

Closure of Aorto-Right Ventricular Tunnel With Amplatzer Duct Occluder II
Download a PDF of this article.
ABSTRACT: Aorto-right ventricular tunnel (ARVT) is a very rare, congenital, abnormal extracardiac channel that connects the ascending aorta at or above the sinotubular junction to the cavity of the right ventricle. Only 16 cases have been reported thus far in the English literature. We report the first transcatheter closure of ARVT with the Amplatzer duct occluder II in an infant, with both coronary arteries arising from the left coronary sinus and with biventricular apical non-compaction.
J INVASIVE CARDIOL 2013;25(4):E75-E77
Key words:ARVT, single coronary ostium, transcatheter closure, ADO II
__________________________________________
Aorto-ventricular tunnel is a congenital extracardiac channel that connects the ascending aorta at or above the sinotubular junction to the cavity of the left ventricle (LV) or less commonly the right ventricle (RV). Although more than 130 cases of aorto-left ventricular tunnel (ALVT) have been reported, the ARVT is an extremely rare entity and only 16 cases have been reported so far.1-16 The incidence of ALVT varies from 0.05%-0.46%.17 The anomaly produces a hemodynamically significant left-to-right shunt with resulting pressure and volume overload of the RV.7 We report the first case of a successful transcatheter closure of an ARVT with Amplatzer duct occluder II (ADO II) in an infant with both coronary arteries arising from left coronary sinus and with biventricular apical non-compaction.
Case Description
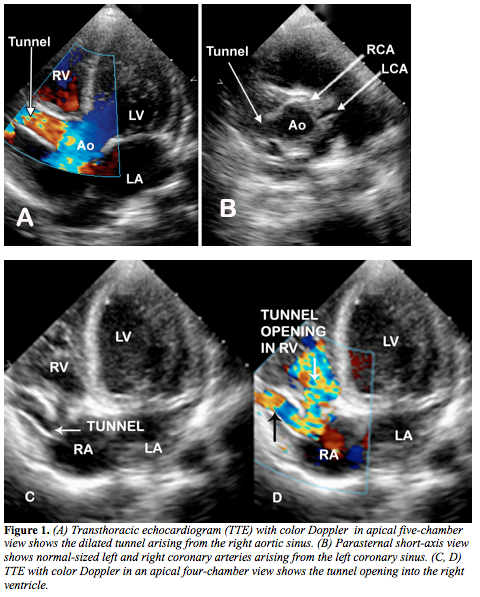 An 11-month-old female was referred by a pediatrician for evaluation of a continuous murmur. On examination, the child weighed 7.5 kg. Pulse was 106/min, collapsing in nature. Blood pressure was 100/20 mm Hg. There was a loud grade 4/6 ‘to and fro’ systolo-diastolic machinery murmur heard in the left-lower sternal border. Electrocardiogram (ECG) was normal. Chest radiograph showed cardiomegaly with apparent enlargement of the right atrium. Transthoracic real-time two-dimensional echocardiography (TTE) and color Doppler in apical five-chamber view showed dilated tunnel arising from the right aortic sinus (Figure 1A).
An 11-month-old female was referred by a pediatrician for evaluation of a continuous murmur. On examination, the child weighed 7.5 kg. Pulse was 106/min, collapsing in nature. Blood pressure was 100/20 mm Hg. There was a loud grade 4/6 ‘to and fro’ systolo-diastolic machinery murmur heard in the left-lower sternal border. Electrocardiogram (ECG) was normal. Chest radiograph showed cardiomegaly with apparent enlargement of the right atrium. Transthoracic real-time two-dimensional echocardiography (TTE) and color Doppler in apical five-chamber view showed dilated tunnel arising from the right aortic sinus (Figure 1A).
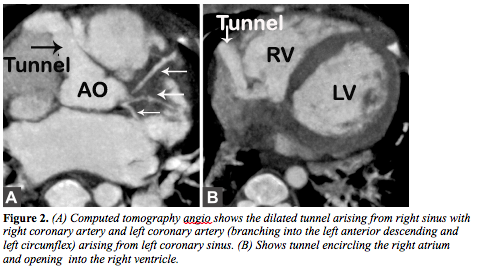 Parasternal short-axis view showed normal-sized left and right coronary arteries arising from left coronary sinus and large tunnel arising from right coronary sinus (Figure 1B). The TTE with color Doppler in the apical four-chamber view showed the tunnel opening into the RV (Figures 1C and 1D). Computed tomographic angiography (CT angio) revealed that the tunnel was arising above the right coronary sinus with both coronary arteries arising from a single left coronary ostium (Figure 2A). The tunnel was draining into the right ventricular infundibulum. (Figure 2B). The origin of the tunnel measured 8.5 mm and the distal RV end measured 6 mm.
Parasternal short-axis view showed normal-sized left and right coronary arteries arising from left coronary sinus and large tunnel arising from right coronary sinus (Figure 1B). The TTE with color Doppler in the apical four-chamber view showed the tunnel opening into the RV (Figures 1C and 1D). Computed tomographic angiography (CT angio) revealed that the tunnel was arising above the right coronary sinus with both coronary arteries arising from a single left coronary ostium (Figure 2A). The tunnel was draining into the right ventricular infundibulum. (Figure 2B). The origin of the tunnel measured 8.5 mm and the distal RV end measured 6 mm.
Procedure
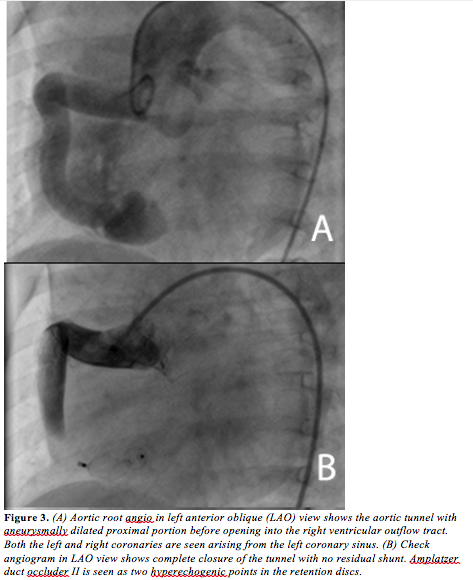 Cardiac catheterization was performed to confirm the diagnosis and to attempt transcatheter closure of the tunnel. Hemodynamic data showed Qp:Qs to be 3:1, with pulmonary artery pressures of 33/17 mm Hg (mean, 22 mm Hg). Aortic pressure was 100/20 mm Hg (mean, 47 mm Hg). Ascending aortogram done in left anterior oblique (LAO) view showed a dilated tortuous tract arising from the right side of the aortic root and draining into the right ventricular outflow tract (RVOT) with an aneurysmally dilated proximal portion (measuring 12 mm) with a narrow opening measuring 6 mm at the RV end (Figure 3A). A Terumo 0.018˝ wire was advanced into the fistulous tract from the aortic end through 4 Fr Cobra catheter into the RV and then into the pulmonary artery. A 4 Fr Cobra catheter was advanced over the wire. The tip of the wire was snared using a 15 mm Goose-neck snare advanced into the left pulmonary artery through the right femoral vein. The standard arteriovenous (AV) loop was made. Over this wire, a 7 Fr Cook shuttle delivery sheath was advanced into the fistula from the RV end with great difficulty. A futile attempt was made to introduce a 10 x 8 Amplatzer duct occluder (ADO). The check angiogram showed that the device was not in the tunnel. As there was an acute bend at the RV end of the tunnel, the large delivery sheath with the bulky ADO was not entering the tunnel. Hence, we decided to close the tunnel with the ADO II, which can be introduced from the aortic end without an AV loop as it has low profile.
Cardiac catheterization was performed to confirm the diagnosis and to attempt transcatheter closure of the tunnel. Hemodynamic data showed Qp:Qs to be 3:1, with pulmonary artery pressures of 33/17 mm Hg (mean, 22 mm Hg). Aortic pressure was 100/20 mm Hg (mean, 47 mm Hg). Ascending aortogram done in left anterior oblique (LAO) view showed a dilated tortuous tract arising from the right side of the aortic root and draining into the right ventricular outflow tract (RVOT) with an aneurysmally dilated proximal portion (measuring 12 mm) with a narrow opening measuring 6 mm at the RV end (Figure 3A). A Terumo 0.018˝ wire was advanced into the fistulous tract from the aortic end through 4 Fr Cobra catheter into the RV and then into the pulmonary artery. A 4 Fr Cobra catheter was advanced over the wire. The tip of the wire was snared using a 15 mm Goose-neck snare advanced into the left pulmonary artery through the right femoral vein. The standard arteriovenous (AV) loop was made. Over this wire, a 7 Fr Cook shuttle delivery sheath was advanced into the fistula from the RV end with great difficulty. A futile attempt was made to introduce a 10 x 8 Amplatzer duct occluder (ADO). The check angiogram showed that the device was not in the tunnel. As there was an acute bend at the RV end of the tunnel, the large delivery sheath with the bulky ADO was not entering the tunnel. Hence, we decided to close the tunnel with the ADO II, which can be introduced from the aortic end without an AV loop as it has low profile.
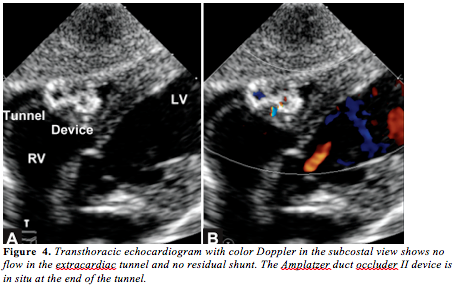 The tunnel was recrossed from the aortic end with a 0.018˝ Terumo wire; over that, a 5 Fr Terumo catheter was introduced into the pulmonary artery and then exchanged with a 0.035˝ J-tip regular wire. A 5 Fr Cook shuttle sheath was advanced over the wire. A 6 x 6 ADO II device was loaded and advanced easily into the delivery sheath. The distal disc of the device was released in the pulmonary artery and the whole system was pulled to the opening of the tunnel in the RVOT. The position of the distal retention disc was checked both by TTE and angiography. Then, the rest of the device was deployed in the aneurysmally dilated portion of the tunnel. The device was released after the check angiogram showed good position of the device with no residual shunt (Figure 3B). After the procedure, on clinical examination, pulse was 100/min with normal volume, blood pressure was 100/80 mm Hg, and no murmur was heard on auscultation. The TTE with color Doppler in the subcostal view showed the device in situ with no residual shunt (Figure 4). The infant had an uneventful postprocedure stay in the hospital and is normal on follow-up after 9 months. The ECG remained normal.
The tunnel was recrossed from the aortic end with a 0.018˝ Terumo wire; over that, a 5 Fr Terumo catheter was introduced into the pulmonary artery and then exchanged with a 0.035˝ J-tip regular wire. A 5 Fr Cook shuttle sheath was advanced over the wire. A 6 x 6 ADO II device was loaded and advanced easily into the delivery sheath. The distal disc of the device was released in the pulmonary artery and the whole system was pulled to the opening of the tunnel in the RVOT. The position of the distal retention disc was checked both by TTE and angiography. Then, the rest of the device was deployed in the aneurysmally dilated portion of the tunnel. The device was released after the check angiogram showed good position of the device with no residual shunt (Figure 3B). After the procedure, on clinical examination, pulse was 100/min with normal volume, blood pressure was 100/80 mm Hg, and no murmur was heard on auscultation. The TTE with color Doppler in the subcostal view showed the device in situ with no residual shunt (Figure 4). The infant had an uneventful postprocedure stay in the hospital and is normal on follow-up after 9 months. The ECG remained normal.
Discussion
The ARVT is an extremely rare, congenital malformation that connects the ascending aorta at or above the sinotubular junction to the cavity of the RV.10 Only 16 cases have been reported in the English literature.1-16 The aorto-ventricular tunnel differs from a ruptured sinus of Valsalva aneurysm in having its vascular orifice in the tubular aorta, rather than in a sinus of the aortic valve and in passing outside the heart into the tissue plane between the muscular subpulmonary infundibulum and the aortic valvar sinuses.17 The abnormal origin or absence of the right or left coronary ostium has been reported.1,2,4,6 It is important to delineate the coronary artery anatomy, as failure to do so in cases of an aberrant origin of a coronary artery may prevent successful correction or can change the therapeutic approach.4
Similar to our case, there is a report of ARVT in a 5-year-old girl in whom the entire coronary system was visualized from a single ostium located at the left sinus.13 In our case, the single left coronary ostium giving rise to the left main coronary artery and its branches and the right coronary artery was demonstrated by TTE, CT angio, and also by angiography. This made device closure from the aortic end feasible and very easy.
Though the surgical closure of the tunnel is the mainstay of treatment for this anomaly, it has a high surgical mortality. Traditionally, non-surgical closure is not considered a feasible option owing to the proximity of the tunnel to the coronary ostium or aortic valve leaflets and any associated coronary anomaly necessitating surgery.13 One case of a successful device closure of the ARVT has been reported with regular duct occluder.13 We had earlier experience with closing an ALVT18 with a large 16 x 14 ADO in a 4-year-old boy; however, in this infant, it was difficult to deploy the ADO due to the acute bend of the tunnel at the narrow RV end. Hence, we chose to close it with the ADO II.
The ADO II is made up of nitinol, a shape memory alloy of nickel and titanium. Each occluder is made up of a multilayered, flexible, nitinol wire mesh shaped into a cylindrical waist with retention discs on either end to secure it in position. Fabric-free technology (no polyester fabric), which allows for low-profile devices and delivery systems, creates superior deliverability and expanded procedural options. The advantage of the ADO II is that it has a very low profile and can be easily delivered through a 4 or 5 Fr sheath in infants. Since it has a retention disc on either side, it can be delivered from either end, which is especially useful in infants, and easy to track through tortuous tunnel with an acute bend as in our case. Since the narrow RV end measured 6 mm, we chose a 6 x 6 ADO II, so the mid-portion of the device snuggly fit the RV end and the 12 mm retention disc was perfect for the 12 mm aneurysmally dilated portion of the tunnel. Although the anatomy of the tunnel was not suitable for transcatheter closure from the venous end with a regular duct occluder, which is bulky, we accomplished successful device closure from the aortic end with the low-profile ADO II. To the best of our knowledge, this is the first and only case report of ARVT with biventricular apical non-compaction to be successfully closed using the new ADO II device in an infant.
Conclusion
Transcatheter closure of ARVT with ADO II from the aortic end is feasible, easy, and successful. This case highlights that the anatomy of the tunnel and the coronary anatomy are important for a successful outcome of transcatheter closure.
Acknowledgment. We thank Dr. Madhav Hegde, MD, Consultant Cardiothoracic Radiologist, Bengaluru for sharing the CT angiogram images.
References
- Bharati S, Lev M, Cassels DE. Aortico-right ventricular tunnel. Chest. 1973;63(2):198-202.
- Saylam A, Tuncali T, Ikizler C, Aytac A. Aorto-right ventricular tunnel. A new concept in congenital cardiac malformations. Ann Thorac Surg. 1974;18(6):634-637.
- Jureidini SB, de Mello D, Nouri S, Kanter K. Aortico-right ventricular tunnel with critical pulmonary stenosis: diagnosis by two dimensional and Doppler echocardiography and angiography. Pediatr Cardiol. 1989;10(2):99-103.
- Kleinkamp G, Minami K, Thies WR, et al. Aorta-right ventricular tunnel with a rudimentary valve and ananomalous origin of the left coronary artery. J Thorac Cardiovasc Surg. 1992;104(6):1759-1760.
- Westaby S, Archer N. Aortico-right ventricular tunnel. Ann Thorac Surg. 1992;53(6):1107-1109.
- Rosengart TK, Redel DA, Stark JF. Surgical repair of aorto-right ventricular tunnel in an infant. Ann Thorac Surg. 1993;55(2):520-522.
- Van Son JA, Hambsch J, Schneider P, Mohr FW. Repair of aortic right ventricular tunnel. Eur J Cardiothorac Surg. 1998;14(2):214-217.
- Vargas FJ, Molina A, Martinez JC, Ranzini ME, Vazquez JC. Aortico-right ventricular tunnel. Ann Thorac Surg. 1998;66(5):1793-1795.
- Talwar S, Choudhary UK, Kothari SS, Airan B. Aortico-right ventricular tunnel. Int J Cardiol. 1999;70(2):201-205.
- Hruda J, Hazekamp MG, Sobotka-Plojhar MA, Ottenkamp J. Repair of aorto-right ventricular tunnel with pulmonary stenosis and an anomalous origin of left coronary artery. Eur J Cardiothorac Surg. 2002;21(6):1123-1125.
- Freund MW, Stoutenbeek P, Van der Laan M, et al. Aortico right ventricular tunnel. Prenatal diagnosis leading to neonatal survival. Fetal Diagn Ther. 2007;22(5):335-338.
- Sheikh N. Repair of aorto-right ventricular tunnel: a case report. Cardiovasc J. 2010;3:398-100.
- Poptani VA, Thakkar BM, Patel NH. Transcatheter closure of a rare case of aorto-right ventricular tunnel with single coronary artery. J Invasive Cardiol. 2010;22(12):611-614.
- Lin BS, Zhang XH, Jiang YZ, Zhang BM, Gao D, Song J. Diagnosis and surgical treatment of adult aortico right ventricular tunnel. Ann Thorac Surg. 2010;89(6):2024-2026.
- Talwar S, Nair VV, Kothari SS, Gulati GS, Choudhary SK, Airan B. Aortico-right ventricular tunnel with anomalous right coronary artery. J Card Surg. 2011;26(5):521-526.
- Singh SK, Dwivedi SK, Kumar A, et al. Aneurysmal aorto-right ventricular tunnel. Ann Thorac Surg. 2012;93(2):e21-e22.
- McKay R. Aorto-ventricular tunnel. Orphanet J Rare Dis. 2007;2:41.
- Vijayalakshmi IB, Chitra N, Prabhu Deva AN. Use of an Amplatzer duct occluder for closing an aortico-left ventricular tunnel in a case of noncompaction of the left ventricle. Pediatr Cardiol. 2004;25(1):77-79.
__________________________________________
From the Sri Jayadeva Institute of Cardiovascular Sciences and Research, Bengaluru-560069, Karnataka, India.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted September 12, 2012 and accepted September 21, 2012.
Address for correspondence: Dr. I. B. Vijayalakshmi , MD, DM (Card), FICC, FIAMS, FIAE, FICP, FCSI, FAMS, DSc, Professor of Paediatric Cardiology, ‘Aditi’ 44 A, V Main road, Vijayanagar II stage, Bengaluru-560040, Karnataka, India. Email: docvj@yahoo.com













