmann C, Loewer C, Schofer J, Bleese N. Congenital fistula between the left internal mammary artery (LIMA) and the pulmonary artery: cause of LIMA bypass occlusion? Heart Surg Forum. 2004;7(5):E403-E404.
- Pagni S, Salloum E, Storey J, et al. Double grafting of the left anterior descending artery: is the distance between the internal mammary artery and supplemental vein graft anastomoses relevant in graft survival? Eur J Cardiothorac Surg.1998;13(1):36-41.
- Spence PA, Lust RM, Zeri RS, et al. Competitive flow from a fully patent coronary artery does not limit acute mammary graft flow. Ann Thorac Surg. 1992;54(1):21-25.
- Lust RM, Zeri RS, Spence PA, et al. Effect of chronic native flow competition on internal thoracic artery grafts. Ann Thorac Surg. 1994;57(1):45-50.
_________________________________________
From the Department of Medicine, Division of Cardiology, Central Arkansas Veterans Healthcare System and University of Arkansas for Medical Sciences, Little Rock, Arkansas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr. Sachdeva is on the speaker’s bureau for Volcano Corporation. Drs. Kalaga and Uretsky report no disclosures.
Manuscript submitted April 4, 2011 and accepted July 11, 2011.
Address for correspondence: Rajesh Sachdeva, MD, 4300 W 7th Street, Little Rock, AR 72205. Email: rrsachdeva@gmail.com











