

"Candy Cane" Guide Catheter Extension for Stent Delivery
Abstract: Stent delivery to a native coronary artery lesion located proximal to the anastomosis of a bypass graft can be challenging due to severe tortuosity. Guide catheter extensions, such as the GuideLiner, can facilitate equipment delivery. In the presented case, a 180° anastomotic bend in the saphenous vein graft resulted in several failed attempts at stent delivery. A 6 Fr guide catheter extension was then advanced through the extreme angulation at the SVG anastomosis using a distal-anchor technique and assuming a “candy cane” configuration, enabling stent delivery.
J INVASIVE CARDIOL 2015;27(8):E169-E170
Key words: new technique, guide catheter extension, GuideLiner, Guidezilla
___________________
Case Report
A 76-year-old man with prior coronary artery bypass graft surgery presented with stable angina. Diagnostic coronary angiography demonstrated patent saphenous vein grafts (SVGs) to the first diagonal (Figure 1A), distal left anterior descending artery, and the right posterior descending artery. The mid-left anterior descending artery filled retrograde via the saphenous vein graft to the first diagonal branch; however, a severe lesion was present proximal to the SVG anastomosis (Figure 1A, arrow). The SVG to diagonal was engaged with an 8 Fr AL1 guide catheter and wired retrograde with a Runthrough guidewire (Terumo Corporation) using a Venture deflecting tip catheter (Vascular Solutions). The lesion was predilated with a 2.0 x 12 mm balloon (Figure 1B, arrowhead); however, no stent could negotiate the 180º anastomotic bend. An 8 Fr guide catheter extension (GuideLiner; Vascular Solutions) (Figure 1C, arrow) was advanced to the SVG anastomosis, enabling delivery of a 2.5 x 12 mm everolimus-eluting stent that covered the distal part of the lesion; however, a proximal lesion remained (Figure 1D, arrow). In spite of multiple balloon predilations, and use of a buddy wire, no 2.5 x 8 mm stent could be delivered past the SVG anastomosis (stents from all available manufacturers were tried without success). The 8 Fr guide catheter extension was exchanged for a 6 Fr version that negotiated the 180º anastomotic turn by using a distal anchor technique, successfully reaching the target lesion after assuming a “candy cane” shape (Figure 1E, arrow). A 2.5 x 8 mm everolimus-eluting stent was then easily delivered to the target lesion with an excellent final angiographic result (Figure 1F, arrow).
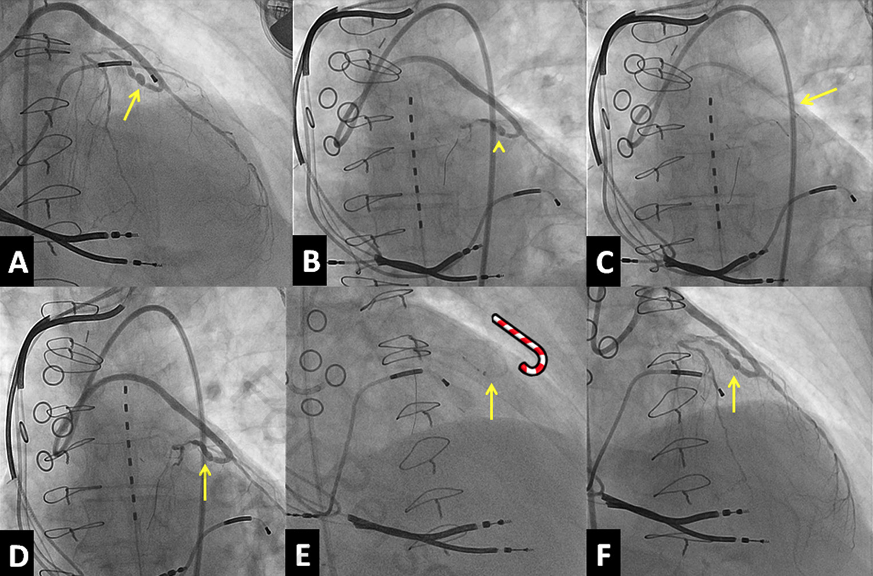 FIGURE 1. (A) Coronary angiography demonstrating a severe lesion proximal to the anastomosis of a saphenous vein graft to the first diagonal branch (arrow). (B) The lesion was predilated with a balloon delivered retrogradely (arrowhead), but no stent could be delivered. (C) After an 8 Fr guide catheter extension (arrow) was advanced to the SVG anastomosis, a 2.5 x 12 mm everolimus-eluting stent was delivered to the lesion; (D) however, the proximal part of the lesion (arrow) was not covered. (E) A stent could not be delivered, so a 6 Fr guide catheter extension was advanced to the lesion using a distal-anchor technique and assuming a “candy cane” configuration. (F) The stent was deployed with an excellent final angiographic result and remarkable symptomatic improvement of the patient.
FIGURE 1. (A) Coronary angiography demonstrating a severe lesion proximal to the anastomosis of a saphenous vein graft to the first diagonal branch (arrow). (B) The lesion was predilated with a balloon delivered retrogradely (arrowhead), but no stent could be delivered. (C) After an 8 Fr guide catheter extension (arrow) was advanced to the SVG anastomosis, a 2.5 x 12 mm everolimus-eluting stent was delivered to the lesion; (D) however, the proximal part of the lesion (arrow) was not covered. (E) A stent could not be delivered, so a 6 Fr guide catheter extension was advanced to the lesion using a distal-anchor technique and assuming a “candy cane” configuration. (F) The stent was deployed with an excellent final angiographic result and remarkable symptomatic improvement of the patient.
Discussion
Delivering stents to a native coronary artery lesion located proximal to the anastomosis of a bypass graft can be challenging due to severe tortuosity. Guide catheter extensions, such as the GuideLiner (available in 5.5 Fr, 6 Fr, 7 Fr, and 8 Fr sizes) and Boston Scientific’s Guidezilla (available in 6 Fr size only), can facilitate equipment delivery.1 In our case, after several attempts to deliver a stent failed, a 6 Fr guide catheter extension was advanced through an area of extreme angulation at the SVG anastomosis, enabling stent delivery. Delivery of the guide catheter extension through the 180º bend required use of the distal-anchor technique2 and carried a risk of dissection; hence, such maneuvers should be performed with extreme caution, and only when other simpler options to achieve equipment delivery have failed.3
References
- Luna M, Papayannis A, Holper EM, Banerjee S, Brilakis ES. Transfemoral use of the GuideLiner catheter in complex coronary and bypass graft interventions. Catheter Cardiovasc Interv. 2012;80:437-446.
- Mahmood A, Banerjee S, Brilakis ES. Applications of the distal anchoring technique in coronary and peripheral interventions. J Invasive Cardiol. 2011;23:291-294.
- Brilakis ES, ed. Manual of Coronary Chronic Total Occlusion Interventions. A Step-By-Step Approach. Waltham, Massachusetts: Elsevier; 2013.
____________________________
From the VA North Texas Health Care System, Dallas, Texas, and the University of Texas Southwestern Medical Center, Dallas, Texas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Brilakis reports consulting fees/speaker honoraria from St. Jude Medical, Boston Scientific, Asahi Intecc, Janssen, Abbott Vascular, Elsevier, Sanofi, and Terumo; research support from Guerbet; spouse is an employee of Medtronic. Drs Repanas and Christopoulos report no conflicts of interest regarding the content herein.
Manuscript submitted August 12, 2014, provisional acceptance given September 8, 2014, final version accepted September 11, 2014.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, VA North Texas Health Care System, Cardiology, 4500 South Lancaster Road, Dallas, TX 75216. Email: esbrilakis@gmail.com











