

Comparison of Six-Year Clinical Outcome of Sirolimus- and Paclitaxel-Eluting Stents to Bare-Metal Stents in Patients with ST-Segment Elevation Myocardial Infarction: An Analysis of the RESEARCH and T-SEARCH Registries
Abstract: Background. Short- and long-term data showed that drug-eluting stents (DES) significantly decreased target vessel revascularization (TVR) and major adverse cardiac event (MACE) rates compared to bare-metal stents (BMS). However, conflicting long-term data remain for patients with ST-segment elevation myocardial infarction (STEMI). Objective. Our aim was to assess the 6-year clinical outcome of all patients undergoing primary percutaneous coronary intervention (PPCI) for a de novo lesion with exclusive use of BMS, sirolimus-eluting stents (SES) and paclitaxel-eluting stents (PES). Methods. Three PPCI cohorts (BMS = 80; SES = 92; PES = 162) were systematically followed for the occurrence of MACE. Results. Very late stent thrombosis was more common after the implantation of SES as compared to PES or BMS (7.6%, 0.6%, and 0.0%, respectively; p = 0.001). Kaplan-Meier estimates indicate no statistically significant difference for mortality between the three stent types at 6 years (BMS = 25%; SES = 15%; PES = 21%; Log-rank p = 0.2). After adjustment for differences in baseline characteristics, mortality, mortality/myocardial infarction (MI), and MACE rates were significantly lower for SES compared to BMS, but not for PES (aHR = 0.41, 95% CI: 0.17–0.98; aHR = 0.44, 95% CI: 0.21–0.96; aHR = 0.35, 95% CI: 0.17–0.72, respectively). No differences were observed between the three stent types for TVR rates. Conclusion. Neither SES nor PES improved safety or efficacy as compared to BMS in a STEMI population at 6 years. After adjusting, the usage of SES resulted in a significant decrease in mortality, mortality/MI and MACE rates as compared to BMS, in contrast to the usage of PES. SES and PES have a similar effectiveness and safety profile, although very late stent thrombosis was more common with SES.
J INVASIVE CARDIOL 2011;23:336–341
Key words: percutaneous coronary intervention, ST-segment elevation myocardial infarction, stents
_____________________________________
The urgent restoration of blood flow to the culprit coronary artery is vital after a sudden thrombotic obstruction causes a myocardial infarction with ST-segment elevations on the electrocardiogram. The duration and location of the coronary obstruction and the existence of collateral vessels to the affected myocardial region are the main factors affecting the size of myocardial necrosis and eventually the prognosis of these patients.
Although the implantation of drug-eluting stents (DES) effectively reduces restenosis rates in various subsets of patient groups including “real-world” patients compared to bare-metal stents (BMS), there still remains considerable uncertainty for the implantation of DES in a primary percutaneous coronary intervention (PPCI) setting due to contrary findings on efficacy and safety endpoints.1–5 In particular, the potential of more very late stent thrombosis after DES implantation, which could be even more pronounced in this high-risk patient population with vulnerable coronary artery disease (CAD), caused a serious dilemma.6–11
A recent meta-analysis, consisting of 13 randomized trials, showed that ST-segment elevation myocardial infarction (STEMI) patients treated with a DES had fewer target vessel revascularization (TVR) procedures as compared with those treated with a BMS in the first year post-PCI without any significant differences in cardiac mortality and stent thrombosis rates.12 In contrast, our 3- and 4-year follow-up data of relatively small consecutive patient cohorts suggested that neither sirolimus-eluting stents (SES) nor paclitaxel-eluting stents (PES) were superior to BMS in terms of decreasing mortality, TVR and major adverse cardiac event (MACE) rates in PPCI patients.13,14 As a consequence of the paucity of long-term data combined with concerns of the increased occurrence of stent thrombosis later than 1 year after DES implantation, we evaluated the 6-year clinical outcomes of STEMI patients treated with BMS and DES in our academic center.
Methods
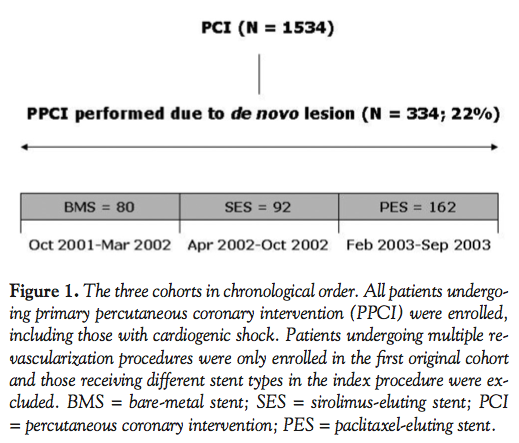 Patient population and study design. A total of 334 consecutive STEMI patients were treated with PPCI for de novo lesions in three “real world” registries in our academic hospital between October 2001 and September 2003 (Figure 1). Patients with a rescue PCI after failed thrombolysis, prior brachytherapy or receiving multiple stent types during the initial procedure were excluded from analysis. All other patients, including those with cardiogenic shock, remained in their first original enrolled cohort during the follow-up period.
Patient population and study design. A total of 334 consecutive STEMI patients were treated with PPCI for de novo lesions in three “real world” registries in our academic hospital between October 2001 and September 2003 (Figure 1). Patients with a rescue PCI after failed thrombolysis, prior brachytherapy or receiving multiple stent types during the initial procedure were excluded from analysis. All other patients, including those with cardiogenic shock, remained in their first original enrolled cohort during the follow-up period.
The Rapamycin-Eluting Stent Evaluated at Rotterdam Cardiology Hospital (RESEARCH) registry was conducted from April 2002 until October 2002 and included 92 consecutive STEMI patients who were treated with only SES (Cypher®, Cordis Corporation, Miami Lakes, Florida). From February 2003 until September 2003, 162 consecutive STEMI patients were treated with the PES (TAXUS™, Express2™ or Liberté™, Boston Scientific, Natick, Massachusetts) as the default strategy for all PCI as part of the Taxus Stent Evaluated at Rotterdam Cardiology Hospital (T-SEARCH) registry. These patients were compared with 80 BMS patients who were treated from October 2001 until March 2002.
 All procedures were performed according to standard clinical guidelines and every patient was pre-treated with aspirin and ≥ 300 mg clopidogrel. The post-procedural dual-antiplatelet regimen consisted of ≥ 80 mg aspirin lifelong and ≥ 75 mg clopidogrel for at least 1 month if BMS were used, ≥ 3 months for patients with SES and ≥ 6 months for patients with PES. Periprocedural glycoprotein IIb/IIIa antagonists were used at the discretion of the treating interventional cardiologist. All of the repeat coronary angiographies were clinically driven by physical symptoms or diagnostic findings suggestive of myocardial ischemia.
All procedures were performed according to standard clinical guidelines and every patient was pre-treated with aspirin and ≥ 300 mg clopidogrel. The post-procedural dual-antiplatelet regimen consisted of ≥ 80 mg aspirin lifelong and ≥ 75 mg clopidogrel for at least 1 month if BMS were used, ≥ 3 months for patients with SES and ≥ 6 months for patients with PES. Periprocedural glycoprotein IIb/IIIa antagonists were used at the discretion of the treating interventional cardiologist. All of the repeat coronary angiographies were clinically driven by physical symptoms or diagnostic findings suggestive of myocardial ischemia.
Definitions and clinical endpoints. Definite stent thrombosis was defined as an angiographically documented thrombus in or within 5 mm of the stent, accompanied by at least one of the following criteria as recommended by the academic research consortium (ARC) criteria: 1) acute symptoms; 2) ischemic electrocardiographic changes; and 3) typical rise and fall of cardiac markers and categorized into early (within 30 days post-stent implantation), late (within 30 days and 1 year post-stent implantation) and very late (> 1 year post-stent implantation). The primary endpoint was the occurrence of MACE [defined as a composite of all-cause mortality, myocardial infarction (MI) and TVR]. Secondary efficacy endpoint included TVR, while safety endpoints consisted of all-cause mortality and the composite of all-cause mortality/MI. MI was diagnosed by recurrent typical clinical symptoms, the development of ST-segment elevation or left bundle branch block on electrocardiography with a CK-MB rise of 3 times the upper limit of normal and/or positive troponin levels in the laboratory values. TVR was defined as a repeat PCI in the same vessel as the index procedure, in the presence of ischemic symptoms or positive functional ischemia study on the target vessel area and a significant minimal luminal diameter stenosis of at least 50%.
 Follow-up. The clinical status of treated PPCI patients was documented yearly by contacting municipal civil registries until December 2009. All living patients received a health-related questionnaire, consisting of queries regarding rehospitalization and cardiac events. The hospital records and coronary angiographies from our academic hospital or the referring institution were systematically reviewed in case of a patient-reported event.
Follow-up. The clinical status of treated PPCI patients was documented yearly by contacting municipal civil registries until December 2009. All living patients received a health-related questionnaire, consisting of queries regarding rehospitalization and cardiac events. The hospital records and coronary angiographies from our academic hospital or the referring institution were systematically reviewed in case of a patient-reported event.
Statistical analysis. Categorical baseline variables were tested with the Chi-square test and the ANOVA test was used for continuous baseline variables between the groups. The Kaplan-Meier method estimated the cumulative adverse cardiac events for the endpoints (all-cause mortality, all-cause mortality/MI, MACE and TVR) and the differences between the three stent curves were tested with the log-rank test.
Multivariate Cox proportional hazard regression model [95% confidence interval (CI) and p-value < 0.05 regarded as significant] was used to adjust for differences in baseline and procedural characteristics between the groups. All baseline variables with a p ≤ 0.5 in univariable analysis were used in the multivariate Cox proportional hazard regression model. Stepwise backward deletion of the least significant variable was performed until all variables had a p ≤ 0.10.
Patients lost to follow-up were considered at risk until the date of last contact, at which point they were censored. All statistical analyses were performed with SPSS for Windows version 17 (SPSS Inc., Chicago, Illinois).
Results
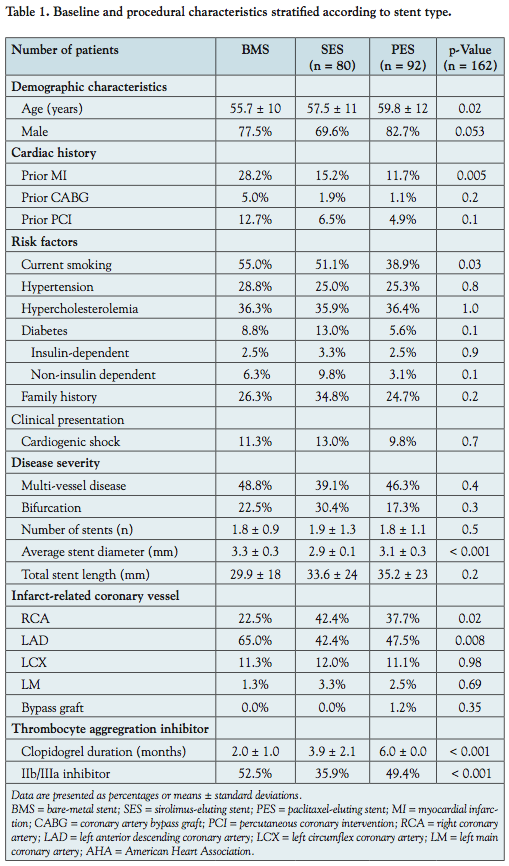 Population characteristics. Complete follow-up was available for 92.5% of patients. The clinical baseline and procedural characteristics of the three cohorts are shown in Table 1. Most of these characteristics were comparable between the three groups, except BMS patients were younger (p = 0.02), more often had a history of prior MI (p = 0.005) and were more likely to smoke cigarettes (p = 0.03) compared to SES and PES patients. The right coronary artery was more often the culprit (p = 0.02) and the diameter of the implanted stents was also larger in the BMS cohort (p < 0.001). Glycoprotein IIb/IIIa was more commonly prescribed to patients receiving BMS, and the clopidogrel intake was longer in both DES cohorts as mandated by the study protocol. The duration of clopidogrel usage post-stent implantation increased over time, being shortest for the BMS group (mean of 1 month) and the longest in the PES population (mean of 6 months).
Population characteristics. Complete follow-up was available for 92.5% of patients. The clinical baseline and procedural characteristics of the three cohorts are shown in Table 1. Most of these characteristics were comparable between the three groups, except BMS patients were younger (p = 0.02), more often had a history of prior MI (p = 0.005) and were more likely to smoke cigarettes (p = 0.03) compared to SES and PES patients. The right coronary artery was more often the culprit (p = 0.02) and the diameter of the implanted stents was also larger in the BMS cohort (p < 0.001). Glycoprotein IIb/IIIa was more commonly prescribed to patients receiving BMS, and the clopidogrel intake was longer in both DES cohorts as mandated by the study protocol. The duration of clopidogrel usage post-stent implantation increased over time, being shortest for the BMS group (mean of 1 month) and the longest in the PES population (mean of 6 months).
6-year clinical outcome. Thirty-day, 1-year and 3-year clinical outcome have been reported previously.15–17 The cumulative incidence and the associated adjusted hazard ratios (HR) (BMS versus SES, BMS versus PES, SES versus PES) of the 6-year follow-up of the STEMI-patients from the BMS cohort, RESEARCH and T-SEARCH are shown in Table 2 for each of the endpoints.
At 6 years, 21 (Kaplan-Meier estimate of 25%) of the BMS patients had died, compared to 14 (15%) of SES patients and 32 (21%) of PES patients, which was non-significant in univariate analysis. No significant differences were found for MACE and TVR rates between SES and PES (HR = 1.12, 95% CI: 0.86–1.44; HR = 0.99; 95% CI: 0.64–1.54, respectively). None of the endpoints were significantly different between the three stent types. Furthermore, MACE (HR = 0.77, 95% CI: 0.49–1.20), TVR (HR = 0.98, 95% CI: 0.42–2.31), mortality (HR = 0.72, 95% CI: 0.43–1.21) and mortality/MI (HR = 0.81, 95% CI: 0.50–1.32) rates did not decrease after bundling SES and PES into the broader DES group (n = 254 patients) compared to the BMS group.
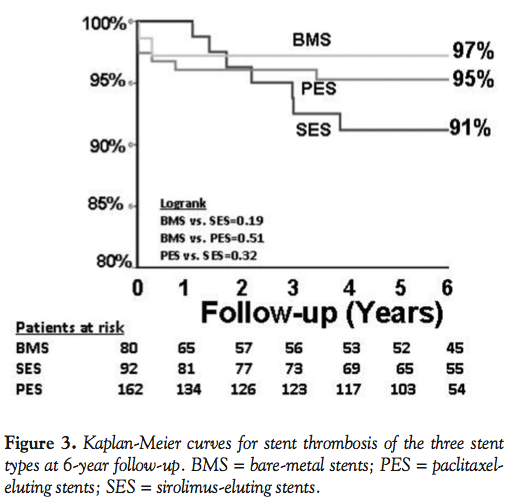
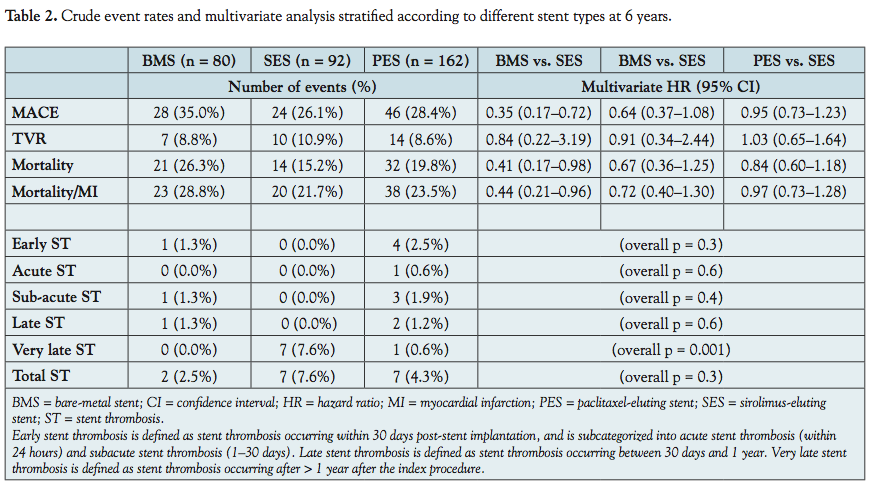 The multivariate Cox regression analysis, which was used to correct for baseline differences and independent predictors of adverse events at 6 years, showed that all-cause mortality rates were lower in the SES group compared to the BMS group (aHR = 0.41, 95% CI: 0.17–0.98). Also, the all-cause mortality/MI and MACE rates were lower in the SES group. However, very late stent thrombosis was more common in SES patients compared to those receiving a PES or BMS (7.6% versus 0.6% versus 0%, respectively; p = 0.001) (Table 2). No significant differences were found on all endpoints between PES patients and BMS patients. The TVR rates of the three stent types were similar.
The multivariate Cox regression analysis, which was used to correct for baseline differences and independent predictors of adverse events at 6 years, showed that all-cause mortality rates were lower in the SES group compared to the BMS group (aHR = 0.41, 95% CI: 0.17–0.98). Also, the all-cause mortality/MI and MACE rates were lower in the SES group. However, very late stent thrombosis was more common in SES patients compared to those receiving a PES or BMS (7.6% versus 0.6% versus 0%, respectively; p = 0.001) (Table 2). No significant differences were found on all endpoints between PES patients and BMS patients. The TVR rates of the three stent types were similar.
Discussion
This is the longest follow-up study comparing the safety and effectiveness of DES with BMS in a STEMI population in the real world. The usage of SES was still associated with a higher rate of very late stent thrombosis compared to PES and BMS at 6 years; however, no events were noted beyond 4 years of follow-up in the three cohorts. Noteworthy is the fact that the duration of clopidogrel use after DES implantation increased from 1 month to 1 year, which potentially effected the occurrence of late stent thrombosis of SES patients in our cohort.
After adjusting for differences in baseline and procedural characteristics, the rate of MACE was significantly lower in the SES patients when compared to BMS patients, driven primarily by a lower mortality rate at 6 years. No difference was observed in terms of TVR between the three stent types.
The benefits of DES over BMS use observed in patients with stable coronary artery disease population at 4 years were accrued in the first year after treatment.18 After this period, there was no incremental benefit in terms of clinical events such that the early advantage was maintained in the long-term without significant catch-up. However, the incidence of very late stent thrombosis was higher in the DES groups. In the STEMI population, the use of DES is still controversial due to safety concerns, especially with the incidence of stent malapposition, delayed healing and subsequent stent thrombosis. The recent HORIZONS-AMI study has alleviated the concerns to some extent by demonstrating similar safety endpoints at 12 months in terms of death and stent thrombosis for both PES and BMS (3.5% and 3.5%, respectively; p = 0.98) and stent thrombosis (3.2% and 3.4%, respectively; p = 0.77).19 This randomized trial with 3,006 patients presenting with STEMI confirmed earlier reports of superior efficacy with the DES. In fact, PES-treated patients had significantly lower 12-month rates of ischemia-driven target lesion revascularization (4.5% versus 7.5%; HR = 0.59; 95% CI: 0.43–0.83; p = 0.002). The 2-year outcomes of PES (n = 90) or SES (n = 90) versus BMS (n = 90) in the PASEO trial demonstrated retained benefit of DES in terms of TVR in a STEMI population.20 As with stable coronary artery disease, the advantage of DES over BMS had been accrued in the first year of follow-up already. On the other hand, in the MISSION! Intervention trial, the significant difference between SES (n = 158) and BMS (n = 152) patients for TVR at 1-year follow-up was no longer statistically significant at 3 years (TVR, 8.9% versus 15.8%; p = 0.06).21 Moreover, as observed in our current report, very late stent thrombosis was observed in the SES group as opposed to none in the BMS group, which may explain the catch-up in TVR rates seen on longer-term follow-up.
Thus, although the occurrence of stent thrombosis in our cohorts remained relatively low and non-different for both BMS and PES, a higher very late stent thrombosis rate in SES remains a realistic concern, and whether this is more common in patients treated for STEMI as compared to stable coronary artery disease remains to be demonstrated.
Similarly, the 3-year follow-up data of the SESAMI trial, which compared outcomes of 320 STEMI patients treated with BMS and SES, showed that the advantage of the latter in terms of target lesion revascularization (13.5% versus 7%; p = 0.048) was mainly accrued during the first year of follow-up, which coincided with the discontinuation of clopidogrel.22 In the present study at 6 years, as well as in our previous report at 4 years, we did not observe differences in the rates of TVR between DES and BMS. Although shorter-term follow-up of similar comparative studies in the STEMI population has found differences in this endpoint at 1 year, our findings may reflect a failure of sustained DES superiority in the longer term. However, the lack of statistical difference was also reported in the pROSIT trial, which compared SES to PES in PPCI patients.23 This trial showed comparable clinical outcomes of both stents at 1 year.23 The study, which included 6-month angiographic follow-up, failed to show statistical superiority of SES despite lower late loss and numerically higher rates of binary stenosis. However, both this and our study results have to be considered with caution. First, the DES group in our RESEARCH and T-SEARCH registries had longer stented segments, as opposed to longer stents in the BMS group in more contemporary randomized trials.24 Second, the study is underpowered to definitely conclude equality in safety and efficacy of these stents in MI. Interestingly, SES-treated patients showed a survival advantage in our cohort. Although no major trial suggested a lower mortality rate with DES when compared with BMS, an observational study by Mauri et al reported a lower risk-adjusted mortality rate for patients treated with DES for MI (10.7% versus 12.8%; p = 0.02).25 The superiority of SES over BMS in our cohort was attributed to a lower mortality in the DES group, whereas TVR was not different. Restenosis has been shown to be associated with increased risk of death and MI.26 Since our patients are real-world registry patients with no regular angiographic follow-up, in the long term, mortality may be one of the manifestations of undetected/inadequately treated myocardial ischemia secondary to subclinical restenosis.
The current analysis has some limitations worthy of note. First, it is observational in nature and differences in baseline clinical variables and adjunctive treatment during the specific time periods may have resulted in revascularization and/or mortality rate advantage. Although statistical adjustment for confounders was performed, this may still have been inadequate, especially given the small number of patients in the three stent groups. Second, some events could have been missed due to the fact that only living patients are asked to self-report events.
In conclusion, very late stent thrombosis is still an issue of concern at 6-year follow-up for first-generation SES. This did not jeopardize the survival advantage or rate of MACE in the SES group when compared to BMS. No differences were found in the TVR rates between the three stent types. These findings need to be addressed in the long-term follow-up of the randomized trials.
References
- Spaulding C, Henry P, Teiger E, et al., for the TYPHOON investigators. Sirolimus-eluting versus uncoated stents in acute myocardial infarction. N Engl J Med 2006;355:1093–1104.
- Laarman GJ, Suttory MJ, Dirksen MT, et al. Paclitaxel-eluting versus uncoated stents in primary percutaneous coronary intervention. N Engl J Med 2006;355:1105–1113.
- Kukreja N, Onuma Y, Garcia-Garcia H, et al. Primary percutaneous coronary intervention for acute myocardial infarction: Long-term outcome after bare-metal and drug-eluting stent implantation. Circ Cardiovasc Interv 2008;1:103–110.
- Daemen J, Kukreja N, van Twisk PH, et al. Four-year clinical follow-up of the rapamycin-eluting stent evaluated at Rotterdam Cardiology Hospital registry. Am J Cardiol 2008;101:1105–1111.
- Daemen J, Tsuchida K, Stefanini GG, et al. Two-year clinical follow-up of the unrestricted use of the paclitaxel-eluting stent compared to the sirolimus-eluting stent as part of the Taxus-Stent Evaluated at Rotterdam Cardiology Hospital (T-SEARCH) registry. EuroIntervention 2006;2:330–337.
- McFadden EP, Stabile E, Regar E, et al. Late thrombosis in drug-eluting coronary stents after discontinuation of antiplatelet therapy. Lancet 2004;364:1519–1521.
- Iakovou I, Schmidt T, Bonizzoni E, et al. Incidence, predictors, and outcome of thrombosis after successful implantation of drug-eluting stents. JAMA 2005;293:2126–2130.
- Lagerqvist B, James SK, Stenestrand U, et al., for the SCAAR Study Group. Long-term outcomes with drug-eluting stents versus bare-metal stents in Sweden. N Engl J Med 2007;356:1009–1019.
- Kernis SJ, Cohen D, Rein K. Clinical outcome associated with use of drug-eluting stents compared with bare-metal stent for primary percutaneous intervention. Am J Cardiol 2005;96(Suppl 7A):47H.
- Spertus JA, Kettelkamp R, Vance C, et al. Prevalence, predictors, and outcomes of premature discontinuation of thienopyridine therapy after drug-eluting stent placement results from the PREMIER registry. Circulation 2006;113:2803–2809.
- Daemen J, Wenaweser P, Tsuchida K, et al. Early and late coronary stent thrombosis of sirolimus-eluting and paclitaxel-eluting stents in routine clinical practice: Data from a large two-institutional cohort study. Lancet 2007;369:667–678.
- Piscione F, Piccolo R, Cassese S, et al. Effect of drug-eluting stents in patients with acute ST-segment elevation myocardial infarction undergoing percutaneous coronary intervention: A meta-analysis of randomized trials and an adjusted indirect comparison. EuroIntervention 2010;5:853–860.
- Daemen J, Tanimoto S, Garcia-Garcia HM, et al. Comparison of three-year clinical outcome of sirolimus- and paclitaxel-eluting stents versus bare-metal stents in patients with ST-segment elevation myocardial infarction (from the RESEARCH and T-SEARCH Registries). Am J Cardiol 2007;99:1027–1032.
- Kukreja N, Onuma Y, Garcia-Garcia H, et al. Primary percutaneous coronary intervention for acute myocardial infarction. Long-term outcome after bare-metal and drug-eluting stent implantation. Circ Cardiovasc Interv 2008;1:103–110.
- Lemos PA, Saia F, Hofma SH, et al. Short- and long-term clinical benefit of sirolimus-eluting stents compared to conventional bare stents for patients with acute myocardial infarction. J Am Coll Cardiol 2004;43:704–708
- Hofma SH, Ong AT, Aoki J, et al. One-year clinical follow-up of paclitaxel-eluting stents for acute myocardial infarction compared with sirolimus-eluting stents. Heart 2005;91:1176–1180.
- Daemen J, Tanimoto S, Garcia-Garcia HM, et al. Comparison of three-year clinical outcome of sirolimus- and paclitaxel-eluting stents versus bare-metal stents in patients with ST-segment elevation myocardial infarction (from the RESEARCH and T-SEARCH Registries). Am J Cardiol 2007;99:1027–1032.
- Simsek C, Onuma Y, Magro M, et al. Interventional Cardiologists of the Thoraxcenter (2000–2005). Four-year clinical outcome of sirolimus- and paclitaxel-eluting stents compared to bare-metal stents for the percutaneous treatment of stable coronary artery disease. Catheter Cardiovasc Interv 2010;76:41–49.
- Wohrle J, Desaga M, Metzger C, et al. Impact of transfer for primary percutaneous coronary intervention on survival and clinical outcomes (from the HORIZONS-AMI trial). Am J Cardiol 2010;106:1218–1224.
- Di Lorenzo E, De Luca G, Sauro R, et al. The PASEO (paclitaxel- or sirolimus-eluting stent versus bare-metal stent in primary angioplasty) randomized trial. J Am Coll Cardiol Interv 2009;2:515–523.
- Atary JZ, van der Hoeven BL, Liem SS, et al. Three-year outcome of sirolimus-eluting versus bare-metal stents for the treatment of ST-segment elevation myocardial infarction (from the MISSION! Intervention Study). Am J Cardiol 2010;106:4–12.
- Violini R, Musto C, De Felice F, et al. Maintenance of long-term clinical benefit with sirolimus-eluting stents in patients with ST-segment elevation myocardial infarction 3-year results of the SESAMI (sirolimus-eluting stent versus bare-metal stent in acute myocardial infarction) trial. J Am Coll Cardiol 2010;55:810–814.
- Lee JH, Kim HS, Lee SW, et al. Prospective randomized comparison of sirolimus- versus paclitaxel-eluting stents for the treatment of acute ST-elevation myocardial infarction: pROSIT trial. Catheter Cardiovasc Interv 2008;72:25–32.
- Kukreja N, Onuma Y, Garcia-Garcia HM, et al. Primary percutaneous coronary intervention for acute myocardial infarction: Long-term outcome after bare-metal and drug-eluting stent implantation. Circ Cardiovasc Interv 2008;1:103–110.
- Mauri L, Silbaugh TS, Garg P, et al. Drug-eluting or bare-metal stents for acute myocardial infarction. N Engl J Med 2008;359:1330–1342.
- Doyle B, Rihal CS, O’Sullivan CJ, et al. Outcomes of stent thrombosis and restenosis during extended follow-up of patients treated with bare-metal coronary stents. Circulation 2007;116:2391–2398.
_____________________________________
From the Thoraxcenter, Department of Cardiology, Erasmus Medical Center Rotterdam, the Netherlands.
The authors report no conflicts of interest regarding the content herein.
Manuscript submitted March 7, 2011, provisional acceptance given April 26, 2011, final version accepted May 16, 2011.
Address for correspondence: P.W.J.C. Serruys, MD, PhD, Department of Cardiology, Thoraxcenter, Room Ba 583, Erasmus Medical Center, Dr. Molewaterplein 40, 3015 RD, Rotterdam, the Netherlands. Email: p.w.j.c.serruys@erasmusmc.nl










