

Comparison of Transvenous Versus Transthoracic Catheter-Based Device Closure of Patent Ductus Arteriosus With Amplatzer Duct Occluder
Abstract: Objective. This study compared the clinical outcome of the transvenous versus transthoracic approach for closure of patent ductus arteriosus (PDA). Background. There are no data regarding the results of transvenous versus transthoracic catheter-based device closure of PDA with Amplatzer duct occluder (ADO) despite their increasing use as alternatives to conventional surgery. Methods. In this observational study, a total of 150 consecutive patients with PDA were allocated either to the transvenous approach (group A, n = 108) and the transthoracic approach (group B, n = 42) by using ADO between January 2010 and April 2012. Echocardiography was performed to evaluate the prespecified initial and 6-month success of PDA closure. The technical indices and procedure-related major acute and chronic complications were documented. Results. There were similar initial success rates (98.2% vs 100%; P>.05) and 6-month success rates (99.1% vs 100%; P>.05) between groups, and group A had fewer major acute complications (3.7% vs 85.7%; P<.001), shorter operating time (1.3 hours vs 2.1 hours; P<.001), Intensive Care Unit stay (0 hours vs 23.0 hours; P<.001), and recovery time (3.8 days vs 9.5 days; P<.001), and lower rates of general anesthesia (36.1% vs 100%; P<.001), blood transfusion (0.9% vs 71.4%; P<.001), and extra use of antibiotics (27.8% vs 78.6%; P<.001), and lower total cost of hospitalization ($3815.78 vs $5730.21; P<.001). Conclusions. Despite similar efficacy for duct closure with ADO, transvenous approach was associated with fewer acute complications, more periprocedural comfort, and lower cost; thus, transthoracic approach should not be a reasonable choice for duct closure except for particular indications.
J INVASIVE CARDIOL 2013;25(10):502-506
Key words: patent ductus arteriosus, transvenous, transthoracic
_____________________________
Patent ductus arteriosus (PDA) is one of the most common congenital heart defects (CHDs).1-3 The presence of volume overloading on the left atrium and the left ventricle is an indicator of closure in the defect. The risks of endocarditis, aneurysm of PDA, and pulmonary vascular disease are likewise indications for closure. Although conventional surgical closure of PDA is safe and effective,4 several inevitable pitfalls exist; these disadvantages include postoperative pain and procedure-related complications, as well as cosmetic and psychosomatic problems associated with the incision scar.5-7 Thus, numerous minimally invasive surgical techniques (eg, axillary vertical incision thoracotomy with duct ligation, video-assisted thoracoscopic duct clipping, and parasternal thoracotomy with catheter-based device duct)8-15 and transvenous catheter-based device closure16-24 have been introduced clinically. These alternative procedures have proven to be as effective as conventional surgery, with less invasion and postoperative discomfort, shorter hospital stay, and fewer or no cosmetic issues related to skin incision. However, available data on transvenous and transthoracic catheter-based device closure for the treatment of PDA are limited, despite their increased use as alternatives to conventional surgery.
Methods
Patient selection criteria. The inclusion criteria were: (1) patient age >6 months and weight >4 kg; (2) moderate-to-large isolated PDA (minimal duct diameter >2 mm, as measured pre-procedurally by echocardiography); and (3) patients who were experiencing persistent residual shunts after surgical intervention.
The exclusion criteria for PDA patients were: (1) any other cardiac comorbidity regardless of congenital conditions or acquired heart disease that necessitated surgical treatment; (2) significant cardiac and non-cardiac comorbidities that could have an effect on clinical outcome of duct closure; (3) right-to-left shunting caused by severe pulmonary hypertension; and (4) true window-type PDA.
Between January 2010 and April 2012, a total of 150 eligible patients were non-randomly treated using either the transvenous approach (group A, n = 108) or the transthoracic approach (group B, n = 42) for using the Amplatzer duct occluder (ADO; St Jude Medical), at the discretion of the patients (or their parents or guardians).
The study was approved by the Ethics Committee of Fujian Medical University. Its protocol conformed to the principles outlined in the Declaration of Helsinki. Signed informed consent was obtained from all participating patients (or from their parents or guardians).
Transvenous catheter-based device closure of patent ductus arteriosus. A simplified method for duct closure was previously reported by our group and used in the present study.25 Briefly, patients were placed under local or general anesthesia, and the femoral vein was punctured to create a device delivery track under brief fluoroscopy. The femoral artery puncture and aortic angiography for the conventional transcatheter duct closure could be neglected. Except for a brief fluoroscopy step, the entire procedure was guided by transthoracic echocardiography (TTE). The TTE method with two-dimensional echocardiography (2DE), color-coded Doppler flow imaging (CDFI), and continuous wave (CW) imaging modalities was used in the following steps: (1) the duct size, length, and anatomical characteristics were carefully evaluated to select the appropriate ADO; (2) the residual shunting and its corresponding changes were continuously monitored; (3) the recovery of the fixed configuration of the ADO was visualized; and (4) a selected occlude was evaluated to determine if it should be replaced (as a result of incorrect size or significant residual shunting) before its release. The accurate measurement of the minimal duct width (MDW) is the key step because a reference of 1.5× to 2.0× MDW (2.0× MDW for type B ductus; 1.5× MDW for other ductus types) was used when the ADO was selected for the first occluding attempt.
Transthoracic catheter-based device closure of patent ductus arteriosus. The minimally invasive technique of transthoracic peripulmonary duct closure was conducted via a parasternal approach under general anesthesia as previously described.26 A 2-3 cm parasternal incision was made in the left second intercostal space. The pericardium was incised, and a specially designed delivery sheath with the device was inserted into the pulmonary trunk through the purse-string sutures. Under the guidance of transesophageal echocardiography, the delivery sheath was advanced through the PDA into the descending aorta, and the device was subsequently deployed. For patients with a large PDA or significant pulmonary hypertension, a stay suture was passed through the device, which was tied down with purse-string sutures to prevent device dislocation after its release. Similar to simplified method for the transcatheter closure of PDA, TTE was used to measure the ductal size and morphology for the preprocedural selection of the proper ADO.
For both approaches, 100 mg of aspirin and periprocedural antibiotic prophylaxis were administered for 6 months, according to the hospital routine. Extra use of antibiotics depended on the clinical situations of patients.
Echocardiographic studies. The TTE method with imaging modalities of 2DE, CDFI, and CW was performed preprocedurally, periprocedurally, and postprocedurally using a commercially available echocardiographic system (Vivid-7; GE Medical Systems). Aside from the aforementioned periprocedural echocardiographic guidance, echocardiography was conducted to routinely assess the cardiac functional indices, including left atrial diameter (LAD), left ventricular end-diastolic volume (LVEDV), left ventricular end-systolic volume (LVESV), left ventricular ejection fraction (LVEF), and peak pulmonary artery systolic pressure (PASP). LVEDV, LVESV, and LVEF were measured using the modified Simpson’s method. PASP was calculated using the equation 4V2 + RAP when tricuspid regurgitation existed without right ventricular outflow and pulmonary stenosis. In this equation, V represents the CW-derived peak velocity of the tricuspid regurgitant jet. The right atrial systolic pressure was approximately 10 mm Hg, and pulmonary hypertension was defined as PASP ≥30 mm Hg.
Periprocedural evaluation and acute clinical outcomes. All patients underwent periprocedural clinical and echocardiographic evaluations during hospitalization. Periprocedural evaluation was intended to record: (1) technical indices including the initial success of PDA closure, general anesthesia, operating time, ICU stay, recovery time (from the procedural finish to discharge), and total cost of hospitalization; (2) major acute complications, including death, severe infection (pneumonia, systemic infection, and infectious endocarditis), or major bleeding that required blood transfusion, thrombosis, thromboembolism, hemolysis, thrombocytopenia, pleural diffusion, and pneumothorax, as well as echocardiographic ADO-related complications, including ADO-induced obstruction at the sides of the aortic arch and/or the left pulmonary artery, ADO displacement, or ADO dislodgment after release; (3) additional medical interventions, including blood transfusion and additional antibiotic use.
Postprocedural follow-up and 6-month outcomes. The postprocedural clinical follow-up was scheduled at 1 and 6 months. Thereafter, the follow-up was conducted yearly, with indexed echocardiography at 1 and 6 months, to record all clinical-cause death, infectious endocarditis, thrombosis and/or thromboembolism, hemolysis, and thrombocytopenia. The follow-up was intended to determine incomplete duct closure (caused by persistent residual shunting or PDA reopening), the ADO-induced obstruction at the sides of the aortic arch and/or the left pulmonary and ADO displacement or dislodgment, as well as to echocardiographically monitor the residual shunting and its related changes.
Definition of procedural success. Except for the clinical presentations, TTE with imaging modalities of 2DE, CDFI, and CW was employed to evaluate the results of device occlusion and the procedural success.
Incomplete closure was described as the existence of the persistent residuals or the reopening of the shunt, which could be postprocedurally detected by CDFI at discharge or during follow-up. The temporal residual shunting that automatically disappeared during the procedure was not considered as incomplete closure.
Initial success at discharge was defined as complete closure with neither residual shunting nor occluder-occupied effects. This phenomenon caused significant aortic arch deformation or pulmonary artery obstruction (CW-derived peak velocity ≤2.0 m/s at the obstructed site), or incomplete closure with residual shunting but no hemodynamic relevance (CDFI-derived shunting width ≤2.0 mm and/or CW-derived shunting peak velocity ≤2.0 m/s). The 6-month success was defined as the absence of persistent residual shunting, PDA reopening, and ADO dislodgment, or the satisfaction of initial success criteria.
Statistical analysis. Data were analyzed by using SPSS version 13.0 (SPSS, Inc). Continuous variables with normal distribution were expressed as mean ± SD; otherwise, they were expressed as the median. The Student’s t-test, χ2 or Fisher’s test, and the Mann-Whitney test were employed to compare the differences between groups for the continuous and non-continuous variables. P-values <.05 were considered statistically significant.
Results
Baseline characteristics. Patients in both groups had similar demographics and preoperative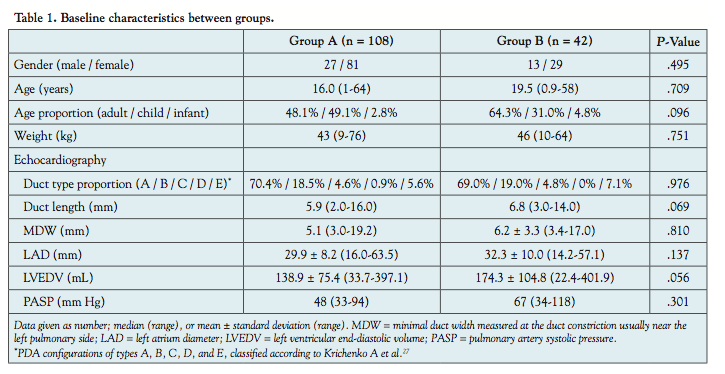 clinical characteristics, including their gender, age, age proportion, weight, duct size, duct length, Krichenko duct types,27 LAD, LVEDV, LVEF, and PASP (Table 1).
clinical characteristics, including their gender, age, age proportion, weight, duct size, duct length, Krichenko duct types,27 LAD, LVEDV, LVEF, and PASP (Table 1).
Immediate outcome and major acute complications. Similar rates were observed for initial success (98.2% vs 100%; P>.05) and 6-month success (99.1% vs 100%; P>.05) in group A and group B, respectively. Group A had fewer major acute complications (3.7% vs 85.7%; P<.001), as well as shorter operating time (1.3 hours vs 2.1 hours; P<.001), ICU stay (0 hours vs 23.0 hours; P<.001), and recovery time (3.8 days vs 9.5 days; P<.001). Furthermore, group A featured lower rates of general anesthesia (36.1% vs 100%; P<.001), blood transfusion (0.9% vs 71.4%; P<.001), and extra use of antibiotics (27.8% vs 78.6%; P<.001), as well as lower total cost of hospitalization ($3519 vs $5730; P<.001) (Table 2).
Clinical follow-up and 6-month outcomes. Both groups had demonstrated the stable initial success of duct occlusion with no major chronic complications based on the follow-up after 6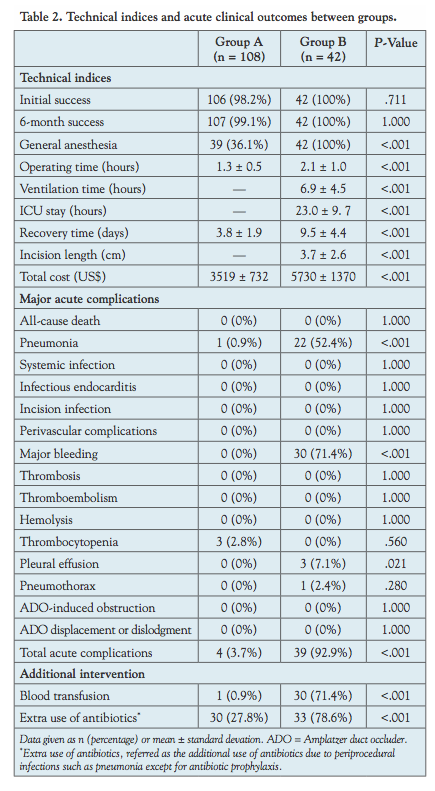 months. Echocardiography showed no ADO dislodgment or duct reopening. The initial mild (no hemodynamic relevance) ADO-induced pulmonary artery obstruction in 5 patients in group A and 3 patients in group B remained unchanged. Postprocedural residual shunting was observed in 6 patients from group A, but these had disappeared upon discharge in 4 of these patients and after 6 months in 1 other patient. The remaining patients remained unchanged after 6 months (with a shunting width of approximately 3 mm). The residual shunting detected in 3 patients from group B was eventually lost during hospitalization or upon discharge (Table 3).
months. Echocardiography showed no ADO dislodgment or duct reopening. The initial mild (no hemodynamic relevance) ADO-induced pulmonary artery obstruction in 5 patients in group A and 3 patients in group B remained unchanged. Postprocedural residual shunting was observed in 6 patients from group A, but these had disappeared upon discharge in 4 of these patients and after 6 months in 1 other patient. The remaining patients remained unchanged after 6 months (with a shunting width of approximately 3 mm). The residual shunting detected in 3 patients from group B was eventually lost during hospitalization or upon discharge (Table 3).
Discussion
Duct closure techniques have evolved since the first report on surgical ligation by Gross and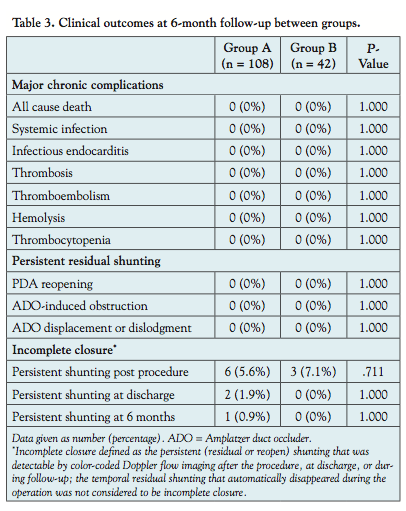 Hubbard in 1939.28 Transcatheter methods with a conical Ivalon plug to avoid thoracotomy were pioneered in 1967 by Portsmann et al.29 Rashkind et al later introduced the use of an umbrella-type in 1979.30 However, these devices were too large, thereby requiring large introducer sheaths that frequently left residual shunting. Upon the introduction of Gianturco coils in 1992,31 transcatheter coil occlusion became a broadly used technique for the closure of small-to-moderate PDAs. Subsequently, devices such as the ADO were developed; these devices allow transcatheter approaches to moderate and large PDAs amenable to occlusion.32 Along with the evolution of transcatheter techniques, various modified surgical methods, such as axillary vertical incision thoracotomy with ductal ligation10 and video-assisted thoracoscopic clipping have been developed.10,12-15 Despite the decreased invasion and increased cosmetic benefits associated with these surgical methods, they have drawbacks, such as procedural complexity, unstable safety, permanent scarring, prolonged hospital stay, postoperative pain, and other associated morbidities.5-7
Hubbard in 1939.28 Transcatheter methods with a conical Ivalon plug to avoid thoracotomy were pioneered in 1967 by Portsmann et al.29 Rashkind et al later introduced the use of an umbrella-type in 1979.30 However, these devices were too large, thereby requiring large introducer sheaths that frequently left residual shunting. Upon the introduction of Gianturco coils in 1992,31 transcatheter coil occlusion became a broadly used technique for the closure of small-to-moderate PDAs. Subsequently, devices such as the ADO were developed; these devices allow transcatheter approaches to moderate and large PDAs amenable to occlusion.32 Along with the evolution of transcatheter techniques, various modified surgical methods, such as axillary vertical incision thoracotomy with ductal ligation10 and video-assisted thoracoscopic clipping have been developed.10,12-15 Despite the decreased invasion and increased cosmetic benefits associated with these surgical methods, they have drawbacks, such as procedural complexity, unstable safety, permanent scarring, prolonged hospital stay, postoperative pain, and other associated morbidities.5-7
Transthoracic per-pulmonary catheter-based device closure of PDA is a novel minimally invasive surgical technique.26 This procedure is conducted through a parasternal mini incision (2-3 cm) made in the left second intercostal space. A specially designed delivery sheath loaded with the ADO was inserted through the purse-string sutures into the pulmonary trunk. The device was advanced through the PDA and into the descending aorta under transesophageal echocardiographic guidance, before the ADO was deployed. The initial results showed that the per-pulmonary device closure of a PDA was simple, safe, and effective, with the advantages of more accurate device positioning and reduced risk of device dislocation using stay sutures.
In our study, the transthoracic per-pulmonary catheter-based device closure had more major acute complications, as well as longer time of operation, ICU stay, and recovery, as compared with the transvenous approach. Despite the similar rates of initial and 6-month success between groups, the transthoracic approach had higher rates of general anesthesia and blood transfusion, as well as extra use of antibiotics and higher total cost of hospitalization. Additionally, the transvenous approach did not require a parasternal incision, which could lead to scar formation and cosmetic or psychological effects.
In this study, we used a novel method for transcatheter duct closure to further simplify the procedure. Except for brief fluoroscopy to create the device delivery track, the entire procedure was guided mainly by TTE. Briefly, TTE with imaging modalities of 2DE, CDFI, and CW was used during the procedure to carefully evaluate the duct size, length, and anatomical characteristics for selecting the appropriate ADO, to continuously monitor the residual shunting and its changes, to visualize the recovery of the ADO memorized configuration, and to decide whether a selected occluder should be replaced or not prior to release (as a result of incorrect size or significant residual shunting). Echocardiography was used as an alternative to aortic angiography for choosing a suitable occluder, continuously monitoring the residual shunting and detecting the ADO-induced aortic pulmonary artery obstruction. Thus, femoral artery puncture and aortic angiography, which were necessary for conventional transcatheter duct closure, could be neglected in this case. The procedure for transcatheter duct closure was simplified and the potential procedural risks were reduced, as reported in our previous study25 and as evidenced in this study by the shorter procedure time, less x-ray exposure and radiation without contrast agent injection, and decreased contrast-induced toxicity, as well as lower rates of general anesthesia and procedure-related complications, particularly for PDA closure in small children, infants, or neonates.
Study limitations. This study has several limitations. Regardless of the similarity in the baseline characteristics between groups, our study was not randomly designed, and bias could not be completely avoided. First, the operators in our center were at the initial stages of learning how to use the transthoracic approach for duct closure, whereas the transvenous approach has been used for over 10 years. Second, the transthoracic approach could provide a fixed suture when closing a large PDA by tying the device down with purse-string sutures to avoid device dislocation. However, our study excluded patients with true window-type PDA. Thus, other benefits of transthoracic approach might have been excluded from our results.
Conclusions
Despite similar efficacy for duct closure with ADO, the transvenous approach is associated with fewer acute complications, more periprocedural comfort, and lower cost; thus the transthoracic approach should not be reasonable for duct closure except for particular indications.
References
- Kitterman JA, Edmunds LJ, Gregory GA, Heymann MA, Tooley WH, Rudolph AM. Patent ducts arteriosus in premature infants. Incidence, relation to pulmonary disease and management. N Engl J Med. 1972;287(10):473-477.
- Chen JY. Patent ductus arteriosus in preterm infants. Pediatr Neonatol. 2012;53(5):275.
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39(12):1890-1900.
- Mavroudis C, Backer CL, Gevitz M. Forty-six years of patient ductus arteriosus division at Children’s Memorial Hospital of Chicago. Standards for comparison. Ann Surg. 1994;220(3):402-410.
- Cherup LL, Siewers RD, Futrell JW. Breast and pectoral muscle maldevelopment after anterolateral and posterolateral thoracotomies in children. Ann Thorac Surg. 1986;41(5):492-497.
- Seghaye MC, Grabitz RG, Alzen G, et al. Thoracic sequelae after surgical closure of the patent ductus arteriosus in premature infants. Acta Paediatr. 1997;86(2):213-216.
- Bal S, Elshershari H, Celiker R, Celiker A. Thoracic sequels after thoracotomies in children with congenital cardiac disease. Cardiol Young. 2003;13(3):264-267.
- Giroud JM, Jacobs JP. Evolution of strategies for management of the patent arterial duct. Cardiol Young. 2007;17(Suppl 2):68-74.
- Kan CD, Luo CY, Yang YJ. Application of pusher in mini-invasive patent ductus arteriosus ligation. J Card Surg. 2001;16(3):252-254.
- Kyoku I, Yokota M, Kitano M, et al. Axillary vertical incision thoracotomy sparing pectoralis major muscle and latissimus dorsi muscle: an approach for patent ductus arteriosus. Kyobu Geka. 1989;42(5):371-373.
- Shu Q, Zhang Z, Zhu X, et al. Transaxillary minithoracotomy in intrathoracic surgery for 316 infants and children. Chin Med J. 2003;116(7):1008-1010.
- Laborde F, Noirhomme P, Karam J, Batisse A, Bourel P, Saint MO. A new video-assisted thoracoscopic surgical technique for interruption of patient ductus arteriosus in infants and children. J Thorac Cardiovasc Surg. 1993;105(2):278-280.
- Vida VL, Rubino M, Bottio T, et al. Thoracoscopic closure of the patent arterial duct. Cardiol Young. 2004;14(2):164-167.
- Nezafati MH, Soltani G, Vedadian A. Video-assisted ductal closure with new modifications: minimally invasive, maximally effective, 1,300 cases. Ann Thorac Surg. 2007;84(4):1343-1348.
- Vanamo K, Berg E, Kokki H, Tikanoja T. Video-assisted thoracoscopic versus open surgery for persistent ductus arteriosus. J Pediatr Surg. 2006;41(7):1226-1229.
- Faella HJ, Hijazi ZM. Closure of the patent ductus arteriosus with the Amplatzer PDA device: immediate results of the international clinical trial. Catheter Cardiovasc Interv. 2000;51(1):50-54.
- Chen HY, Weng GX, Chen ZQ, et al. Comparison of long-term clinical outcomes and costs between video-assisted thoracoscopic surgery and transcatheter Amplatzer occlusion of the patent ductus arteriosus. Pediatr Cardiol. 2012;33(2):316-321.
- Choi DY, Kim NY, Jung MJ, Kim SH. The results of transcatheter occlusion of patent ductus arteriosus: success rate and complications over 12 years in a single center. Korean Circ J. 2010;40(5):230-234.
- Bridges ND, Perry SB, Parness I, Keane JF, Lock JE. Transcatheter closure of a large patent ductus arteriosus with the clamshell septal umbrella. J Am Coll Cardiol. 1991;18(5):1297-1302.
- Latson LA, Hofschire PJ, Kugler JD, Cheatham JP, Gumbiner CH, Danford DA. Transcatheter closure of patent ductus arteriosus in pediatric patients. J Pediatr. 1989;115(4):549-553.
- Stokhof AA, Sreeram N, Wolvekamp WT. Transcatheter closure of patent ductus arteriosus using occluding spring coils. J Vet Intern Med. 2000;14(4):452-455.
- Magee AG, Huggon IC, Seed PT, Qureshi SA, Tynan M. Transcatheter coil occlusion of the arterial duct; results of the European Registry. Eur Heart J. 2001;22(19):1817-1821.
- Lloyd TR, Fedderly R, Mendelsohn AM, Sandhu SK, Beekman RR. Transcatheter occlusion of patent ductus arteriosus with Gianturco coils. Circulation. 1993;88(4 Pt 1):1412-1420.
- Hosking MC, Benson LN, Musewe N, Dyck JD, Freedom RM. Transcatheter occlusion of the persistently patent ductus arteriosus. Forty-month follow-up and prevalence of residual shunting. Circulation. 1991;84(6):2313-2317.
- Chen LL, Lin CG, Peng YF, et al. A new simplified catheter technique for the occlusion of patent ductus arteriosus. Chin J Interv Cardiol. 2007;15(1):41.
- Li HX, Guo WB, Zhu M, et al. New minimally invasive technique of perpulmonary device closure of patent ductus arteriosus through a parasternal approach. Ann Thorac Surg. 2012;93(3):862-868.
- Krichenko A, Benson LN, Burrows P, et al. Angiographic classification of the isolated, persistently patent ductus arteriosus and implications for percutaneous catheter occlusion. Am J Cardiol. 1989;63(12):877-880.
- Gross RE, Hubbard JP. Surgical ligation of a patent ductus arteriosus. Report of first successful case. JAMA. 1939;112(8):729-731.
- Porstmann W, Wierny L, Warnke H. Closure of persistent ductus arteriosus without thoracotomy. Ger Med Mon. 1967;12(6):259-261.
- Rashkind WJ, Mullins CE, Hellenbrand WE, Tait MA. Nonsurgical closure of patent ductus arteriosus: clinical application of the Rashkind PDA Occluder System. Circulation. 1987;75(3):583-592.
- Cambier PA, Kirby WC, Wortham DC, Moore JW. Percutaneous closure of the small (less than 2.5 mm) patent ductus arteriosus using coil embolization. Am J Cardiol. 1992;69(8):815-816.
- Masura J, Walsh KP, Thanopoulous B, et al. Catheter closure of moderate- to large-sized patent ductus arteriosus using the new Amplatzer duct occluder: immediate and short-term results. J Am Coll Cardiol. 1998;31(4):878-882.
From the 1Fujian Institute of Coronary Heart Disease, Fuzhou, P. R. China, the 2Department of Cardiology, Fujian Medical University Union Hospital, Fuzhou, P. R. China, and the 3Department of Cardiovascular Surgery, Fujian Medical University Union Hospital, Fuzhou, P. R. China.
Funding: This study was supported by the Key Program for Scientific Research of Fujian Medical University (Grant No. 09ZD011).
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. The authors report no conflicts of interest regarding the content herein.
Manuscript submitted April 1, 2013, provisional acceptance given May 28, 2013, final version accepted June 26, 2013.
Address for correspondence: Prof. Liang-long Chen, Department of Cardiology, Fujian Medical University Union Hospital, 29 Xin-Quan Road, Fuzhou, 350001, Fujian, P. R. China. Email: lianglongchenxh@126.com









