

Conservative Management of an Epicardial Collateral Perforation During Retrograde Chronic Total Occlusion Percutaneous Coronary Intervention
Abstract: Coronary artery perforation is a highly feared complication of chronic total occlusion (CTO) percutaneous coronary intervention (PCI) and can lead to pericardial effusion, tamponade, and, rarely, emergent cardiac surgery. Perforation of epicardial collaterals during retrograde CTO-PCI may be particularly challenging to treat, as embolization from both sides of the perforation may be required to control the bleeding. However, conservative measures can occasionally be effective. We present a case of epicardial collateral vessel perforation that was managed conservatively with anticoagulation reversal.
J INVASIVE CARDIOL 2016;28(1):E11-E12
Key words: percutaneous coronary intervention, surgery, bridging, complications, outcomes
________________________________________
Coronary artery perforation is a highly feared complication of chronic total occlusion (CTO) percutaneous coronary intervention (PCI) and can lead to pericardial effusion, tamponade, and, rarely, emergent cardiac surgery. Perforation of epicardial collaterals during retrograde CTO-PCI may be particularly challenging to treat, as embolization from both sides of the perforation may be required to control the bleeding.1 Thrombin injection has been recently proposed as a safe and effective treatment of this complication.2 However, conservative measures may occasionally be effective. We report a case of epicardial collateral vessel perforation that was managed conservatively with anticoagulation reversal.
Case Report
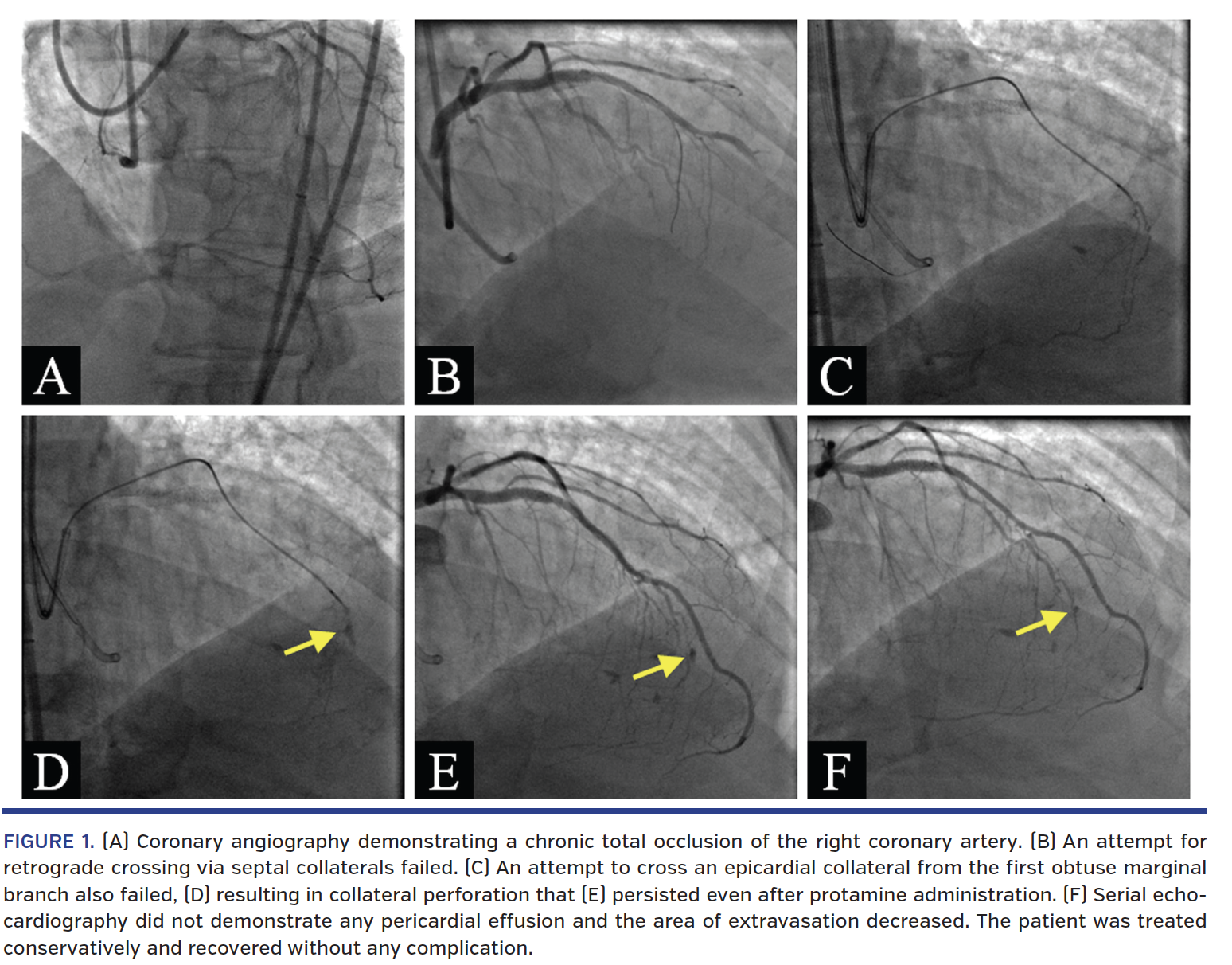
A 69-year-old man presenting with dyspnea on exertion was found to have a CTO of the right coronary artery (Figure 1A) and was referred for PCI. After failure of antegrade crossing and retrograde crossing via septal collaterals, retrograde wiring through an epicardial collateral originating from the first obtuse marginal artery was attempted (Figure 1B). The collateral could not be crossed due to severe tortuosity (Figure 1C) and collateral perforation occurred (Figure 1D, arrow). The patient remained hemodynamically stable. Anticoagulation was reversed with protamine, but angiography continued to demonstrate contrast staining (Figure 1E, arrow). However, several transthoracic echocardiograms performed during the course of an hour did not reveal pericardial effusion. The patient remained hemodynamically stable and repeat angiography demonstrated decrease in contrast staining at the perforation site without any pericardial effusion (Figure 1F, arrow). No further intervention was performed. Repeat echocardiography the following day did not demonstrate any pericardial effusion and the patient had an uneventful recovery.
Discussion
Our case demonstrates that epicardial collateral perforations during CTO-PCI may occasionally be treated conservatively without embolization or other hemostatic measures apart from anticoagulation reversal.
The incidence of perforation during CTO-PCI is between 1.3%-13.6%,3-6 but its clinical significance is variable. In a meta-analysis by Patel et al, perforation occurred in 3.4% of cases, but tamponade developed in only 0.3%.4 In a Japanese CTO registry, approximately 75% of CTO-PCI perforations resolved with observation; however, 2.6% of all patients required intervention for a perforation.6
Coronary artery perforations are traditionally classified using the Ellis classification,7 which does not cover epicardial and septal collateral perforations.8 Septal collateral perforations are typically self-limited and require no treatment. Epicardial collateral perforations, on the other hand, have a higher risk of tamponade and are typically managed with anticoagulation reversal and coiling,1 with coils deployed on both sides of the perforation.8 Rarely, microcatheter advancement through the collateral vessel with or without application of suction may be sufficient to control bleeding.1,8 However, each of these methods involves deep vessel intubation with a large microcatheter, which may result in further complications. Thrombin injection through a small microcatheter has been recently shown to control epicardial collateral perforation as well.2
In the case described here, early identification of a perforation and reversal of anticoagulation with protamine was sufficient to control epicardial collateral perforation. Repeat echocardiography was a key part of the management in this case, as real-time monitoring for pericardial effusion was possible. Since no effusion was found and the patient remained hemodynamically stable, a watchful waiting approach was taken. Subsequent angiography revealed a reduction in the size of contrast staining and it was felt that the perforation had self-sealed.
In summary, some epicardial collateral vessel perforations may be managed conservatively with serial echocardiographic evaluation and watchful waiting. Further studies can assist in identifying angiographic characteristics to select patients for collateral vessel coiling or thrombin injection vs conservative management.
References
1. Brilakis ES, Karmpaliotis D, Patel V, Banerjee S. Complications of chronic total occlusion angioplasty. Interv Cardiol Clin. 2012;1:373-389.
2. Kotsia A, Brilakis E, Karmpaliotis D. Thrombin injection for sealing epicardial collateral perforation during chronic total occlusion percutaneous coronary interventions. J Invasive Cardiol. 2014;26:E124-E126.
3. Rathore S, Matsuo H, Terashima M, et al. Procedural and in-hospital outcomes after percutaneous coronary intervention for chronic total occlusions of coronary arteries 2002 to 2008. JACC Cardiovasc Interv. 2009;2:489-497.
4. Patel VG, Brayton KM, Tamayo A, et al. Angiographic success and procedural complications in patients undergoing percutaneous coronary chronic total occlusion interventions. JACC Cardiovasc Interv. 2013;6:128-136.
5. Karmpaliotis D, Michael TT, Brilakis ES, et al. Retrograde coronary chronic total occlusion revascularization. JACC Cardiovasc Interv. 2012;5:1273-1279.
6. Morino Y, Kimura T, Hayashi Y, et al. In-hospital outcomes of contemporary percutaneous coronary intervention in patients with chronic total occlusion. JACC Cardiovasc Interv. 2010;3:143-151.
7. Ellis SG, Ajluni S, Arnold AZ, et al. Increased coronary perforation in the new device era. Incidence, classification, management, and outcome. Circulation. 1994;90:2725-2730.
8. Brilakis E. Manual of Coronary Chronic Total Occlusion Interventions: A Step-by-Step Approach. Waltham, MA: Elsevier Science; 2013.
____________________________________________
From the VA North Texas Health Care System, Dallas, Texas and University of Texas Southwestern Medical School, Dallas, Texas.
Disclosure: The authors have completed and returned the ICMJE Form for Disclosure of Potential Conflicts of Interest. Dr Brilakis reports consulting/speaker honoraria from Abbott Vascular, Asahi Intecc, Boston Scientific, Elsevier, Somahlution, St. Jude Medical, and Terumo Corporation; research support from Boston Scientific and InfraRedx; spouse is employee of Medtronic. The remaining authors report no disclosures regarding the content herein.
Manuscript submitted September 2, 2014, final version accepted September 2, 2014.
Address for correspondence: Emmanouil S. Brilakis, MD, PhD, VA North Texas Health Care System, The University of Texas Southwestern Medical Center at Dallas, Division of Cardiology (111A), 4500 S. Lancaster Rd, Dallas, TX 75216. Email: esbrilakis@gmail.com










